Three Views of the Entrance to the Esophagus From Far Away to Close-up
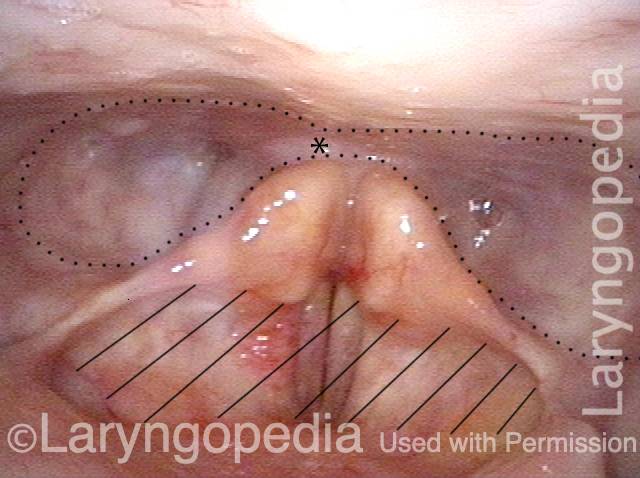
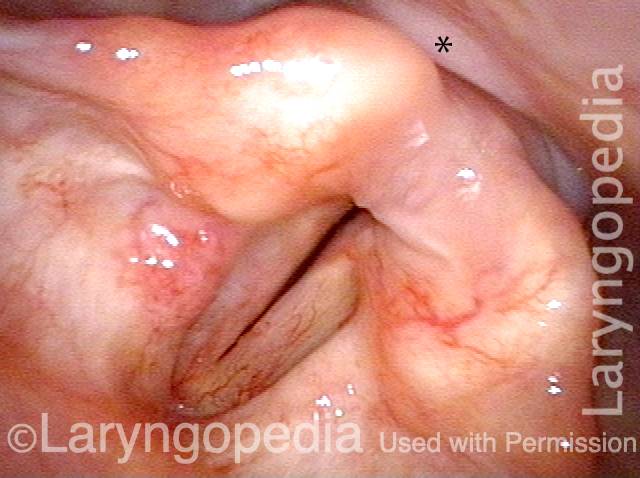
Swallowing Crescent (1 of 3)
During swallowing, the “the swallowing crescent”—outlined by the dotted line—receives swallowed food or liquid in order to funnel it into the esophagus (not open in this view). The asterisks are reference points to compare all three photos. One does not want any material to enter the laryngeal vestibule (hashed lines).
Closed esophagus (2 of 3)
A closer view. The esophagus is still not open in this view. Compare asterisk with prior and following photo.
Open Esophagus (3 of 3)
At the moment of a dry swallow, the esophagus opens as shown here. Again, the asterisks allow comparison with photos 1 and 2.

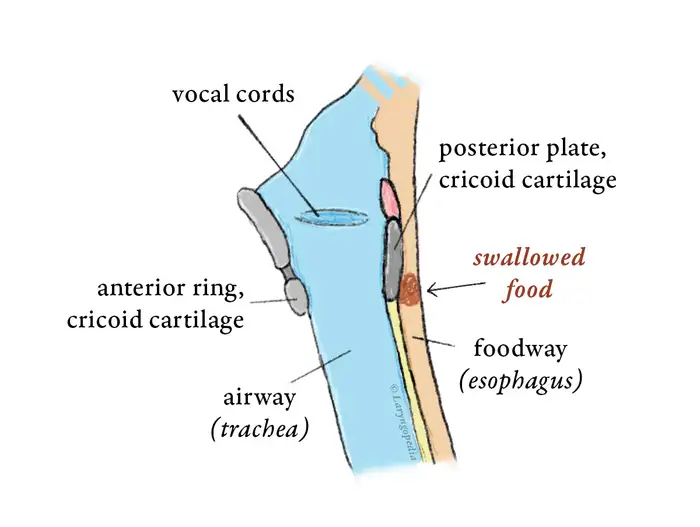
Dramatic Lateral Stretch of the Esophagus
Swallowed air (a fraction of every human swallow) must either be burped, absorbed, or (after some time) passed as flatulence. In a person with retrograde cricopharyngeus dysfunction (R-CPD: defined syndromically as inability to belch, gurgling, bloating, flatulence, etc.) the esophagus will eventually dilate.
