 Videoendoscopic Swallowing Study (VESS)
Videoendoscopic Swallowing Study (VESS)
A method of evaluating a person’s swallowing ability by means of a video-documented physical examination, looking from inside the throat. Also called the fiberoptic endoscopic evaluation of swallowing (FEES). The videoendoscopic swallowing study (VESS) is to be distinguished from the videofluoroscopic swallowing study (VFSS), which is an x-ray-based assessment.
 How a VESS works
How a VESS works
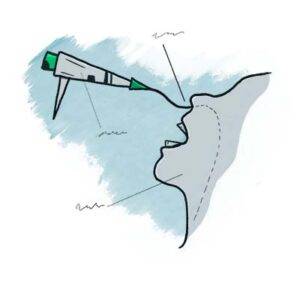
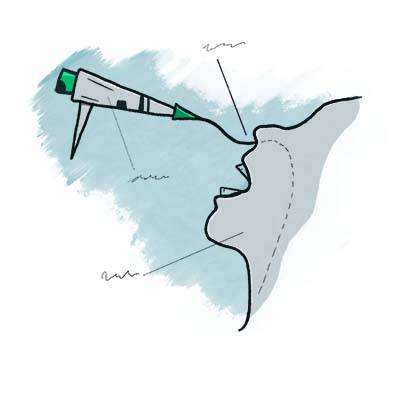
To perform a VESS, a clinician uses a fiberoptic or distal-chip nasolaryngoscope. The clinician begins by examining the structure and function of the patient’s palate, tongue, pharynx, and larynx, including sensation, if desired. Next, to assess the patient’s swallowing capabilities and limitations, the clinician positions the tip of the nasolaryngoscope just below the nasopharynx and, looking downward into the throat, asks the patient to swallow a series of colored substances with a range of consistencies (e.g., blue-stained water, blue-stained applesauce, and orange-colored crackers).
As the patient swallows these substances, the clinician watches to see if any significant traces remain in or reappear in the space above, around, or within the larynx, rather than disappearing into the entrance to the esophagus. If significant traces remain in view, or if any material spills into the opening of the larynx or down the trachea, the patient may have presbyphagia. If significant traces initially disappear but then re-emerge upward from the esophageal entrance, the patient may have cricopharyngeal dysfunction, with or without a Zenker’s diverticulum.
 Benefits of the videoendoscopic swallowing study
Benefits of the videoendoscopic swallowing study
This method has particular value for patients who are bedfast and cannot travel to the radiology suite, or for patients whose swallowing function is rapidly evolving (improving, usually), such as those recovering from a mild stroke. For clinicians experienced with this technique, VESS can also often be used with new patients complaining of dysphagia during the initial consultation as a robust and—depending on patient history—potentially stand-alone method of diagnosis and management.
Sometimes, the VESS findings, along with a patient history of solid food lodgment at the level of the cricoid cartilage or cricopharyngeus muscle, will indicate when VFSS should also be obtained to assess for possible cricopharyngeal dysfunction. Even in this latter circumstance, when VFSS is called upon to confirm a suspected diagnosis, VESS will have already oriented the examiner to the nature and severity of the problem. In most follow-up circumstances other than after cricopharyngeal myotomy, VESS is generally more efficient and inexpensive than VFSS.
VESS Assesses Equipment, Secretions, then Swallowing Ability
Part Ia: Palate elevates normally (1 of 7)
Part Ib: phonation (2 of 7)
Part Ic: High pitch elicited (3 of 7)
Part IIa: applesauce (4 of 7)
Part IIb: cracker (5 of 7)

