Long-Term Remission or even “cure” of RRP/Laryngeal Papilloma
Chronic hoarseness (1 of 6)
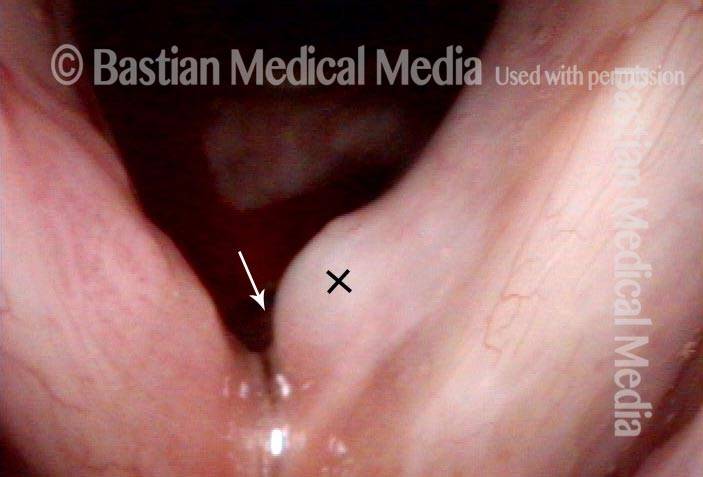
In this distant view, the nature of the abnormality of the right vocal cord (left of photo) is not well seen, and the lesion of the left posterior cord (right of photo) is subtle.
Narrow band light (2 of 6)
Under narrow band light, the two discrete lesions are better identified as being papillomas due to the punctate (dotted) vascular markings.

Higher magnification (3 of 6)
Again under standard light but at higher magnification.
Higher magnification, narrow band lighting (4 of 6)
Back to narrow band light, to more carefully scrutinize the anterior right vocal cord lesion (left of photo).

Post-operation (5 of 6)
18 months after surgical removal and cidofovir injection, voice is excellent and there is no sign of recurrent papilloma.

Post-operation, narrow band lighting (6 of 6)
Under narrow band light, no stippled vascularity is seen. The question is: is remission due to surgery, cidofovir, or the patient’s immune system?

RRP Cure? Or Just Long Term Remission?
Chronic hoarseness (1 of 4)
Chronic hoarseness, due to these papillomas, subsequently proven to be caused by subtype 6. Note HPV-effect vascularity.
4 months later (2 of 4)
A second surgery, 5 cidofovir injections (3 in office), and 4 months later, neither papilloma nor HPV vascular effect are seen here, under narrow band light.
8 months from start of treatment (3 of 4)
Now 8 months from the start of treatment, and 5 months since the final (office) cidofovir injection, there remains no evidence of abnormality. This view is under standard light.
Narrow band lighting (4 of 4)
An even closer view under narrow band light still shows no sign of HPV effect or papilloma. Voice is normal and vibratory flexibility is maintained when examined under strobe light.

What “Cured” this Case of RRP? Surgery? Cidofovir? The Patient’s Immune System? All Three?
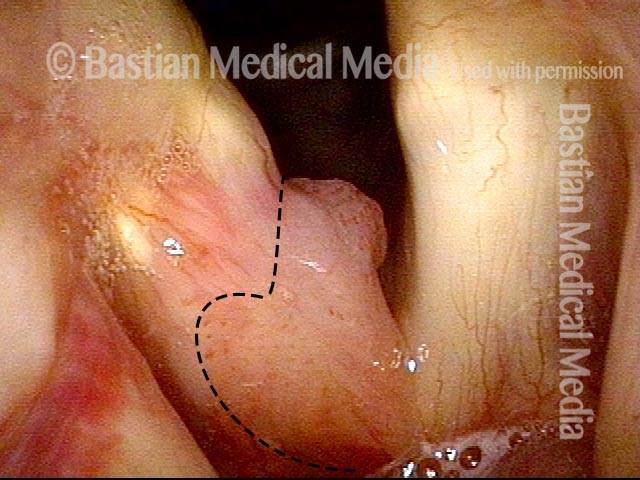
Papilloma (1 of 8)
Papilloma on right vocal cord (left of photo), proven by biopsy elsewhere. The disease has both a projecting component along with ‘carpet-variant’ component seen only via stippled vascular marks (within dashed line).
Stippling (2 of 8)
Closer view under strobe light; stippling is seen more clearly. Compare the stippling with the linear capillaries of the opposite cord.