This esophageal stretching can hurt, especially during hiccups. And the esophageal wall muscle thins out and its ability to contract weakens. The LES can also fail, leading to reflux of stomach acid from stomach up into the esophagus. Standard manometry typically describes low esophageal and LES pressures and slow transit. These findings are not the diagnosis, but instead are findings that result from the fundamental diagnosis: R-CPD.
Normal Esophageal View (1 of 3)
Expected view inside the a “general population” esophagus, when using an ENT scope. Such as scope is normally ineffective for esophagoscopy. That is because the diameter of the scope is tiny (3.7mm) and it does not have a channel to insufflate air (blow it out the tip of the scope from a compressor, to expand the esophagus). Consequently, the walls of the esophagus are collapsed and can’t be seen clearly. The arrow points to the collapsed lumen.
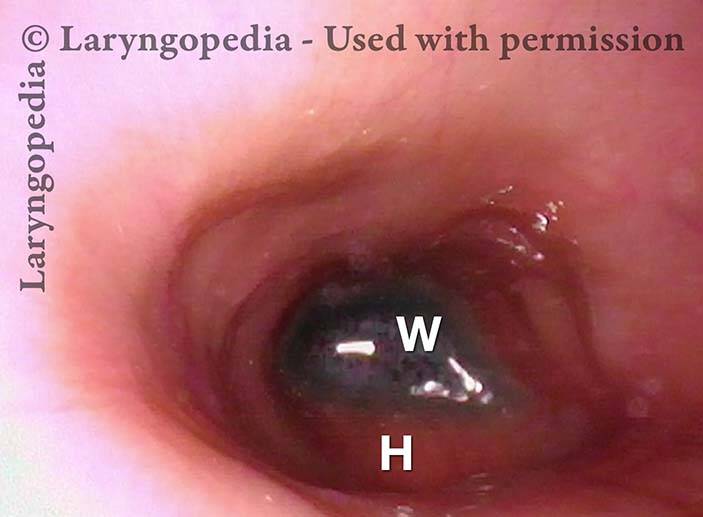
Reflux in stretched esophagus (2 of 3)
In this R-CPD patient, an ENT scope works extremely well to visualize the esophagus, because of the retained air the individual cannot burp out. That un-burped air keeps the esophagus in an “always open” state, and so the ENT scope can see the walls well. They are smooth/unwrinkled, denoting full expansion and even “stretch.” In this view of the lower esophagus, H = the posterior surface of the beating heart. W= blue water the patient has swallowed, pooled in the lower esophagus and occasionally refluxing upward.
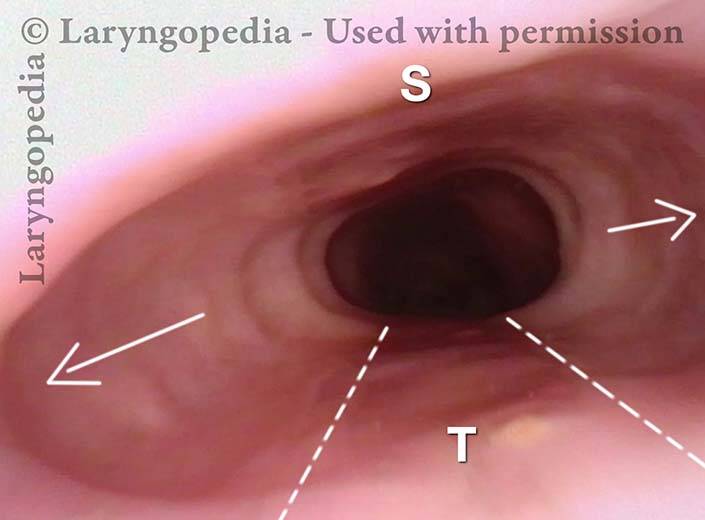
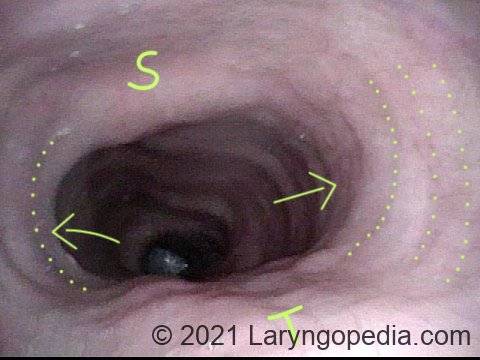
Stretched Esophagus (3 of 3)
This view is in the mid-esophagus. The tracheal “mound” is indicated by the dotted lines and “T.” Neither trachea nor spine (“S”) is compressible. Thus, the un-burped air under pressure bulges the esophagus laterally. The esophagus of this patient is estimated to have stretched laterally (arrows) to 3 or 4 times the diameter of the trachea!
