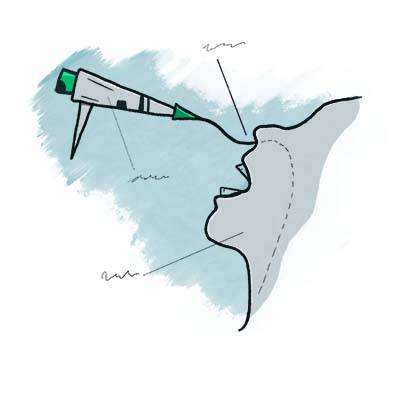



VESS bewertet Ausrüstung, Sekrete und dann die Schluckfähigkeit
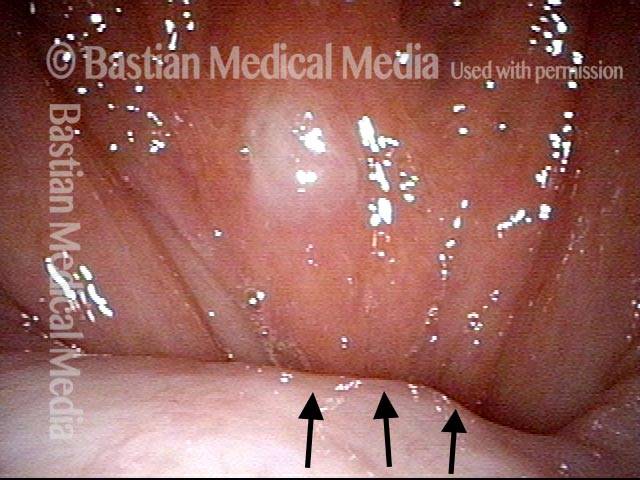
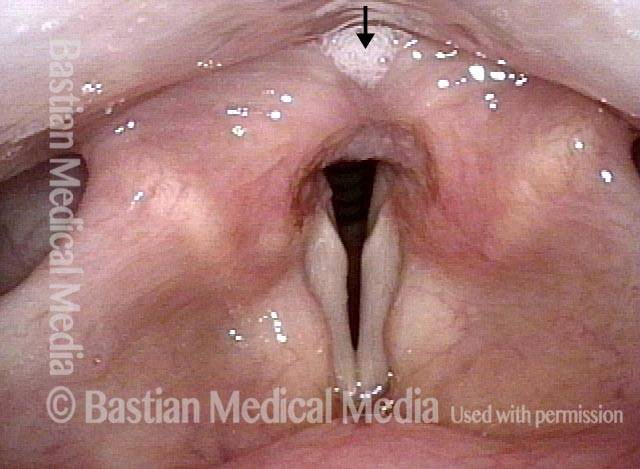
Part Ia: Palate elevates normally (1 of 7)
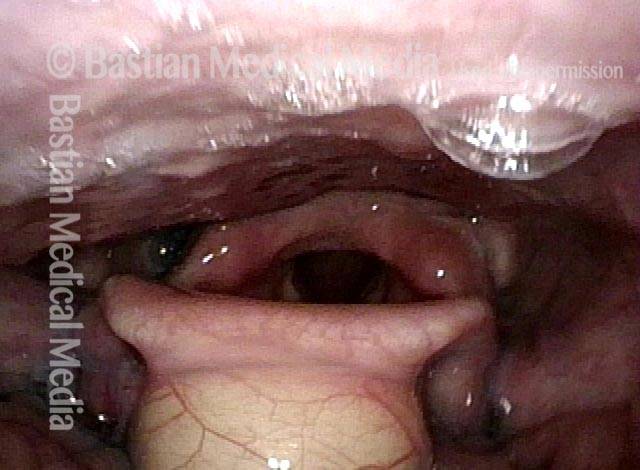
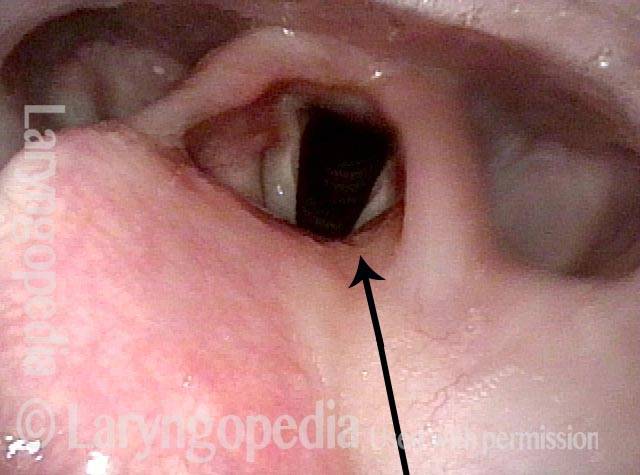
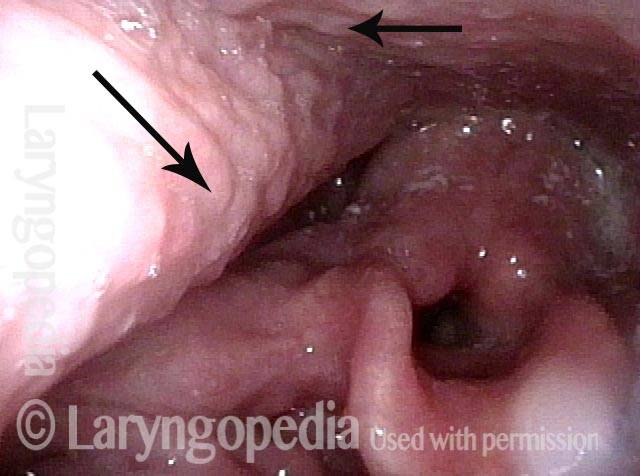
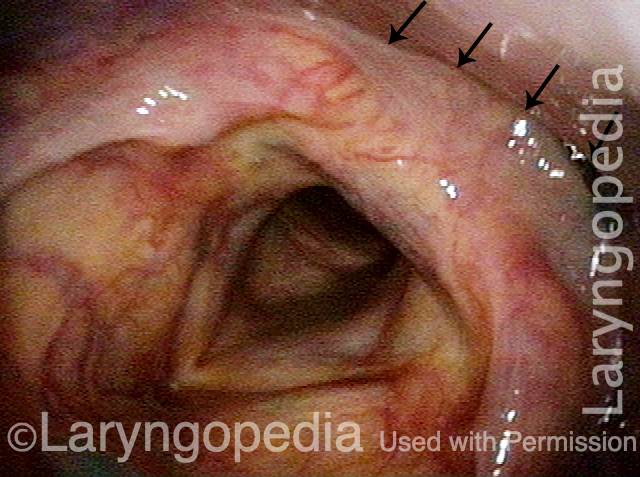
This man has symptoms of cricopharyngeus muscle dysfunction (CPD), with frequent lodgment of solid food (never soft or liquid material) at the level of mid-to-low neck. This VESS sequence demonstrates his propulsive or “pitcher” ability. Here in VESS part Ia, palate elevates normally (arrows). Left palate is not drooping and there is no deviation.
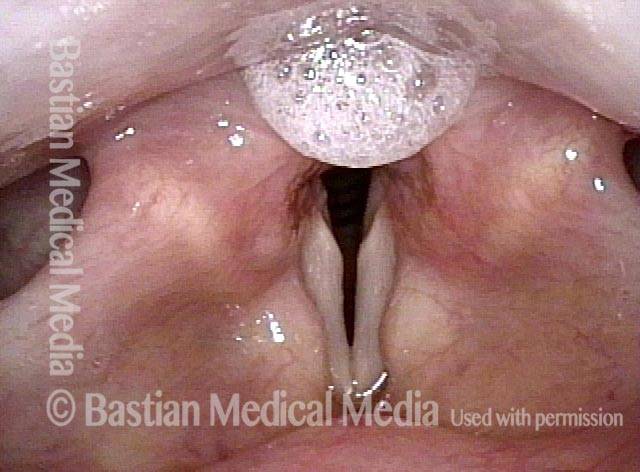
Part Ib: phonation (2 of 7)
In Part Ib of VESS, the patient makes voice, to prove normal movement and good closure of the vocal cords. In addition, no secretional pooling is seen in vallecula or pyriform sinuses.