One week after surgical removal (3 of 8)
One week after removal and sub typing (HPV 6) and cidofovir injection. Under narrow band light there is residual bruising but no significant stippling.

Cidofovir injection (4 of 8)
At final office-based cidofovir injection. Blood from the injection is seen, but still no stippling.
Six months after surgical removal (5 of 8)
Six months after removal, papillomas have recurred at the margin of the vocal cord, but not on its upper surface where linear capillaries have replaced stippling.
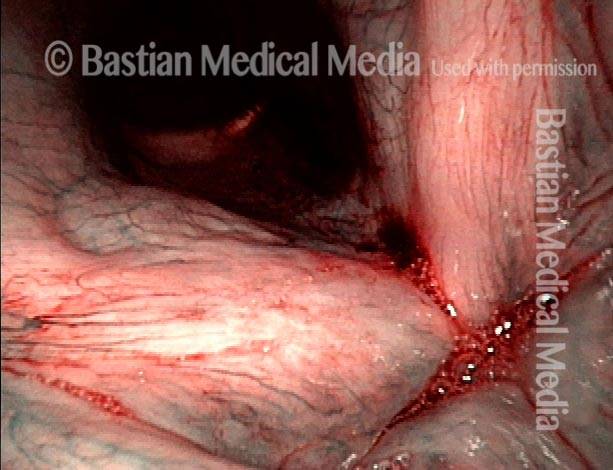
One week after second removal (6 of 8)
A week after second removal of papillomas and cidofovir injection, with expected inflammation, but no visible remaining stippled vascularity.
4 months later, healed (7 of 8)
4 months later, the vocal cord has long since healed and narrow band light is used to accentuate capillaries. No HPV effect (stippling) is seen.