Esophagus, After Total Laryngectomy
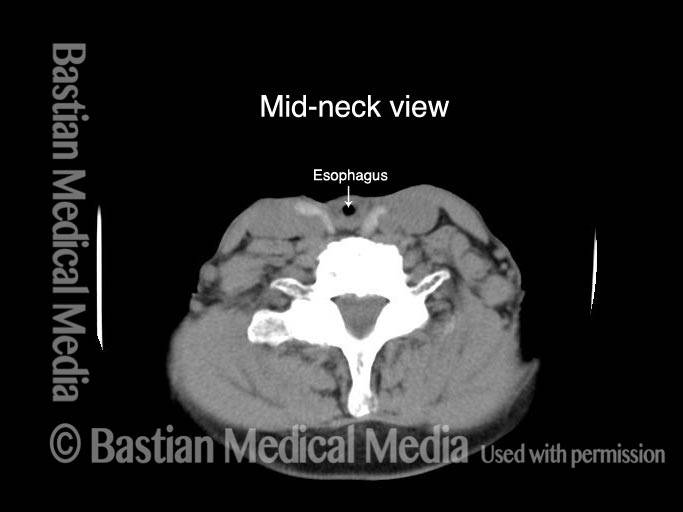
Esophagus, after total laryngectomy (1 of 4)
After total laryngectomy. At the level where larynx was, there is no airway seen. The small air collection (at arrow) is within the reconstructed esophagus, at the level of the neck.
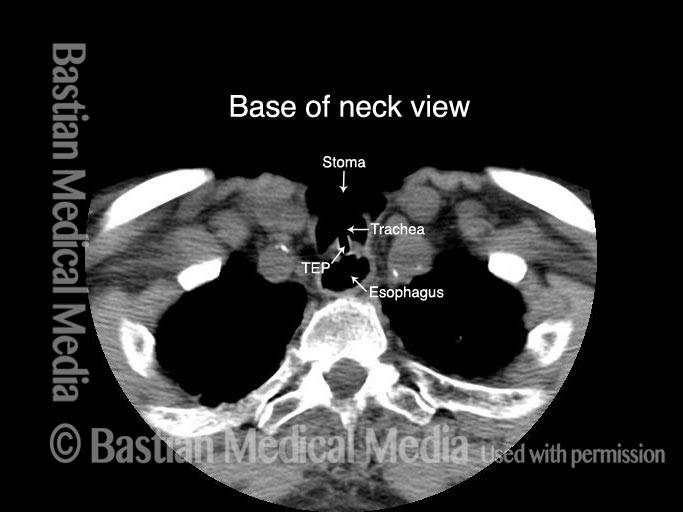
Esophagus, after total laryngectomy (2 of 4)
At the base of neck, the trachea has been sutured forward to neck skin. In this view, the tracheoesophageal prosthesis (TEP) can be seen traversing the shared tracheoesophageal party wall. In this view, the esophagus is very dilated with air.