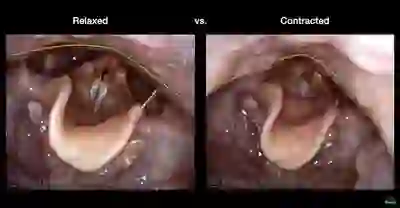
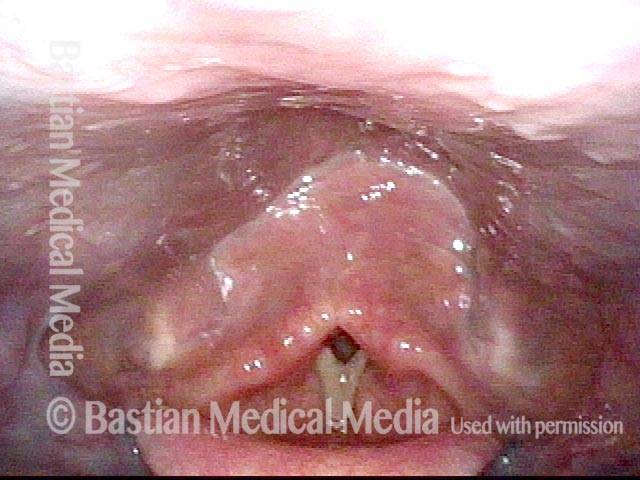
Part Ic: High pitch elicited (3 of 7)
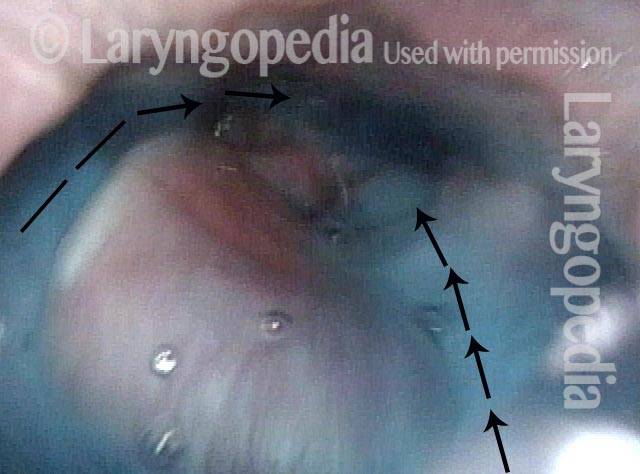
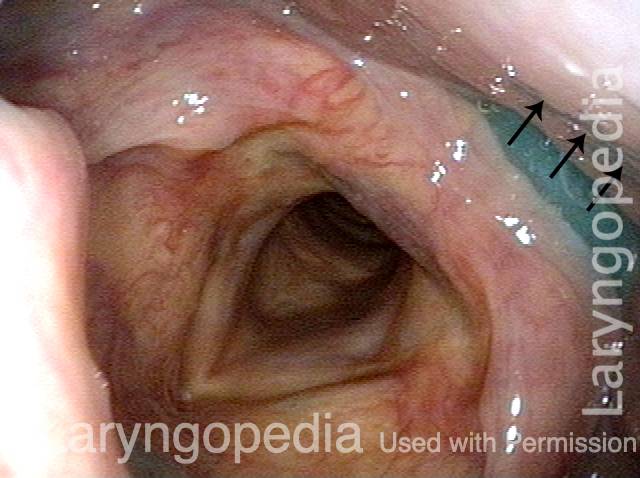
Part Ic: Very high pitch is elicited. Pharyngeal walls contract inward (arrows), closing the pyriform sinuses. Part Ia,b, and c (Photos 1, 2, and 3) verify that there is good function of swallowing equipment, i.e. palate, pharynx, and larynx (and tongue).
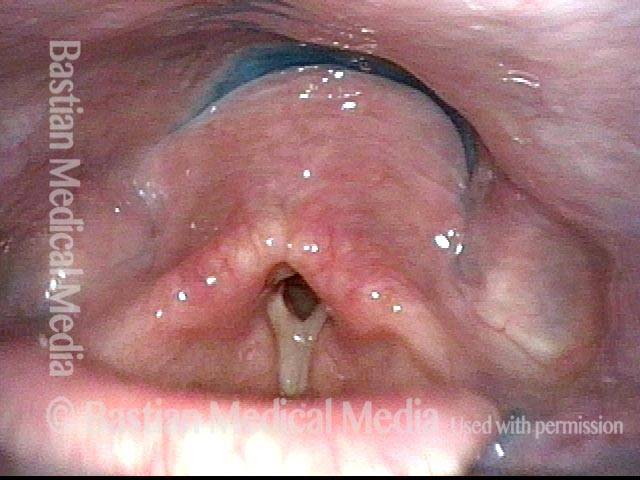
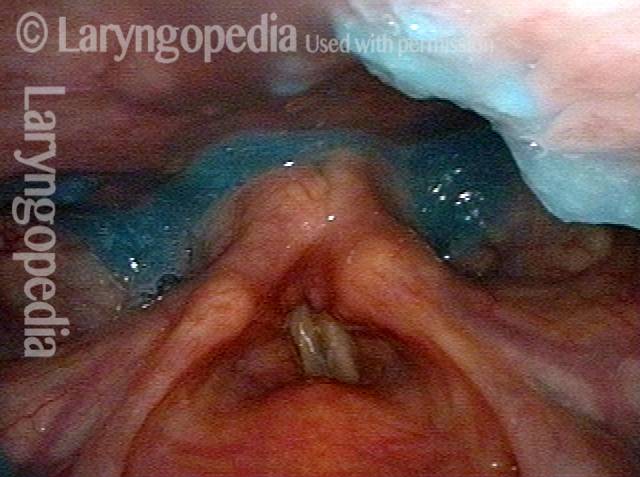
Part IIa: applesauce (4 of 7)
Part IIa: Blue-stained applesauce is first, because puree is the “easiest” material for the majority of patients, whatever their diagnosis. Here, one sees only minimal residue after several boluses are swallowed.
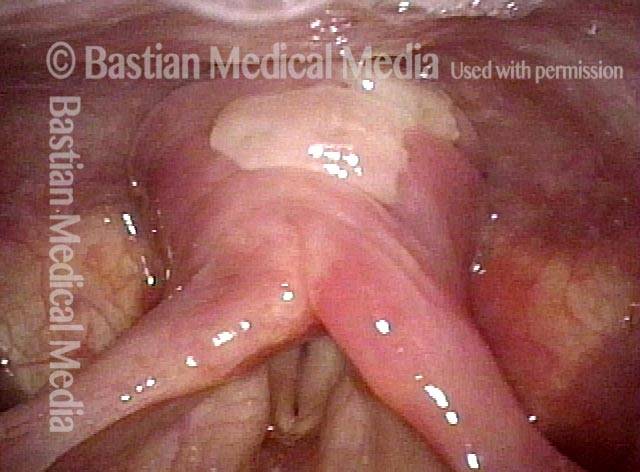
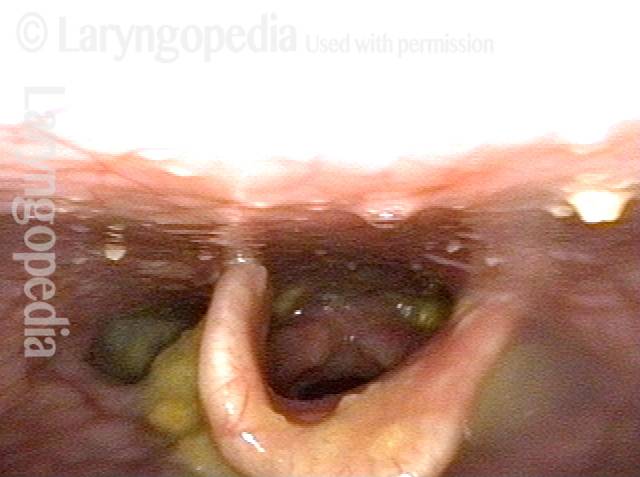
Part IIb: cracker (5 of 7)
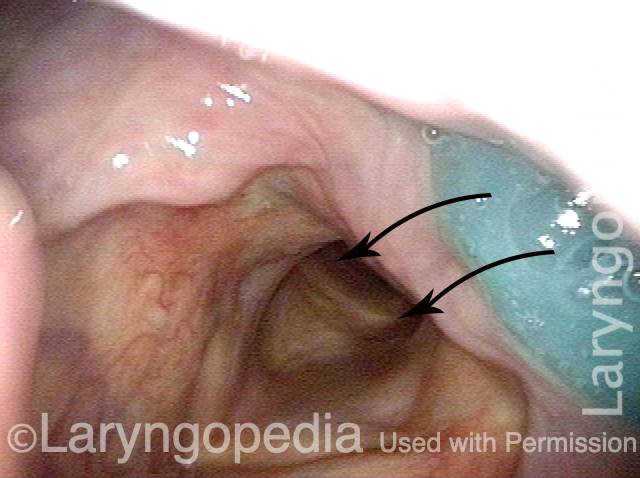
Part IIb: After an orange (cheese) cracker, lodgment in the vallecula, and…