3 years later, no sign of papilloma (8 of 8)
3 years later, there is still no sign of papilloma or stippled vascularity (HPV effect).
Humility Before the HPV Virus—A Recurrence of Papillomas at Ten Years
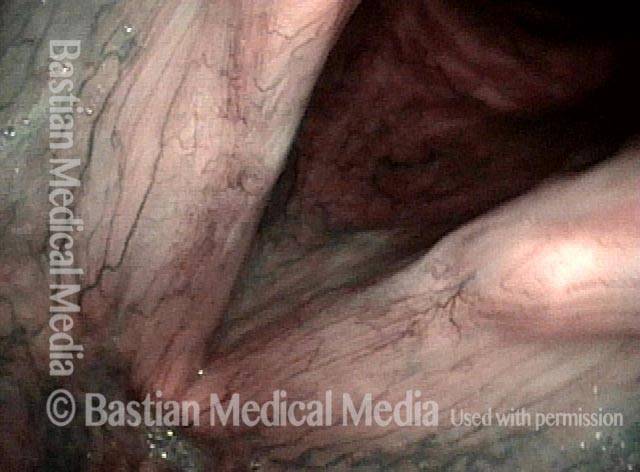
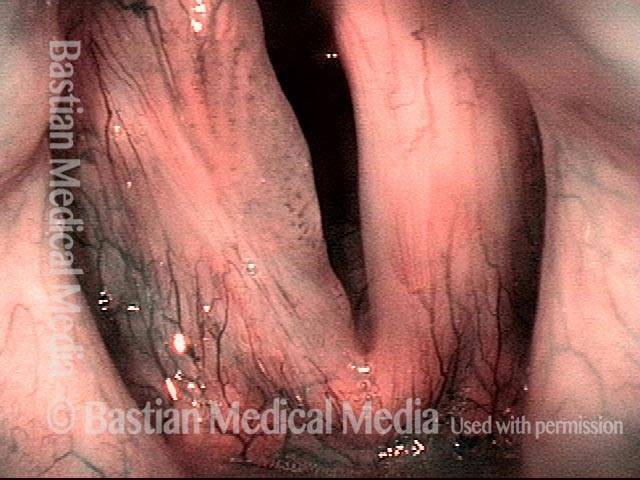
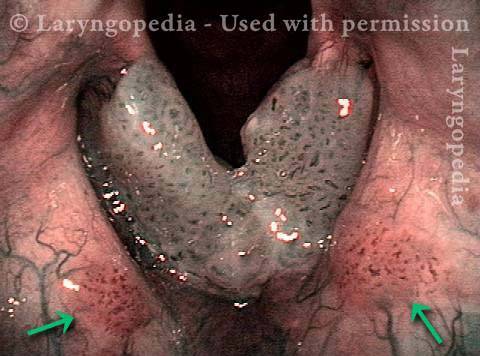
Stippled Vascularity (1 of 8)
In a somewhat distant view from 10 years earlier, under standard light, both vocal cords appear to be covered with stippled rather than (normal) linear or curvilinear vascularity. The diagnosis (biopsy confirmed): laryngeal papillomatosis aka RRP (recurrent respiratory papillomatosis), type 6.
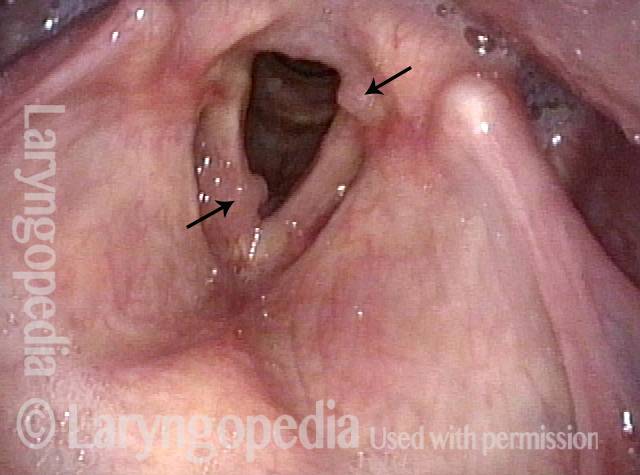
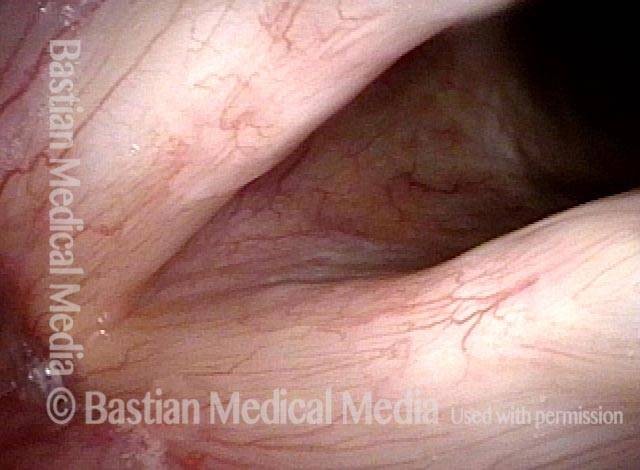
HPV infection (2 of 8)
A somewhat closer view under blue-green narrow band light accentuates the stippled vascularity so typical of HPV infection. Both true cords are covered and there are patches on the false cords (arrows).
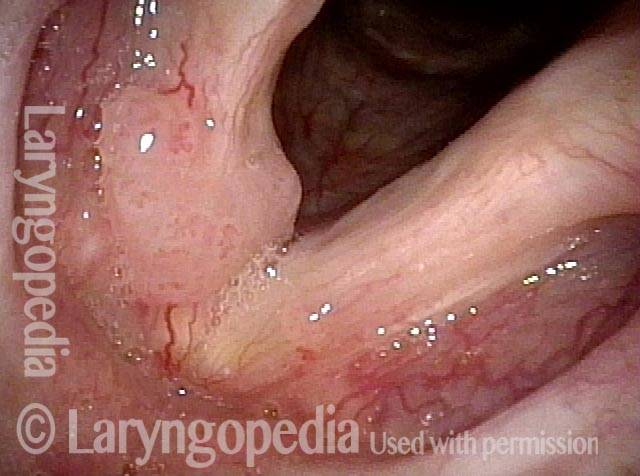
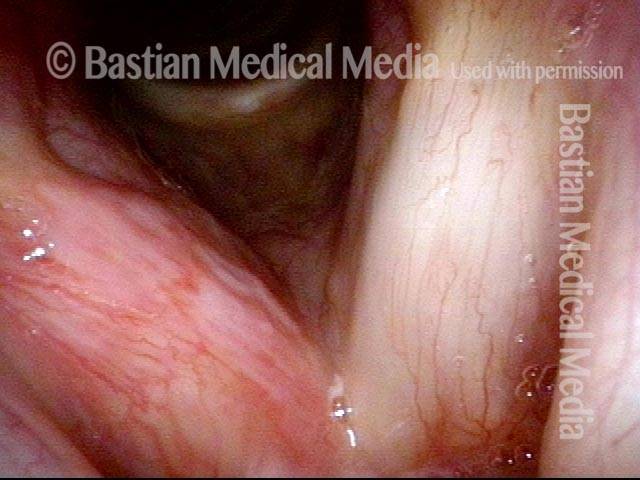
Stippled vascularity (3 of 8)
After surgery and cidofovir injection a year earlier, voice remains normal to the patient. Sharp eyes can pick up a tiny focus of stippled vascularity of the right cord (left of photo).