Part IIb: continued (6 of 7)
Part IIc: water (7 of 7)
Dysphagia / Delayed Swallow Reflex
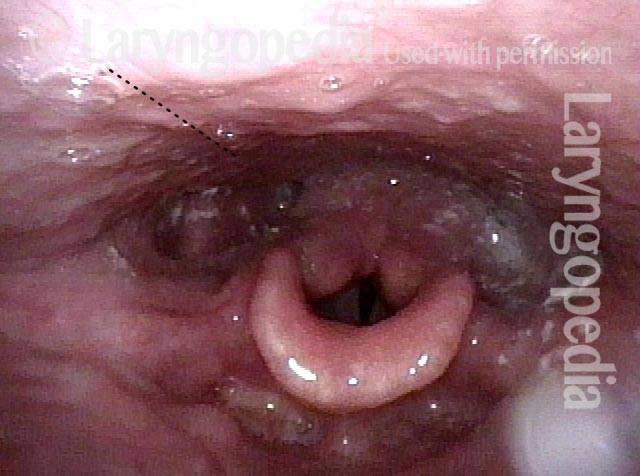
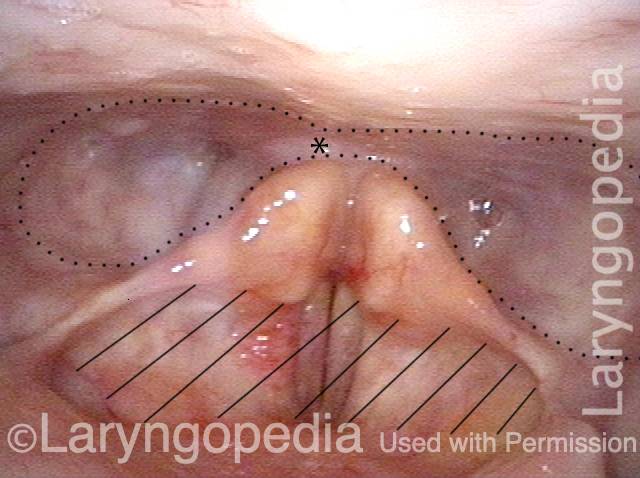
Laryngopharynx (1 of 3)
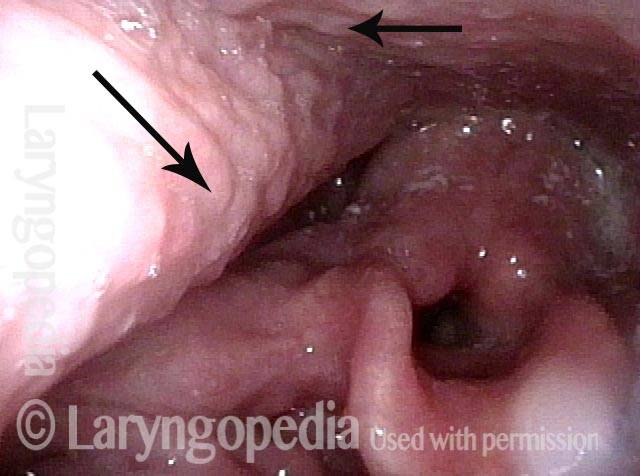
Dysphagia / Delayed swallow reflex (2 of 3)
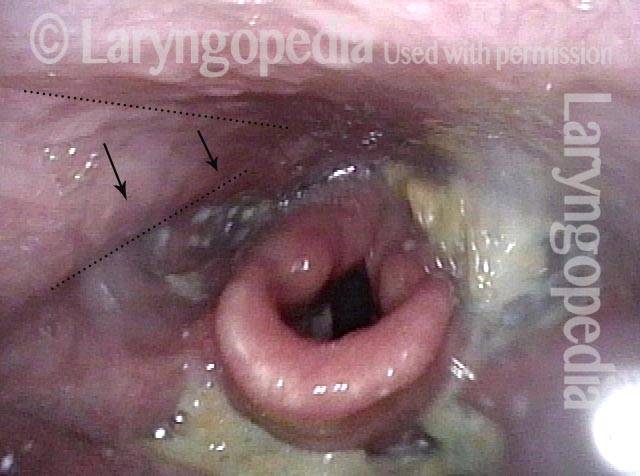
Hypopharyngeal pooling (3 of 3)
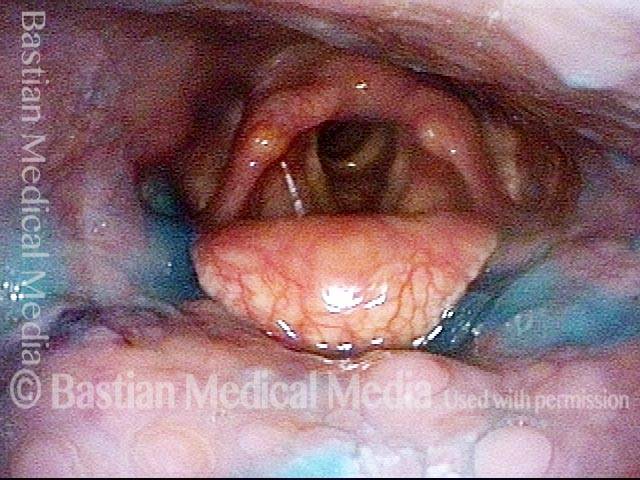
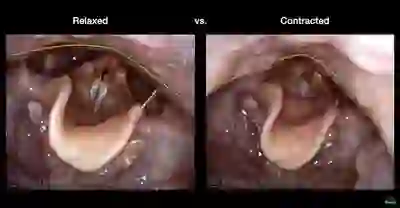
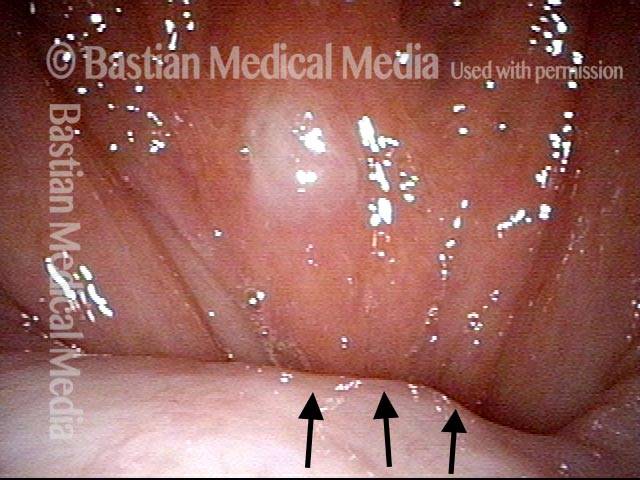
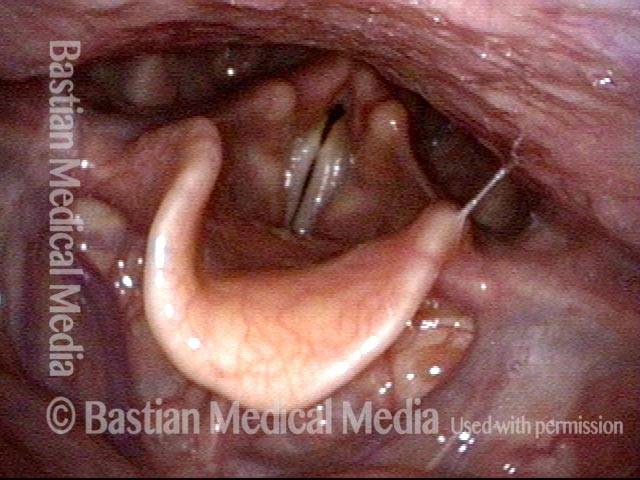
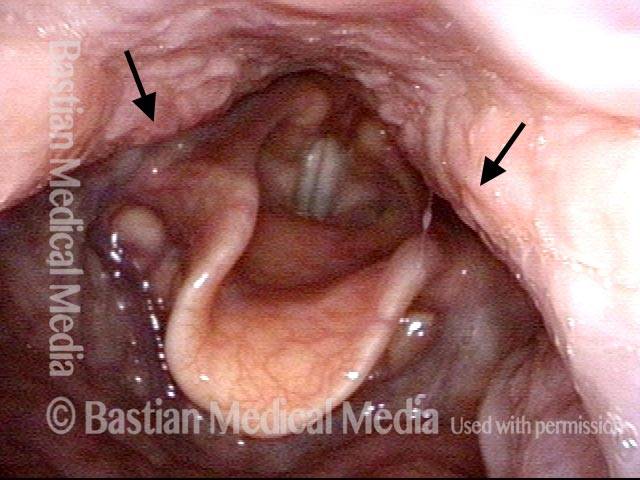
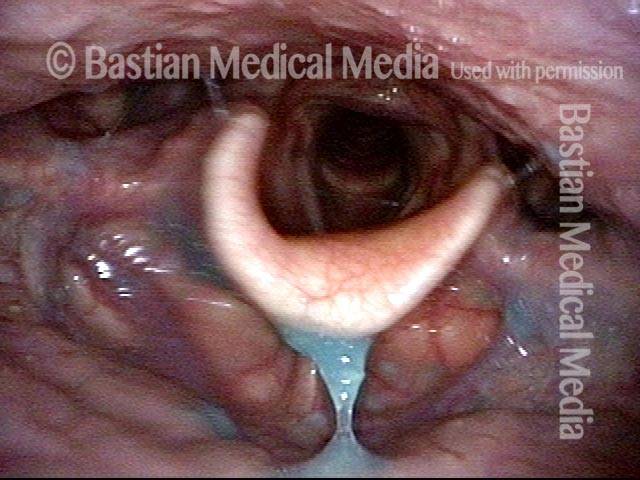
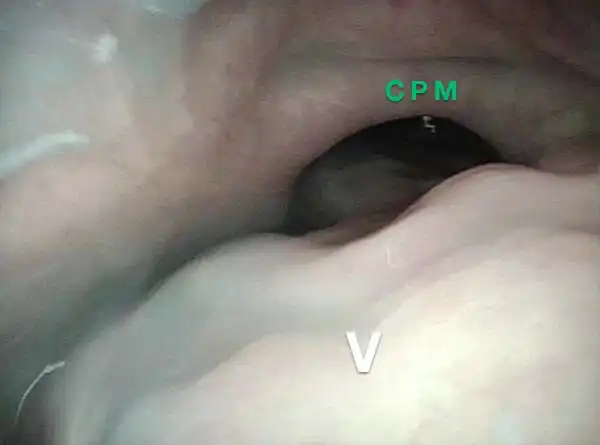
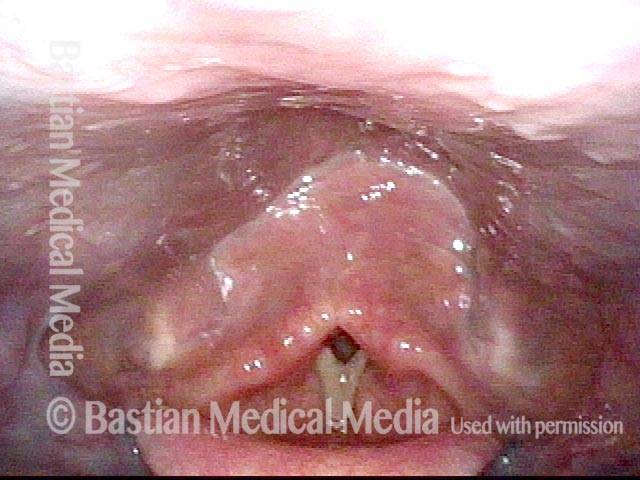