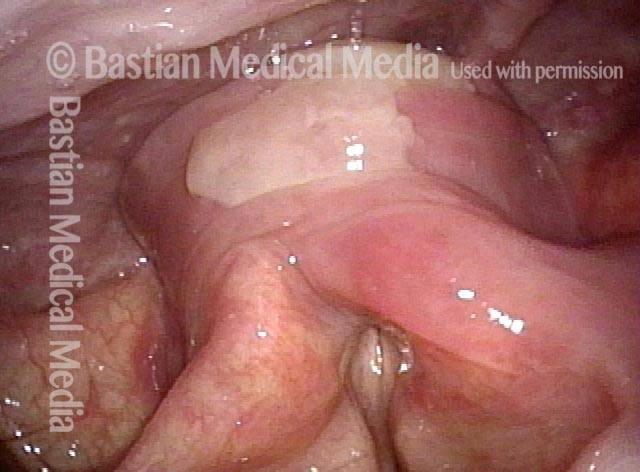
Part IIb: continued (6 of 7)
…on the pharyngeal walls (arrows).
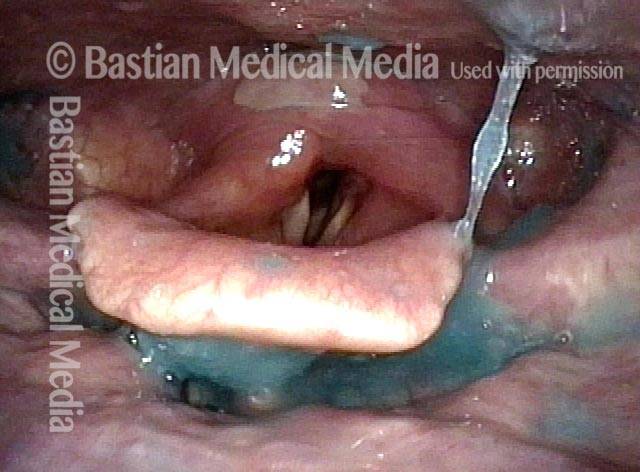
Part IIc: water (7 of 7)
Part IIc: After several boluses of blue-stained water, all cracker is washed away and there is no blue staining or residue within the laryngeal vestibule, subglottis, or high trachea. Given this man’s CPD symptoms, VFSS may show a cricopharyngeus muscle bar, indicating incomplete relaxation of the upper esophageal sphincter.
Dysphagie / verzögerter Schluckreflex
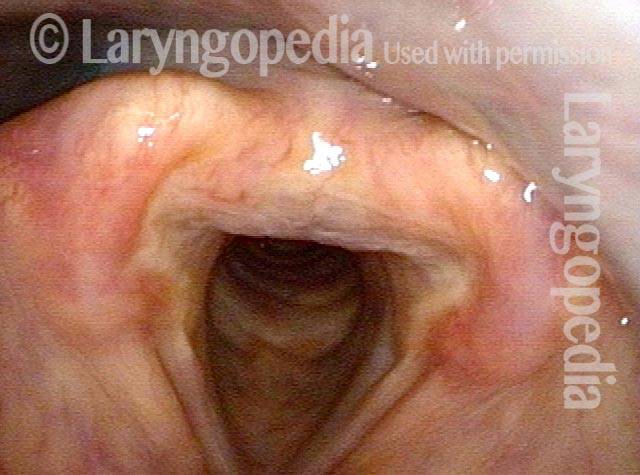
Laryngopharynx (1 of 3)
Panoramic view of laryngopharynx before administering blue-stained applesauce.
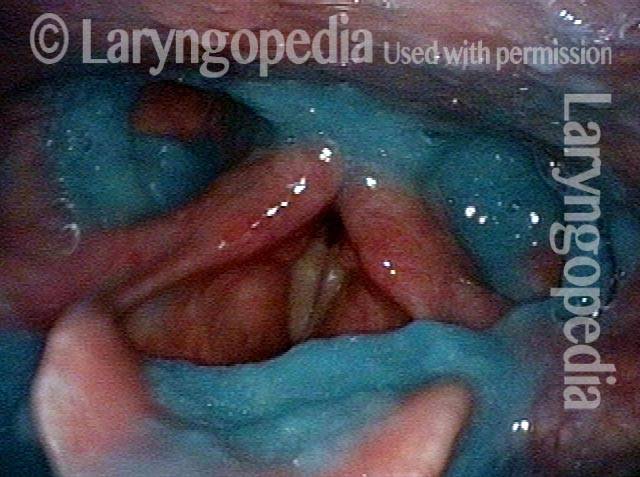
Dysphagia / Delayed swallow reflex (2 of 3)
Same view after first bolus of blue-stained applesauce. The vallecula fills with material before the swallow “happens”—signifying a delayed swallow reflex.
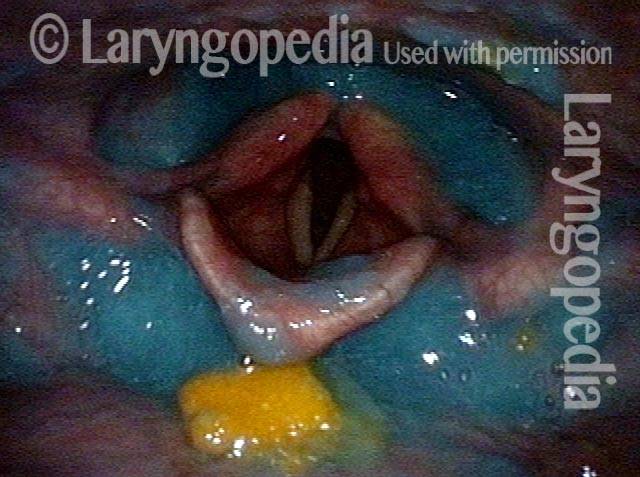
Hypopharyngeal pooling (3 of 3)
After several rapidly-administered boluses (to assess patient’s “limits”), note hypopharyngeal pooling, but none within the laryngeal vestibule.
Zenkers Divertikel
Zenker’s diverticulum (1 of 3)
This view is a moment after a completed swallow of blue-stained applesauce.