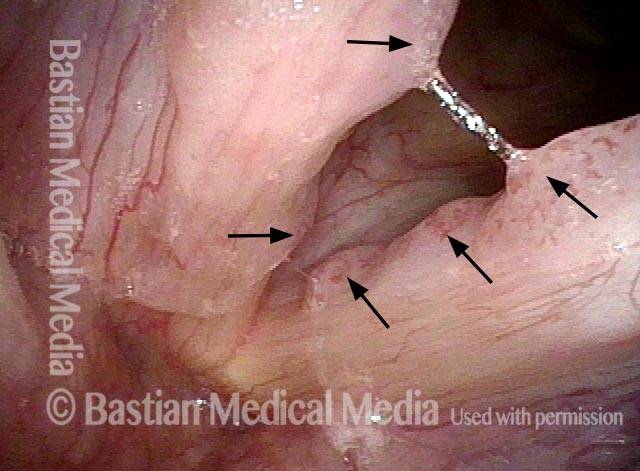
HPV vascular effect (4 of 8)
At closer range with narrow band light, the HPV vascular effect on the right cord is made more obvious (arrows). The patient requested a “curative mode” additional surgery to clear up this tiny residue and inject cidofovir.

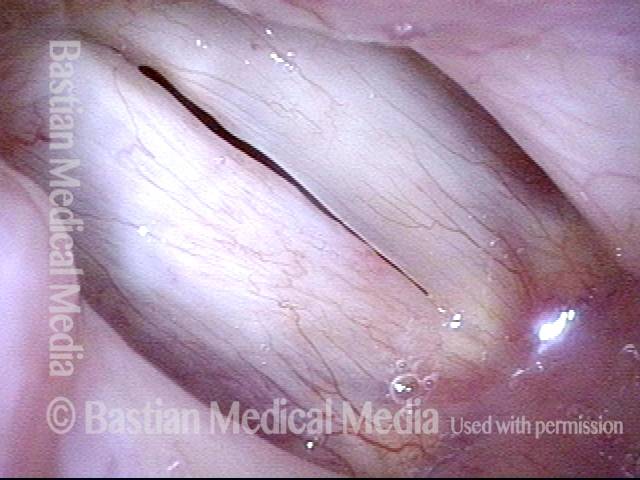
16 months later (5 of 8)
16 months later, voice remains normal to patient, and there is no sign of recurrent HPV vascularity or lesion.
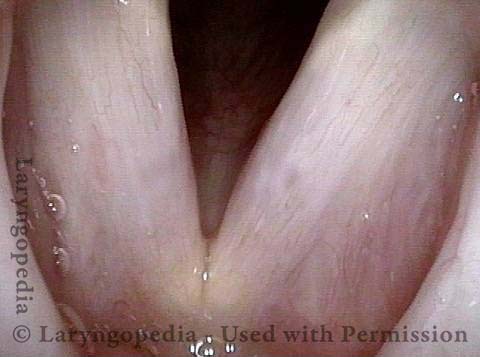
Is it long-term remission? (6 of 8)
A slightly blurry narrow band view, again showing no sign of stippling. Is she “cured?” Or in long-term remission?