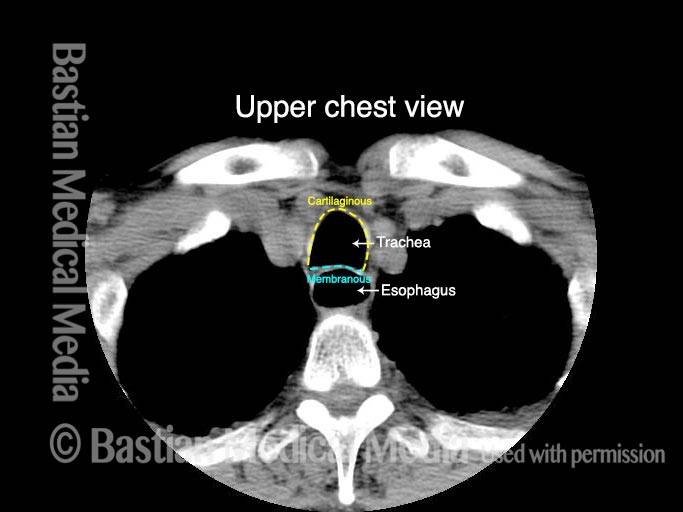
Esophagus, after total laryngectomy (3 of 4)
Below the tracheostome, the entire trachea is again seen. The horseshoe-shaped anterior segment of the trachea’s wall, two-thirds of the total circumference, is the trachea’ s cartilaginous component. The posterior one-third is the membranous trachea, which also constitutes the anterior one-third of the esophagus, and is also called the tracheoesophageal party wall. The esophagus is again dilated with air here.
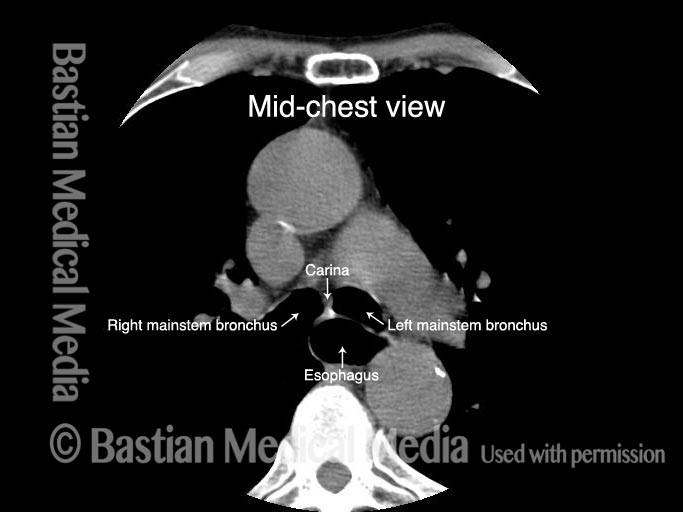
Esophagus, after total laryngectomy (4 of 4)
At the mid-thoracic level, the trachea is splitting into the two mainstem bronchi, and the esophagus is still seen due to dilation with swallowed air.
Endoscopic View of Esophageal (Acid) Reflux
Liquid in the lower esophagus (1 of 2)
After swallowing blue food-colored water, it sits momentarily in the lower esophagus waiting to enter the stomach. The saliva bubbles indicated by arrow and dotted lines are for reference with the next photo.

Acid reflux in the lower esophagus (2 of 2)
A moment later, without effort or gag, the blue water refluxes (zooms upwards from the lower esophagus and stomach) towards the stationary camera chip. If this occurred with acidic stomach contents, the esophagus would suffer chemical irritation and the patient might experience “heartburn.”

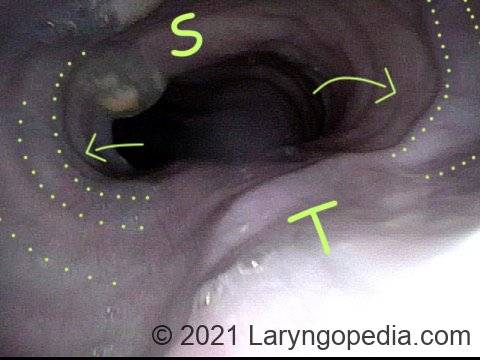
Dramatic Dilation of the Esophagus in A Person with R-CPD Due to Buildup of Swallowed Air that He Cannot Belch to Get Rid Of
View of the mid-esophagus (1 of 2)
This view in the mid-esophagus was obtained with a 3.6mm scope without an air channel. The dilation is from the patient’s own unbelchable air. Note quite major lateral dilation of the esophagus, indicated by concentric dotted lines and arrows. Dilation is not possible in the direction of unyielding spine (S) and trachea (T).
View of the mid-esophagus (2 of 2)
A view that shows more clearly the indentation of trachea (T). Persons with this much dilation of esophagus often complain as much of chest pressure as they do abdominal bloating. This man has experienced “large” reduction of R-CPD symptoms after botulinum toxin injection into his upper esophageal sphincter (cricopharyngeus muscle).