Postcricoid area (2 of 3)
Same view, a second later, as blue-stained applesauce emerges from the Zenker’s diverticulum upward (toward the camera) into the postcricoid area.

Hypopharynx (3 of 3)
Another second later, applesauce continues to re-emerge into the hypopharynx.

Beispiel 2
Zenker’s diverticulum (1 of 4)
This middle-aged woman has had a known Zenker’s diverticulum for several years. She has now reached a point of frustration that has motivated her to proceed with cricopharyngeus myotomy. The series that follows explains some of the reason for her frustration. In this view, the patient has just completed a swallow of her saliva.

Saliva from Zenker’s sac (2 of 4)
A few seconds later, saliva begins to return upwards into the post-arytenoid area (at arrow) from the Zenker’s sac.
More saliva (3 of 4)
Less than a second later, more saliva comes upward from the Zenker’s sac.
Forced to re-swallow (4 of 4)
A few seconds later, sufficient saliva has welled up from the sac that the patient is forced to re-swallow, taking her back to the appearance of the first photo in this series, only to begin the same cycle depicted in these four photos again and again.

Reflux in den Hypopharynx, charakteristisch für krikopharyngeale Dysfunktion
Reflux into hypopharynx (1 of 3)
The patient has swallowing problems typical of cricopharyngeal dysfunction. This swallow study reinforces that impression as well as the likely presence of a Zenker’s diverticulum. In this photo, blue-stained water has just been swallowed, and the vocal cords are beginning to open. At this point, the hypopharynx contains no residue.
Water flows into the swallowing crescent (2 of 3)
One second later, the blue-stained water begins to emerge from just above the cricopharyngeus muscle into the „swallowing crescent“.
Larynx opens up (3 of 3)
Another two seconds later, the larynx has fully opened post-swallow. The post-swallow hypopharyngeal re-emergence of the blue-stained water is apparent.

Hypopharynx-Pooling nach dem Schlucken
Hypopharynx pooling after swallow (1 of 1)
Shows trace of blue-stained applesauce remaining behind after the patient has swallowed.