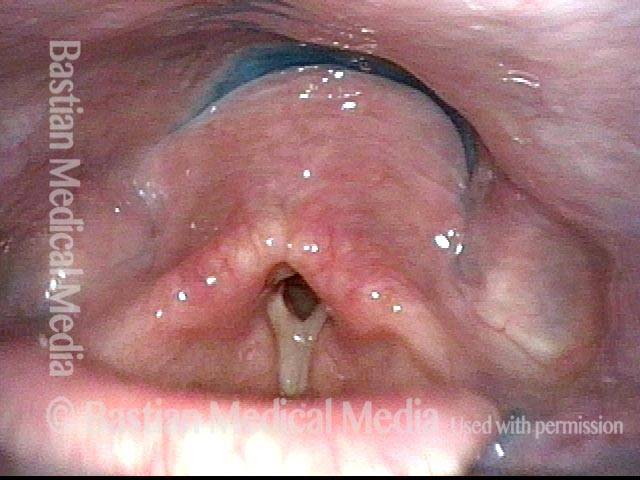
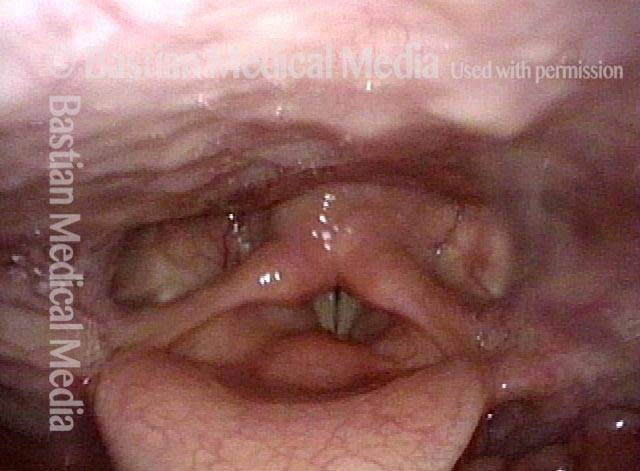
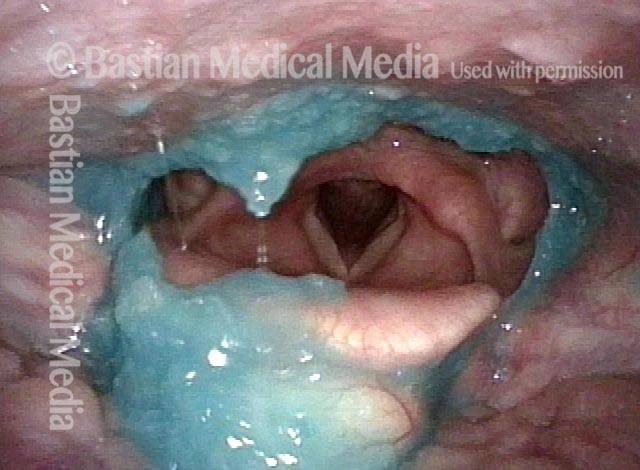
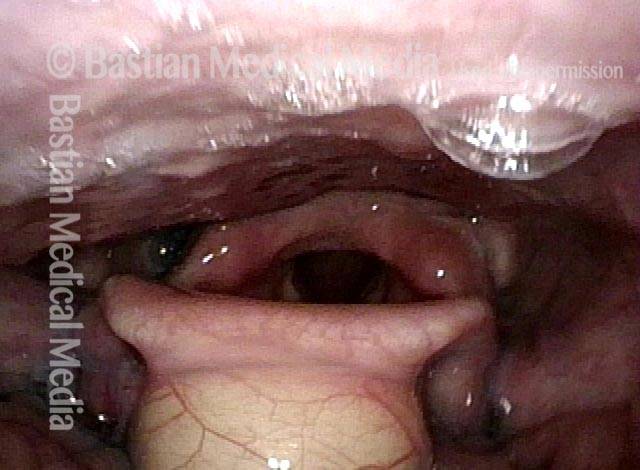
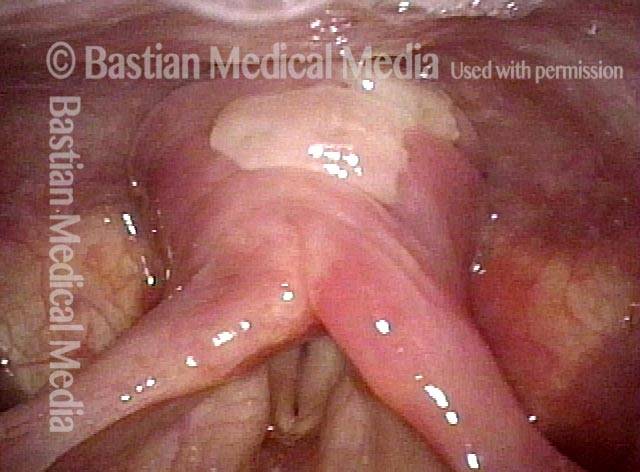
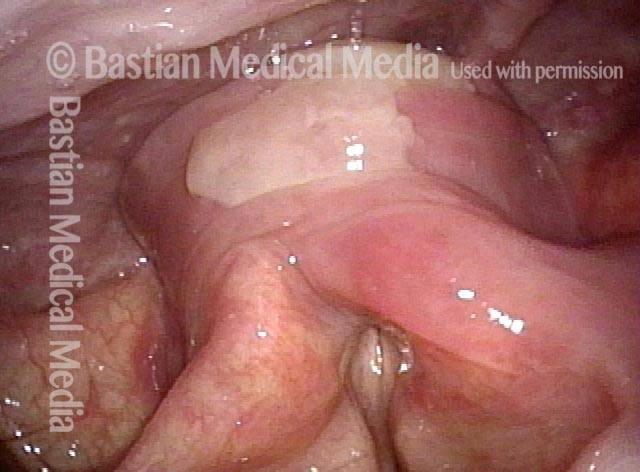
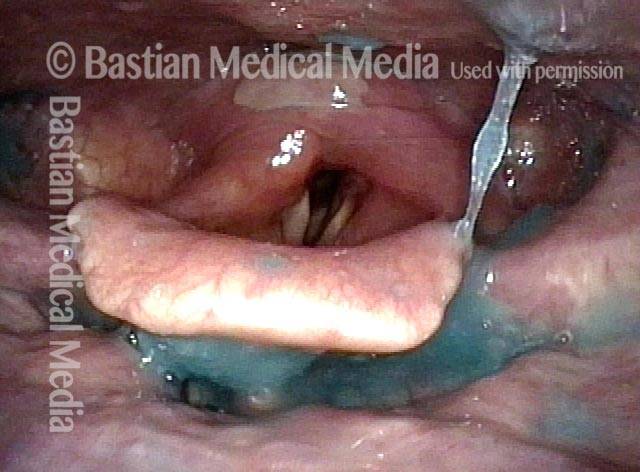
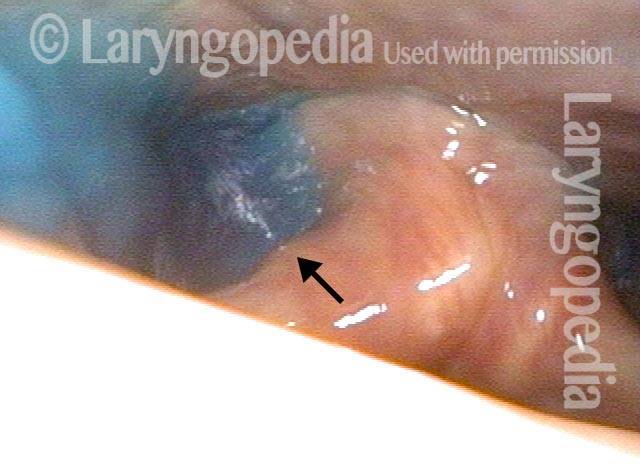
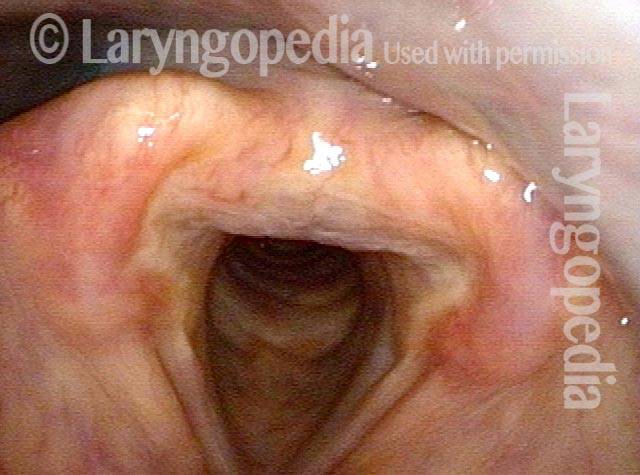
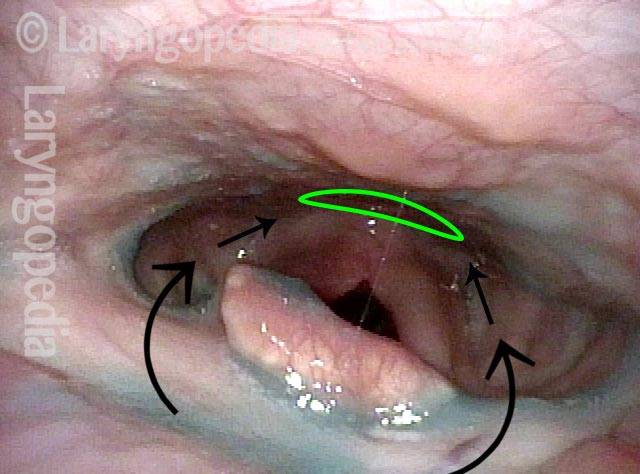
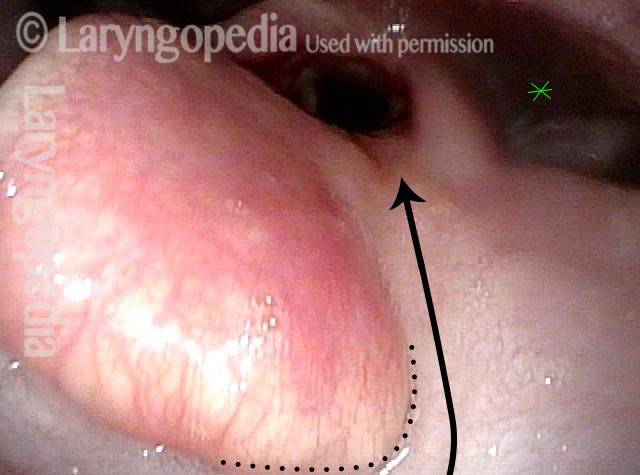
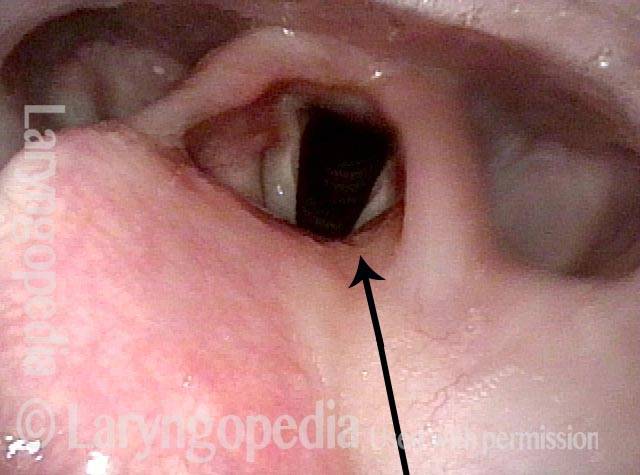
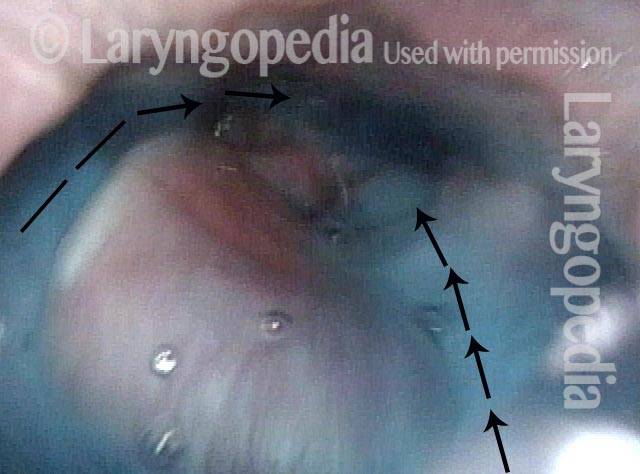
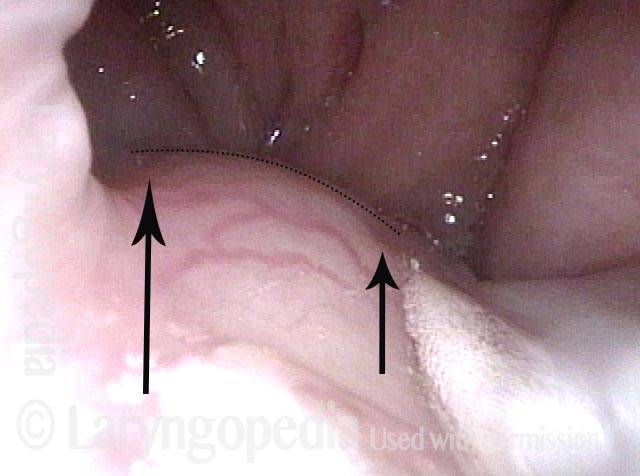
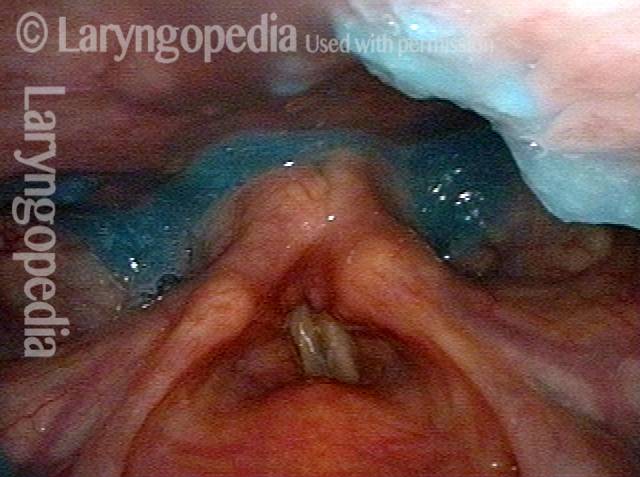
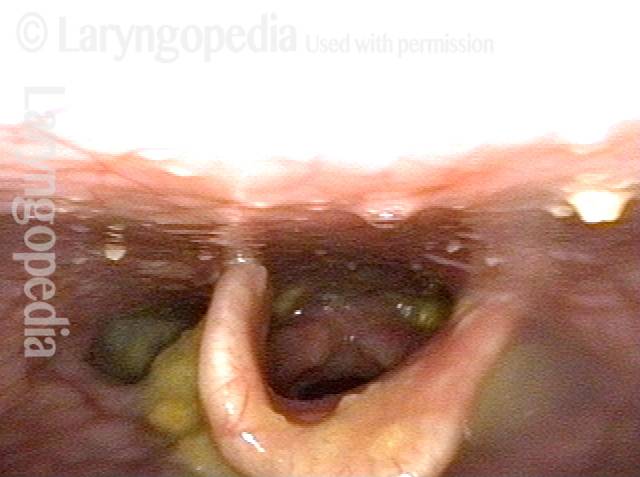
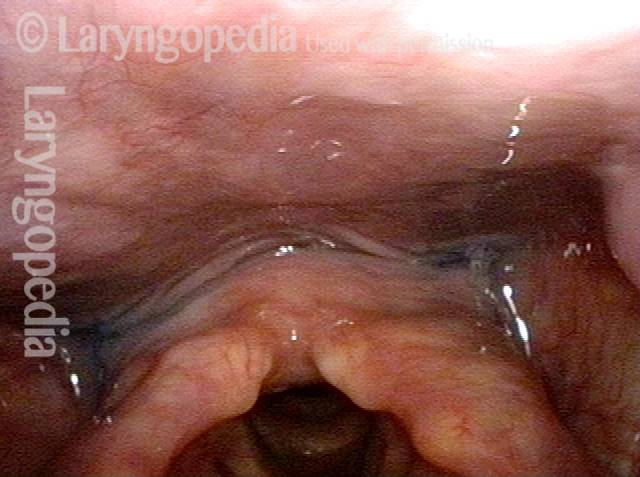
