Tracheal Stenosis Here Is A Red Herring; the Diagnosis Is Actually CPS
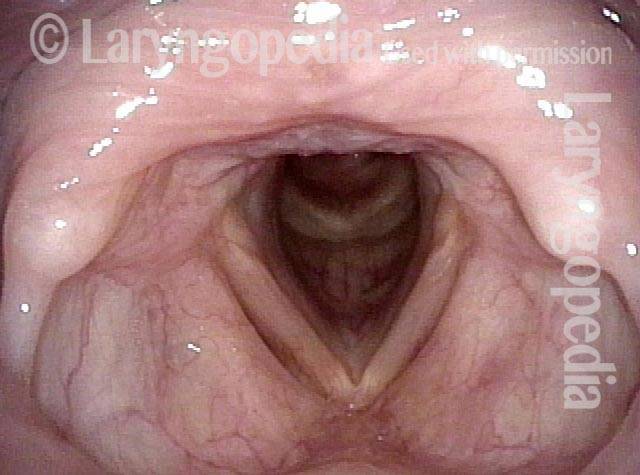
Tracheal stenosis? (1 of 4)
During a grave illness, this woman eventually underwent tracheotomy. Though she wore the tube for several months, it was removed 3 years ago. Only six months prior to this examination, due to a feeling of choking, she underwent a CT scan that revealed tracheal stenosis. The patient does have mildly noisy breathing but has no sense of exercise intolerance.
Narrowing at trachea (2 of 4)
Viewing from just below the vocal cords, there is narrowing and deformity of the trachea at the site of prior tracheotomy.

Closer view (3 of 4)
A closer view shows normal trachea beyond.

No significant change in breathing (4 of 4)
Now with the scope through the area of greatest narrowing, the patient doesn’t experience any significant change in her breathing. Her symptoms are those of cricopharyngeus spasm, not tracheal stenosis.