Kehlkopfpenetration
Laryngeal penetration (1 of 1)
After the patient swallowed several boluses of blue-stained applesauce, there were traces visible on the laryngeal surface of the epiglottis, indicative of penetration into the earliest part of the airway. By itself, soiling of the laryngeal vestibule to this minor degree does not threaten the person’s ability to eat by mouth.
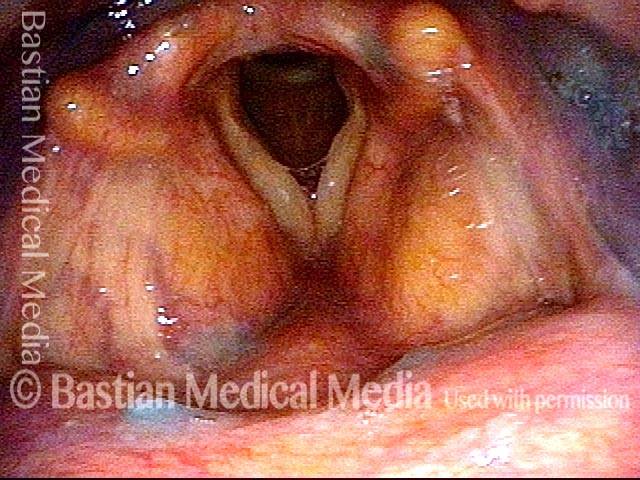
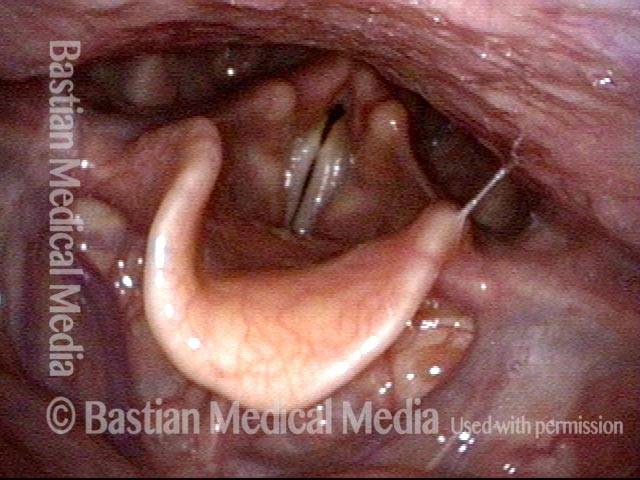
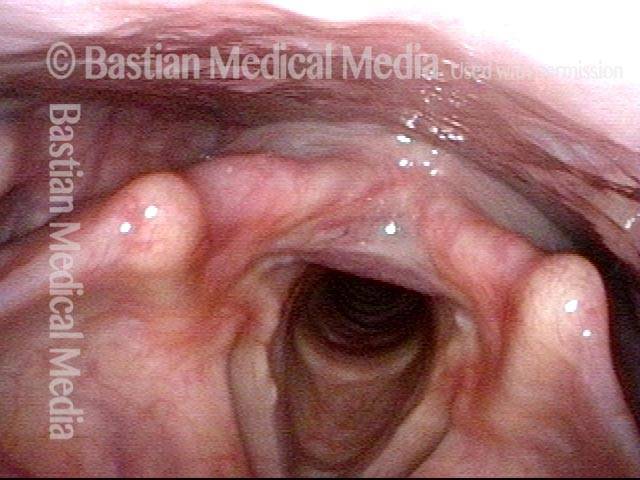
Vallekulare Zysten stören das Schlucken nicht – außer wenn sie es tun
Vallecular cyst (1 of 4)
Enormous vallecular cyst in this young woman. Swallowing of solids is affected. Food seems to catch and then expectorate back up to the mouth. No problem with liquids.
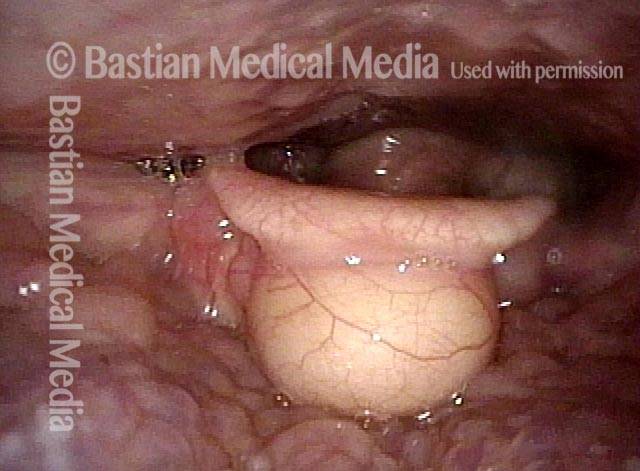
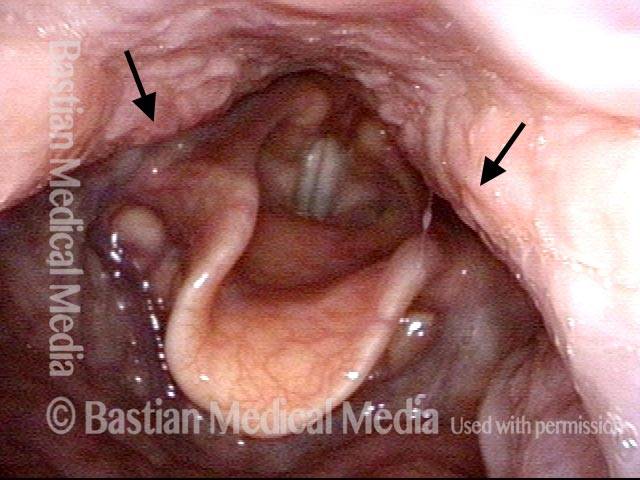
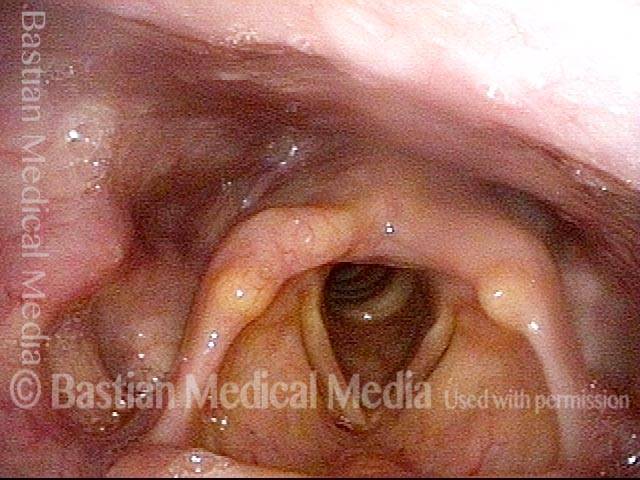
Evaluation of function (2 of 4)
Palate, pharynx, and larynx function are all normal. There is no pooling of saliva in the hypopharynx.
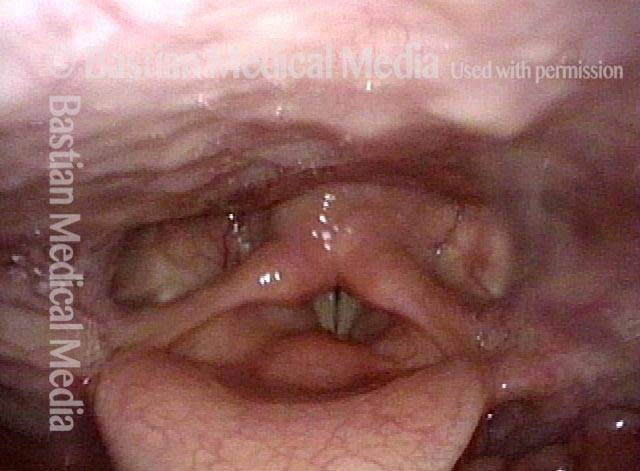
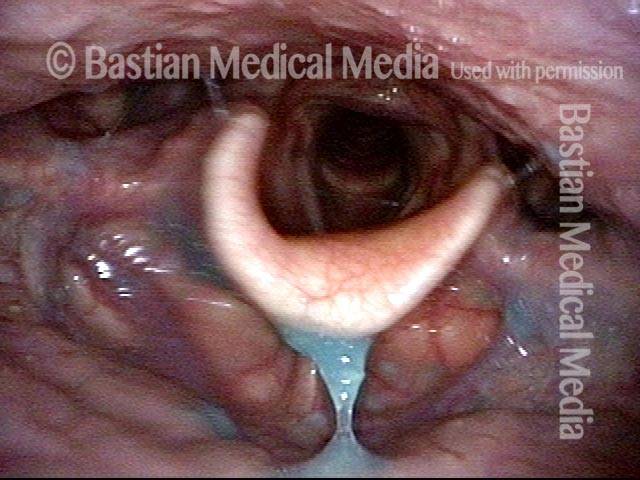
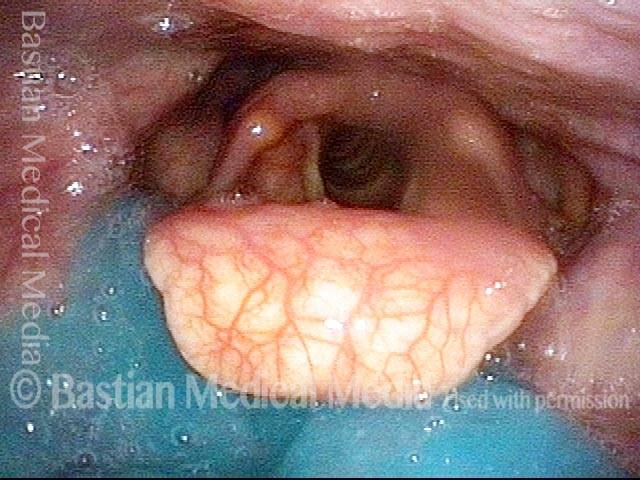
Applesauce residue (3 of 4)
An organized ring of applesauce remains after trying to swallow blue-stained applesauce.
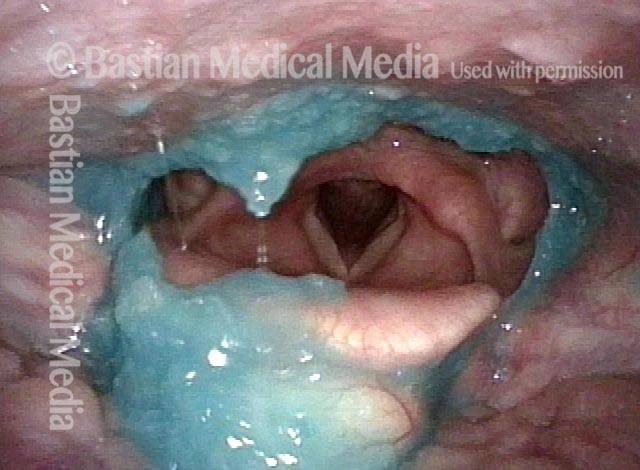
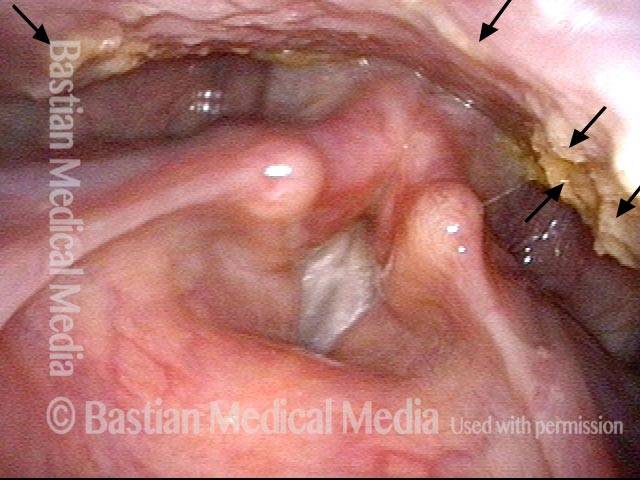
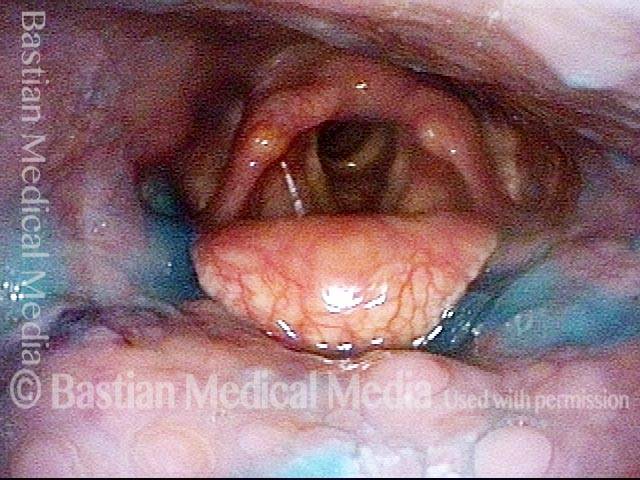
Water wash (4 of 4)
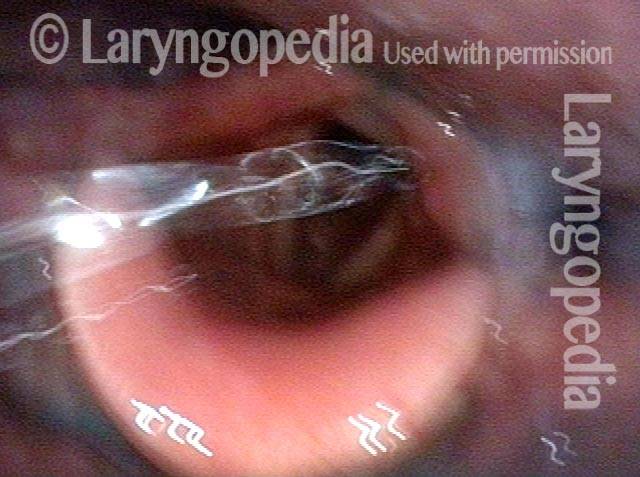
Water wash is very effective in clearing the applesauce away. Vallecular cysts are usually left alone; here, the plan is to remove it with the thulium laser and see if swallowing is restored.
Pillenunterbringung aufgrund von Schluckbehinderung
Lodged pill (1 of 4)
This older woman swallowed a pill that lodged low in her throat. In spite of repeated swallows and attempts at expectoration, she couldn’t move it for many hours. On examination a few days later, this superficial ulceration is seen due to mild chemical burn. Note as well the redness of the left arytenoid and pyriform sinus (right of photo).
Trumpet maneuver (2 of 4)
At closer range, while having the patient perform a trumpet maneuver, a well-demarcated superficial ulcer is seen again.
VESS (3 of 4)
Administration of blue-stained applesauce during VESS shows that a partial reason for lodgment may be reduced propulsive strength, indicated by pooling of material in the vallecula.
Incomplete relaxation of CPD (4 of 4)
After sips of blue-stained water, note the fairly organized crescent of pooled water in the pyriform sinuses and post-arytenoid area. This can suggest a functional outlet obstruction caused by incomplete relaxation of the cricopharyngeus muscle (CPD).