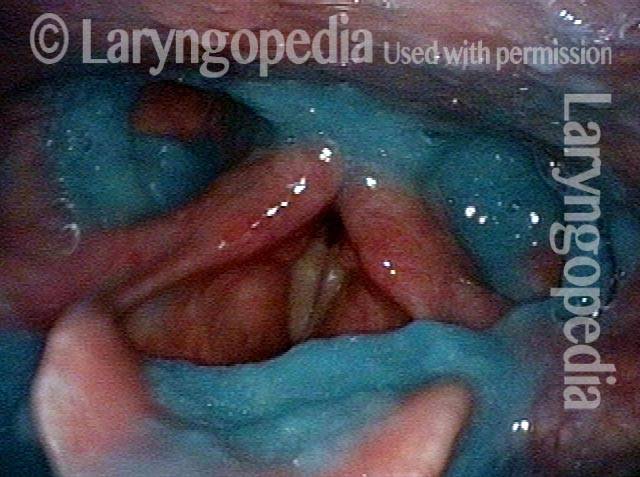
The Cricopharyngeus Muscle Seen During Swallowing
This person struggles to swallow due to a combination of prior tongue cancer surgery decades ago, and longterm radiation effects. Solid foods are the most problematic, and so this sequence shows an attempt to swallow water stained with blue food coloring.
Swallowing crescent (1 of 5)
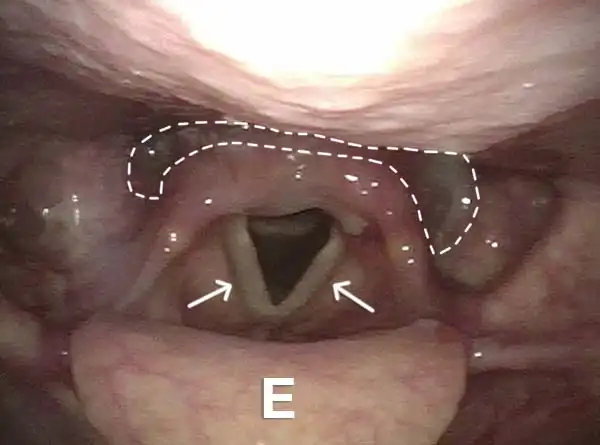
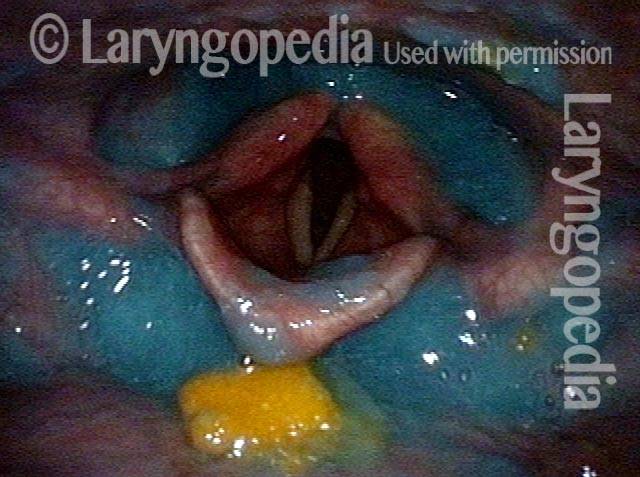
Swallowing water (2 of 5)
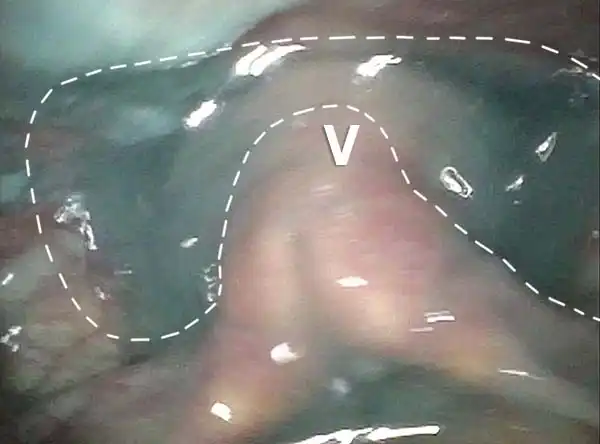
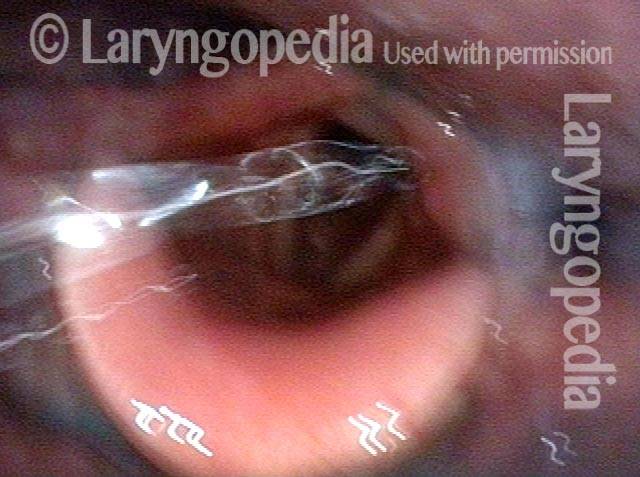
Cricopharyngeus muscle (3 of 5)
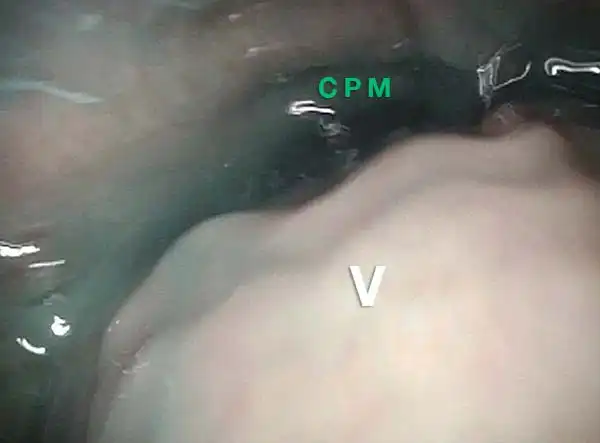
Relaxed CPM (4 of 5)