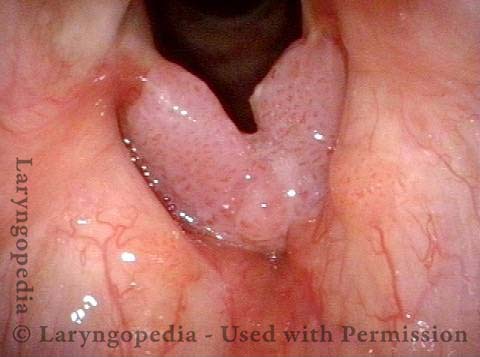
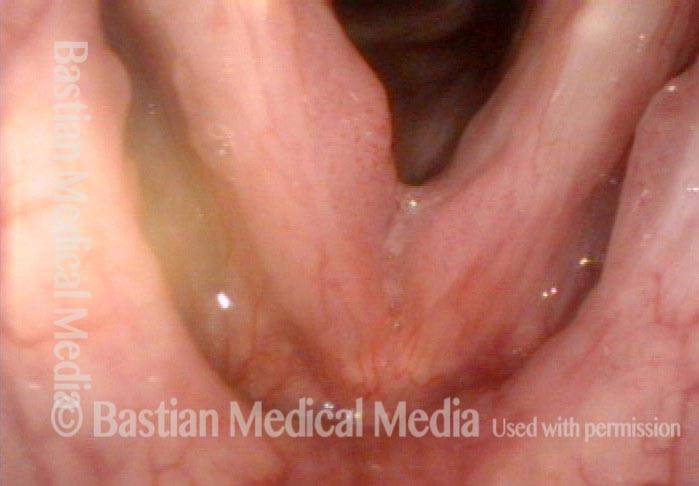
Recurrent Papilloma (7 of 8)
After 8 years of normal voice, the patient re-presented due to hoarseness, saying that her voice had been “perfect” up until a few weeks earlier. She was not sick, but noticed increased “drainage” and voice change. The explanation is a recurrent papilloma.
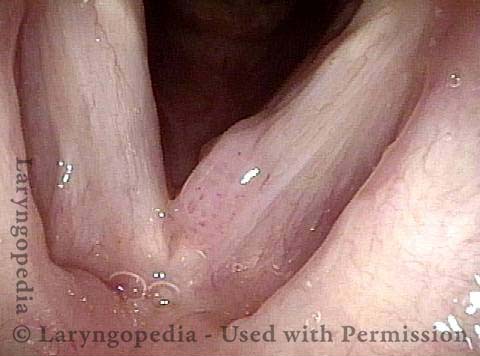
Stippled vascularity (8 of 8)
Narrow band light again accentuates the stippled vascularity. The patient is embarking on another “curative mode” series of surgical procedures, hoping to again put her into remission.

HPV 18—High Risk Subtype
Papillomas seen (1 of 4)
Middle-aged man with chronic hoarseness and the lesions seen here, diagnosed by the pathologist as papillomas.
Stippled vascularity (2 of 4)
Closer view. Stippled vascular markings consistent with HPV effect are seen more clearly here.

Surgical removal (3 of 4)
Soon after microlaryngoscopic removal, and in preparation for followup cidofovir injection.

Cidofovir injection (4 of 4)
Needle (arrow) and blanching and swelling of the left cord as cidofovir is injected. The same technique can be used for Avastin.