Verzögerter Schluckreflex: Vergleichen Sie blaues Apfelmus und blaues Wasser
VESS (1 of 4)
During VESS, blue-stained applesauce falls down to the posterior base of tongue. If the swallowing reflex were normal, the patient would have swallowed before the applesauce arrived here.

Delayed swallow reflex (2 of 4)
Because of the viscosity of the material it „hangs“ for a moment and does not fall down into the entrance of the larynx. Even with a delayed swallow reflex, there is still a second or two to swallow before that happens. The patient will tend to cough less with this consistency than with water.

Blue-stained water (3 of 4)
Here, blue-stained water is flowing into the right pyriform sinus (left of photo at arrow). Movement is rapid (note the blur) due to the low viscosity of water; there is less time to react and swallow than with applesauce, explaining why coughing on water is more common than purée or solid.
No residue (4 of 4)
Still, at the end of several boluses of applesauce and water, stained with blue food coloring, there is no stain or residue inside the entrance of the airway. The delayed swallowing reflex is a liability but without a risk of pneumonia.
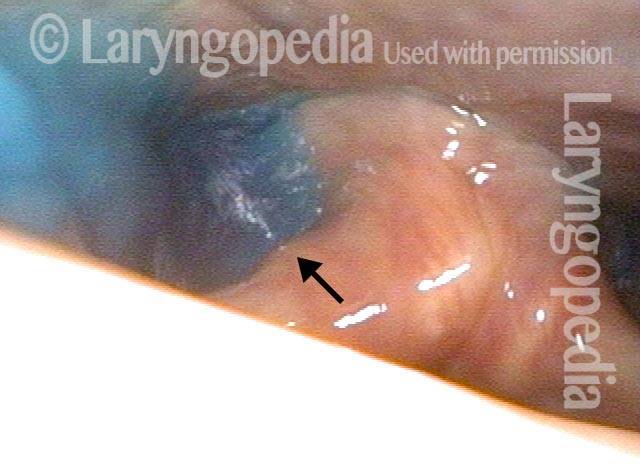
Narbenbildung leitet geschluckte Materialien direkt in den Kehlkopf
Post tonsillectomy (1 of 4)
A young woman struggles to swallow after extensive cauterization of severe bleeding after tonsillectomy elsewhere. The arrows here show the path food and liquid should follow to get into the esophagus (opening indicated by flat oval).
Closer view (2 of 4)
Closer view shows that the epiglottis is tethered to base of tongue at the dotted line. Furthermore, the „ski jump“ scar appears to be ready to divert swallowed material directly into the larynx ( arrow) rather than into the pyriform sinus at *.
The „chute“ (3 of 4)
A closer view shows even better the „chute“ into the larynx.
Abnormal diversion (4 of 4)
While swallowing blue-colored water, arrows indicate the normal path on the left (right of photo) and the abnormal diversion into the larynx on the right (left of photo). The patient manages, but must swallow carefully, especially since the epiglottis cannot invert since it is scarred to the base of tongue as shown in photo 2.
Schädelbasisfraktur und Verletzung des Vagusnervs – Beachten Sie die Pharynxkontraktion und die Auswirkungen auf das Schlucken
Palate branch of the vagus nerve (1 of 4)
This young woman sustained facial bone and skull base fracture during an auto accident. In this nasopharynx view, note that her right palate (left of photo) elevates fully (long arrow), while the left side only partially (short arrow). The palate branch of the vagus nerve is injured on the left (right of photo).
Pharynx branch of the vagus nerve (2 of 4)
At rest, the pharynx appears flat and symmetrical, but there is a question whether the midline may have migrated to the patient’s right (left of photo). The vagal branch to the pharynx is also injured on the left (right of photo)
Damage to left vagal nerve function (3 of 4)
By eliciting a very high-pitched voice, a pharynx contraction is recruited and now we can see that the pharyngeal wall pulls to the right (horizontal arrow) and the constrictor muscle squeezes inward only on the right (long arrow at left of photo). This confirms good right vagal function (left of photo) and damage on the left (not pictured).
Residue during swallowing test (4 of 4)
After eating a cracker and attempting to wash it away with water, the residue is primarily in the vallecula and left pyriform sinus. Arrows show how the pharynx can squeeze during swallowing in order to clear out the right pyriform sinus (left of photo). With no active muscle on the left (right of photo) to clear out the pyriform sinus, it pools food.
VESS in 6 Standbildern
Assessing the patient’s swallowing (1 of 6)
Step 1 is assessment of the patient’s swallowing „equipment.“ Here we see that the palate elevates symmetrically against the posterior pharyngeal wall.

Observing the pharynx (2 of 6)
The next step is to observe the pharynx squeeze with inferior constrictors bulging to surround the larynx. The vocal cords close fully.

Patient secretions (3 of 6)
Next is the assessment of patient secretions. This hypopharyngeal pooling of saliva (foamy bubbles) predicts that there will be similar pooling of swallowed food materials during the next step of VESS.