Partially open esophagus due to A-CPD (5 of 5)
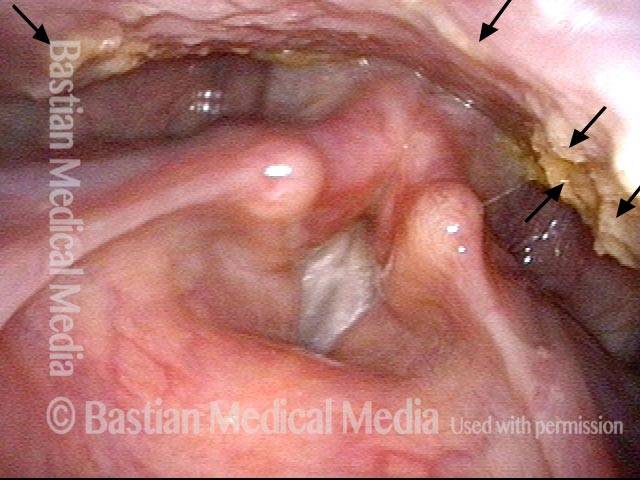
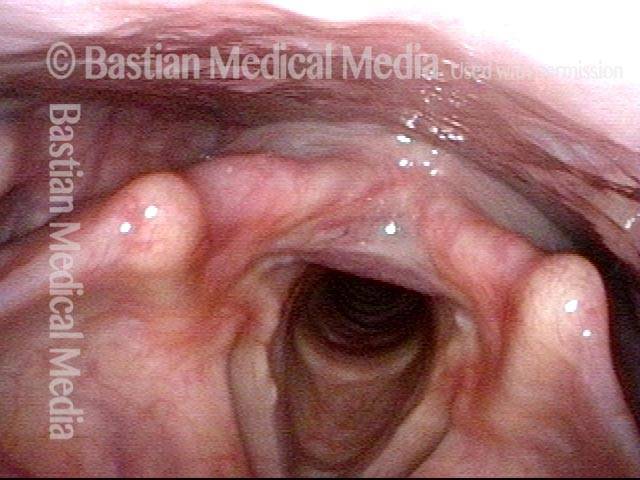
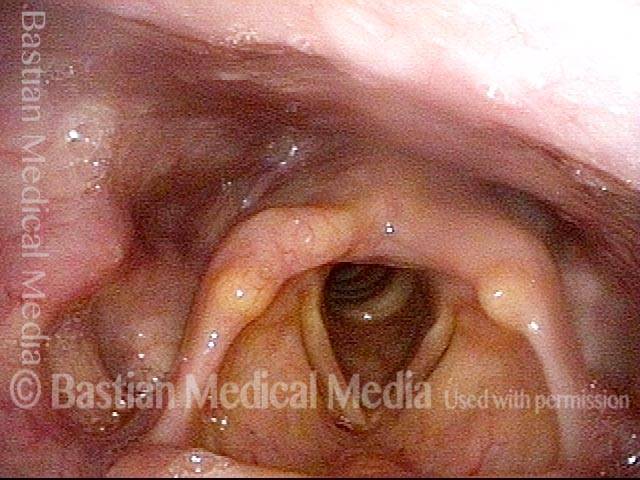
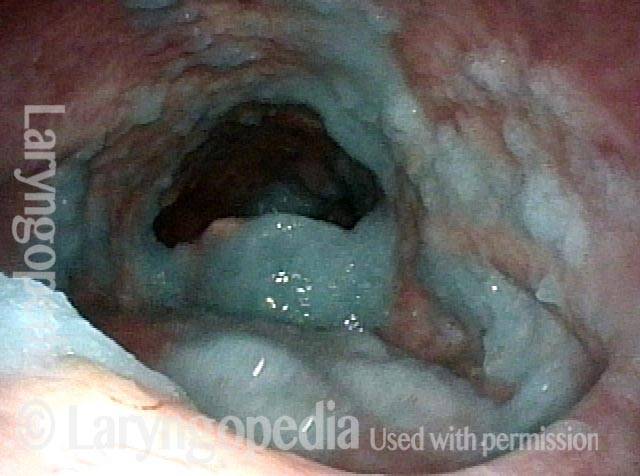
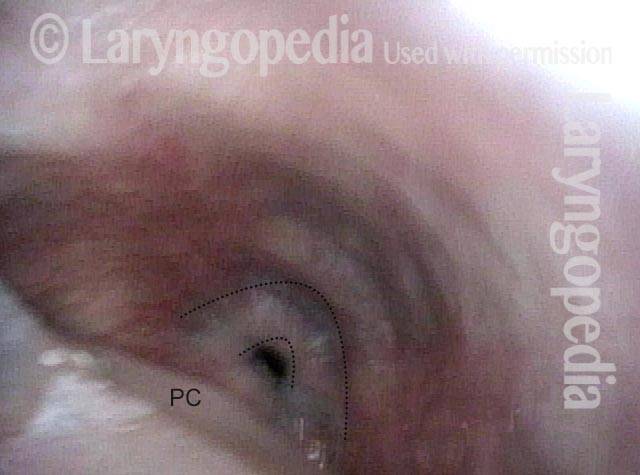
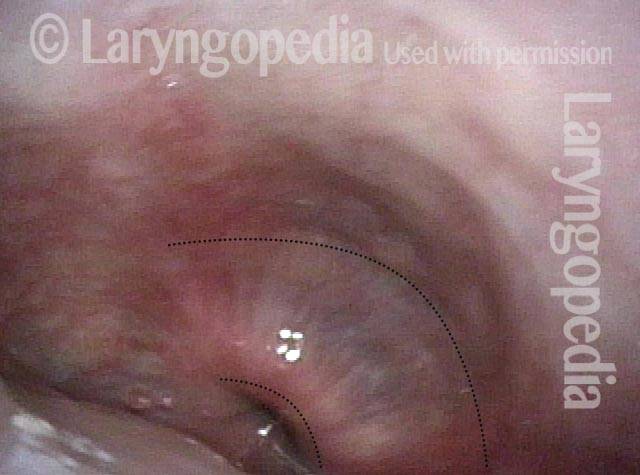
Zenker’s Diverticulum
Zenker’s diverticulum (1 of 3)

