Esophagoscopy is a procedure by which the examiner looks inside the full length of the esophagus, as well as the stomach if desired, in order to diagnose an abnormality or to take a biopsy of an abnormal lesion.
Esophagoscopy (1 of 4)
View into left pyriform sinus and post-arytenoid area.
Esophagoscopy (2 of 4)
Similar view at initiation of swallow, with opening of the upper esophageal sphincter (cricopharyngeus muscle) to allow admission of the tip of the scope.

Esophagoscopy (3 of 4)
View within esophagus, using mild air insufflation.

Esophagoscopy (4 of 4)
Within hiatal hernia.

More Interesting Esophageal Findings of R-CPD (Inability to Burp)
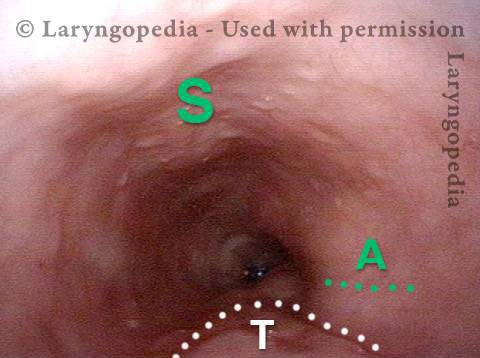
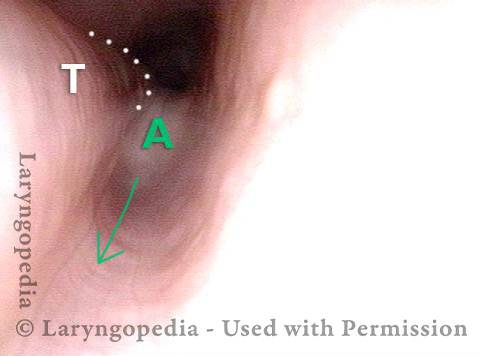
Stretched Esophagus (1 of 4)
Using a 3.7mm ENT scope with no insufflated air, note the marked dilation of the esophagus by swallowed air the patient is unable to belch. T = trachea; A = aortic shelf; S = spine
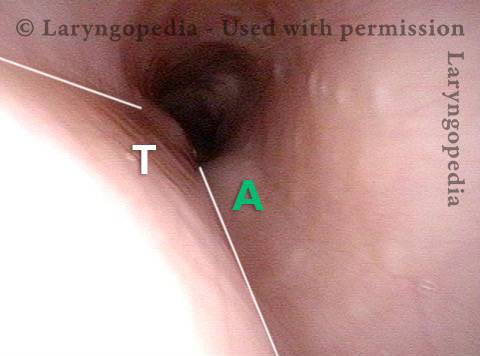
Tracheal Wall (2 of 4)
The posterior wall of the trachea (T) is better seen here from a little higher in the esophagus. A = aorta
Over-dilation (3 of 4)
The photo is rotated clockwise at a moment when air from below is pushed upward so as to transiently over-dilate the esophagus. Note that the esophagus is almost stretching around the left side of the trachea in the direction of the arrow.
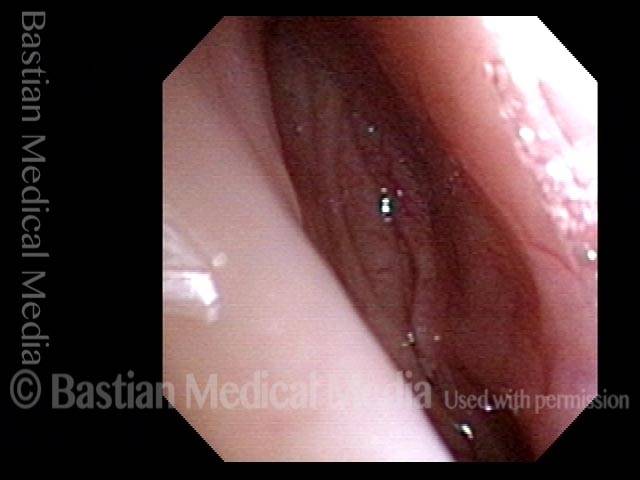
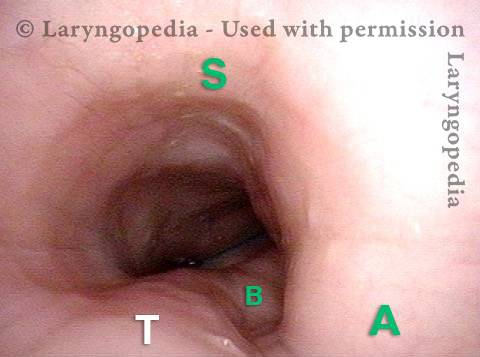
Bronchus is visible (4 of 4)
Now deeper in the esophagus (with it inflated throughout the entire examination by the patient’s own air), it even appears that the left mainstem bronchus (B) is made visible by esophageal dilation stretching around it.
Dramatic dilation of the esophagus in a person with R-CPD due to buildup of swallowed air that he cannot belch to get rid of. : Series of 2 photos
View of the mid-esophagus (1 of 2)
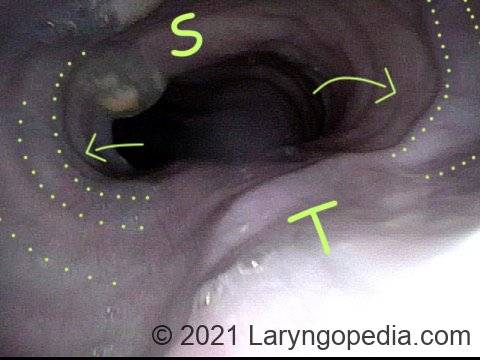
This view in the mid-esophagus was obtained with a 3.6mm scope without an air channel. The dilation is from the patient’s own unbelchable air. Note quite major lateral dilation of the esophagus, indicated by concentric dotted lines and arrows. Dilation is not possible in the direction of unyielding spine (S) and trachea (T).
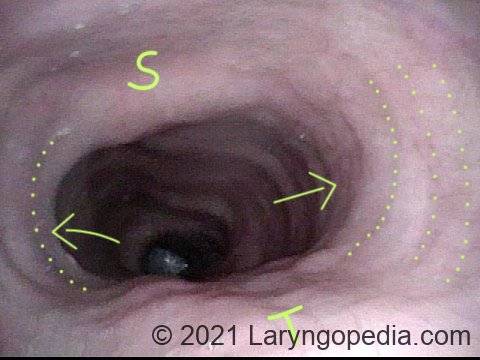
View of the mid-esophagus (2 of 2)
A view that shows more clearly the indentation of trachea (T). Persons with this much dilation of esophagus often complain as much of chest pressure as they do abdominal bloating. This man has experienced “large” reduction of R-CPD symptoms after botulinum toxin injection into his upper esophageal sphincter (cricopharyngeus muscle).