Pooling of swallowed pureed food (4 of 6)
As predicted, blue-stained applesauce (purée consistency) pools in the pyriform sinuses. There is no laryngeal soiling (penetration, aspiration).
Swallowing solids (5 of 6)
The next test is the cheese cracker (solid consistency). After swallowing, the residue is seen especially in the vallecula.
Residue after foods (6 of 6)
After several boluses of blue-stained water, a small amount remains in the pyriform sinuses and post-arytenoid area.
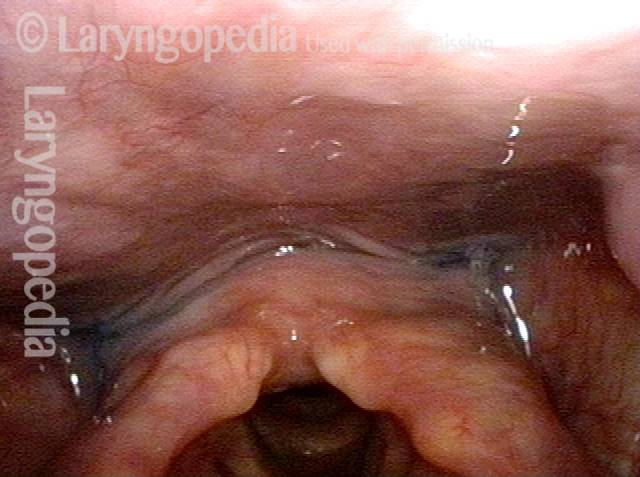
VESS (Videoendoskopische Schwalbenstudie) Befunde nach Strahlentherapie
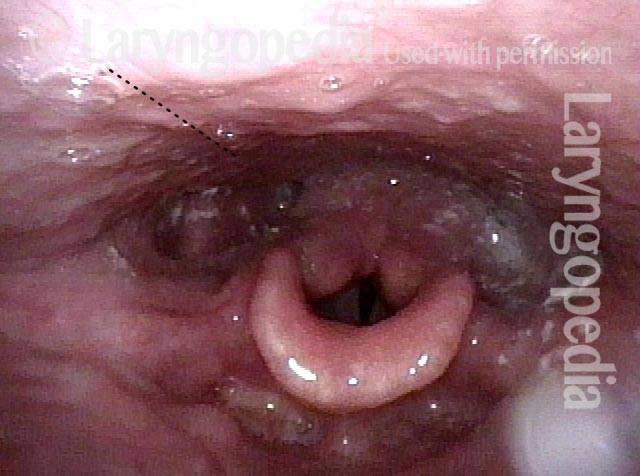
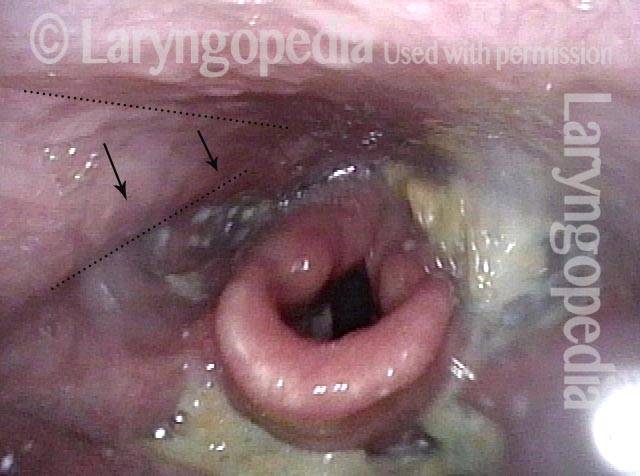
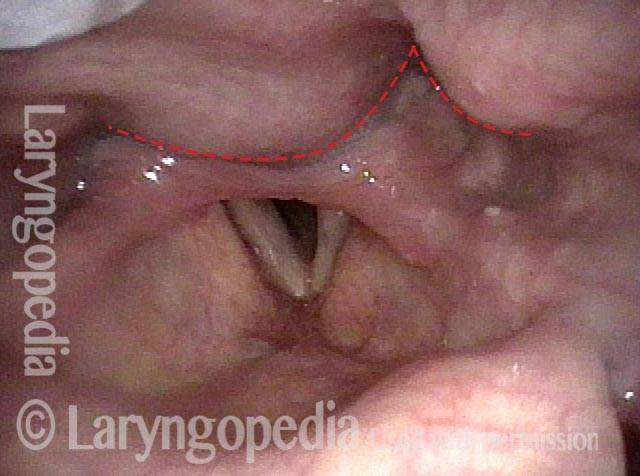
Narrowed pharyngeal wall (1 of 7)
After radiation and chemotherapy for larynx cancer several years earlier. Note the dry secretions. There is narrowing of the pharyngeal wall (dotted line) due to radiation scarring.

Swallowing applesauce (2 of 7)
After the second bolus of blue-stained applesauce. The propulsive ability („pitcher of swallowing“) is inadequate, leaving a lot of post-swallow residue.
After sipping water (3 of 7)
After three sips of blue-stained water, much of the applesauce has been washed away.

Gravity aiding in swallowing (4 of 7)
Additional water washes nearly all of the residue in the „swallowing crescent“ away–mostly by gravity as seen in the next photo.

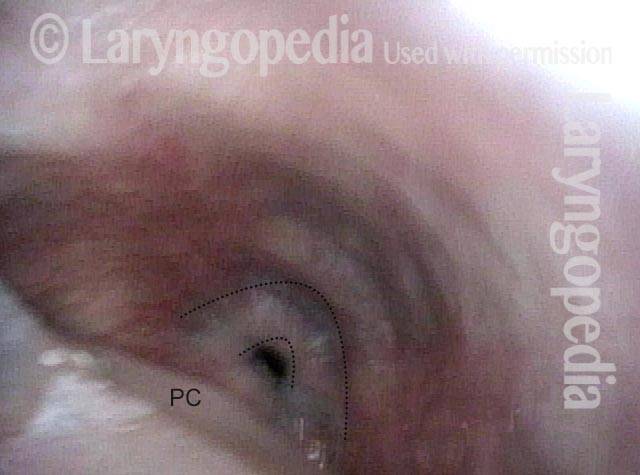
Lifting larynx (5 of 7)
Each swallow looks like this. The pharynx „bird swallow“ mechanism lifts larynx forward so that the swallowing crescent opens down to the cricopharyngeus muscle, indicated by double dotted lines. (PC = post-cricoid.)
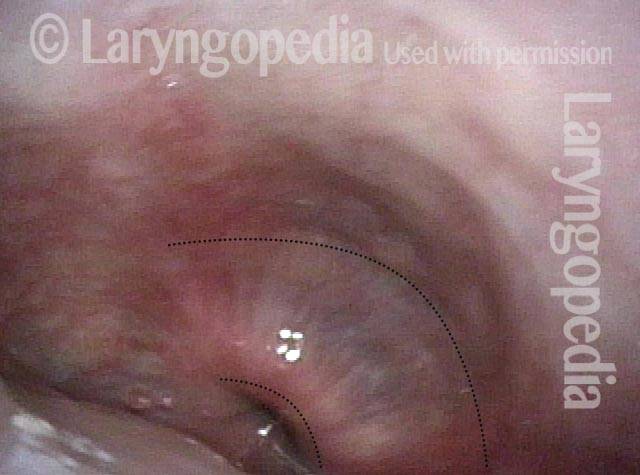
A closer look (6 of 7)
At closer range, the cricopharyngeus muscle bulge is seen more clearly, along with the small opening into the esophagus.
Gravity aiding again in swallowing (7 of 7)
Blue-stained water flowing into the esophagus mostly by gravity.
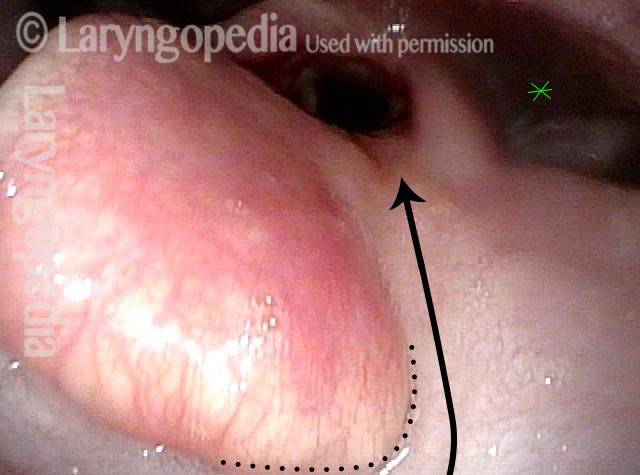
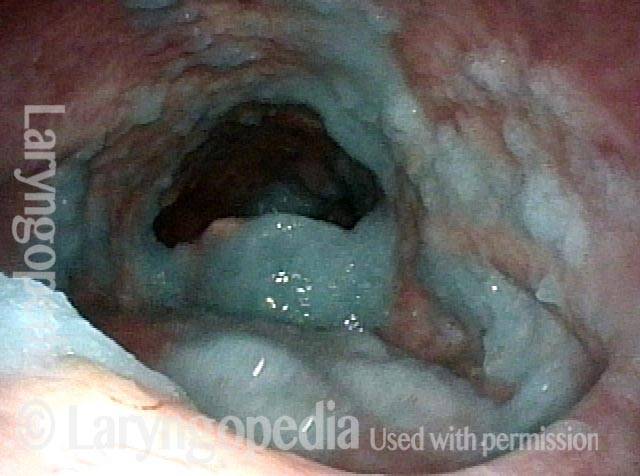
Zervikale Osteophyten selbst scheinen kein großes Hindernis beim Schlucken zu sein
Protruding osteophytes (1 of 2)
This 95 year-old man has large cervical osteophytes (bony proliferation due to arthritis). These osteophytes protrude into the pharynx (dotted lines). It would seem they would be a major impediment to swallowing.
Rapid swallowing (2 of 2)
After an initial test swallow, eight boluses of blue applesauce are administered rapidly. The purpose of this is to serve as a “stress test” so that we see his swallowing at its worst…But he has only a small amount of residue, and passes the test. Most individuals with cervical osteophytes are of advanced age. When swallowing is impaired, the explanation is usually more than just the osteophyte.