Postcricoid area (2 of 3)

Hypopharynx (3 of 3)

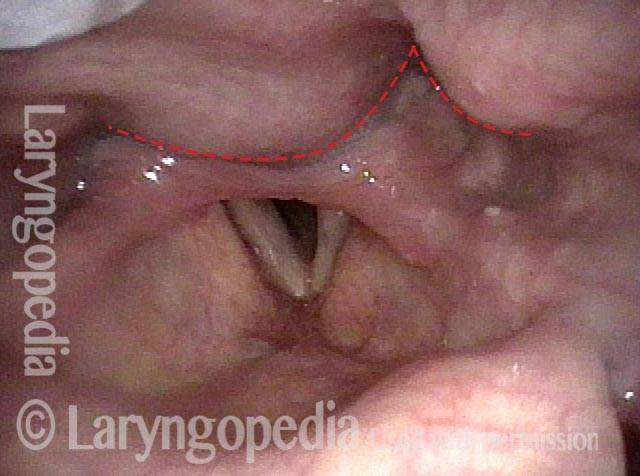
Reflux Into Hypopharynx, Characteristic of Cricopharyngeal Dysfunction
Reflux into hypopharynx (1 of 3)
Water flows into the swallowing crescent (2 of 3)
Larynx opens up (3 of 3)

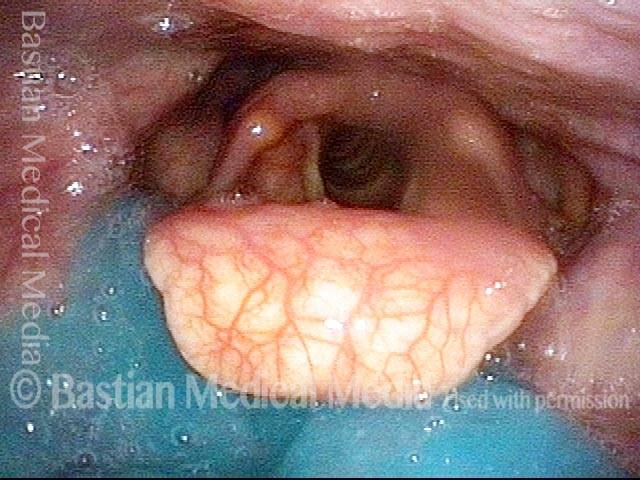
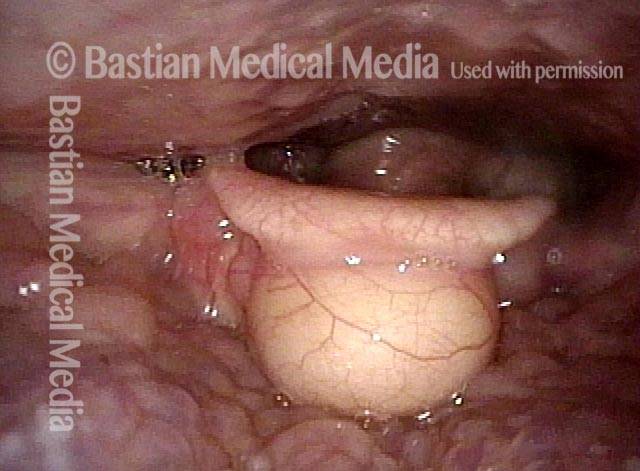
Vallecular Cysts don’t Disturb Swallowing—Except When They Do
Vallecular cyst (1 of 4)
Evaluation of function (2 of 4)
Applesauce residue (3 of 4)
Water wash (4 of 4)
Pill Lodgment Due to Swallowing Disability
Lodged pill (1 of 4)
Trumpet maneuver (2 of 4)
VESS (3 of 4)
Incomplete relaxation of CPD (4 of 4)