Aspiration und Quelle des zurückgekehrten Aspirats nach Husten
Salivary pooling (1 of 5)
This young man has a chromosome disorder. He has trouble swallowing but no history of pneumonia. The palate, pharynx, and larynx motor function is normal, but the salivary pooling seen here predicts what follows…

After applesauce (2 of 5)
After several boluses of blue-stained applesauce, there is significant pooling (residue), but nothing down at the level of the vocal cords.
After cheese cracker (3 of 5)
After chewing and swallowing a cheese cracker, a part is lodged in the vallecular.
After water (4 of 5)
During administration of blue-stained water, a large drip is seen falling downwards, directly into the laryngeal vestibule.
Cough expels the water from airway (5 of 5)
A moment later, a cough sprays the aspirated blue-stained water upwards and out of the airway.

Das Zenker-Divertikel gibt seinen Inhalt nach jedem Schlucken nach oben in die Kehle zurück
VESS (1 of 3)
During Videoendoscopic swallow study (VESS), this patient has just swallowed blue applesauce. It has disappeared downwards (arrows) into the upper esophagus but part of it is retained in a Zenker’s diverticulum (out of view).
Swallowing Crescent (2 of 3)
Exactly one second later blue applesauce appears in the swallowing crescent as the sac empties a part of its contents upwards.
Applesauce spills into airway (3 of 3)
One second later, even more blue applesauce has emerged. If it were more liquid, it would spill forward to enter the airway. This explains the constant throat clearing and re-swallowing of persons with Zenker’s diverticula (caused by antegrade cricopharyngeus dysfunction).
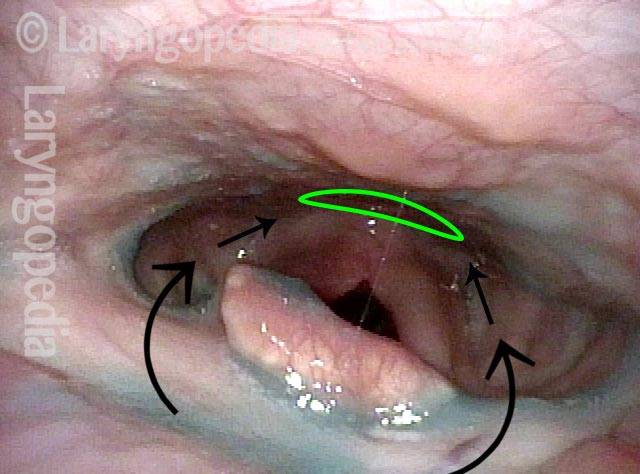
Drei Ansichten des Ösophaguseingangs von weit weg bis nah
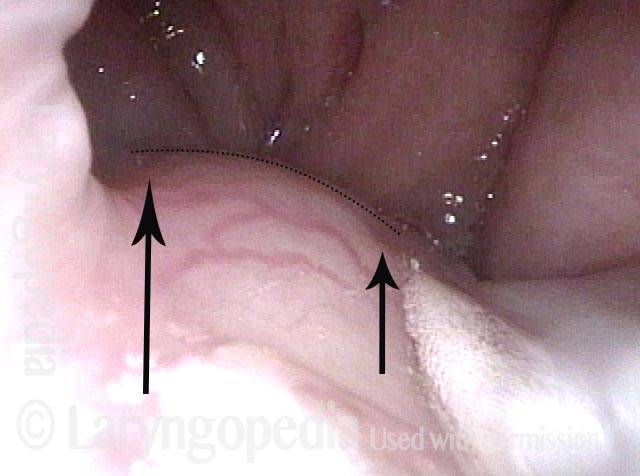
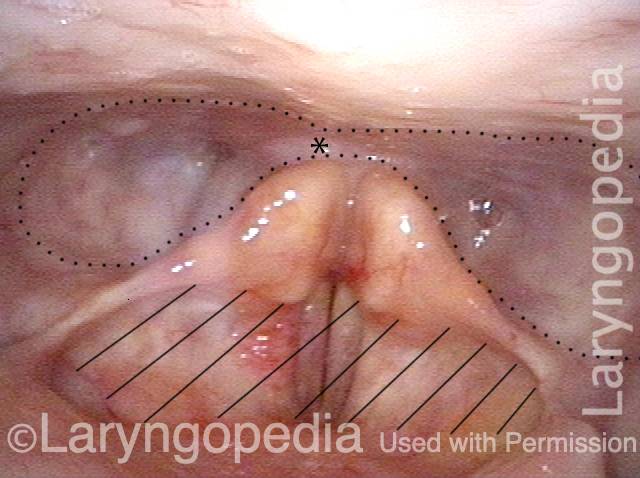
Swallowing Crescent (1 of 3)
During swallowing, the “the swallowing crescent”—outlined by the dotted line—receives swallowed food or liquid in order to funnel it into the esophagus (not open in this view). The asterisks are reference points to compare all three photos. One does not want any material to enter the laryngeal vestibule (hashed lines).
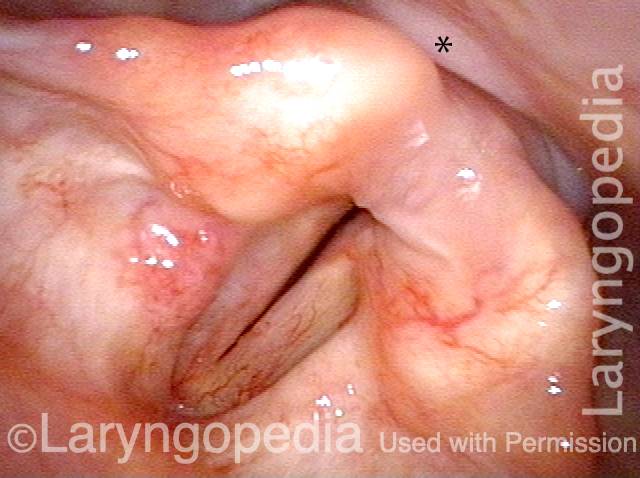
Closed esophagus (2 of 3)
A closer view. The esophagus is still not open in this view. Compare asterisk with prior and following photo.
Open Esophagus (3 of 3)
At the moment of a dry swallow, the esophagus opens as shown here. Again, the asterisks allow comparison with photos 1 and 2.