Delayed Swallow Reflex: Compare Blue Applesauce and Blue Water
VESS (1 of 4)

Delayed swallow reflex (2 of 4)

Blue-stained water (3 of 4)
No residue (4 of 4)
Scarring Diverts Swallowed Materials Directly into the Larynx
Post tonsillectomy (1 of 4)
Closer view (2 of 4)
The “chute” (3 of 4)
Abnormal diversion (4 of 4)
Skull Base Fracture and Vagus Nerve Injury—Note Pharynx Contraction and Impact on Swallowing
Palate branch of the vagus nerve (1 of 4)
Pharynx branch of the vagus nerve (2 of 4)
Damage to left vagal nerve function (3 of 4)
Residue during swallowing test (4 of 4)
VESS in 6 Still Photos
Assessing the patient’s swallowing (1 of 6)

Observing the pharynx (2 of 6)

Patient secretions (3 of 6)

Pooling of swallowed pureed food (4 of 6)
Swallowing solids (5 of 6)
Residue after foods (6 of 6)
VESS (Videoendoscopic Swallow Study) Findings after Radiotherapy
Narrowed pharyngeal wall (1 of 7)

Swallowing applesauce (2 of 7)
After sipping water (3 of 7)

Gravity aiding in swallowing (4 of 7)

Lifting larynx (5 of 7)
A closer look (6 of 7)
Gravity aiding again in swallowing (7 of 7)
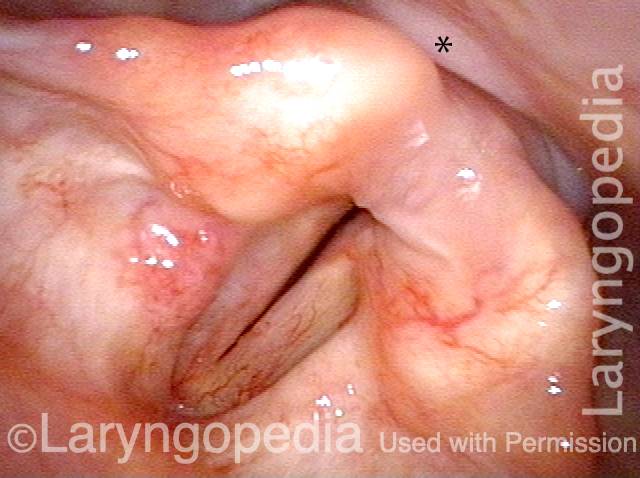
Cervical Osteophytes do not by Themselves Seem a Major Impediment to Swallowing
Protruding osteophytes (1 of 2)
Rapid swallowing (2 of 2)

Aspiration, and Fountain of Returned Aspirate after Coughing
Salivary pooling (1 of 5)

After applesauce (2 of 5)
After cheese cracker (3 of 5)
After water (4 of 5)
Cough expels the water from airway (5 of 5)

Three Views of the Entrance to the Esophagus from far Away to Close-up
Swallowing Crescent (1 of 3)
Closed esophagus (2 of 3)
Open Esophagus (3 of 3)