An abnormal, continuous sheet of mucosa that joins the vocal cords together. This glottic web is analogous to the web one sees between adjacent fingers. Normally, in the absence of a glottic web, the mucosa covers each vocal cord individually to form a crisp “V”.
A glottic web may be congenital, or it may result from injury. Classic teaching is that surgeons ought not to operate on the anterior portion of both vocal cords simultaneously, because the raw, de-epithelialized surfaces may grow together and create an anterior glottic web. Some webs do not need to be addressed because the effect on voice is minimal; in other cases, surgical approaches are indicated because of the poor voice often associated with this abnormality.
Glottic web, divided and treated with steroid injections
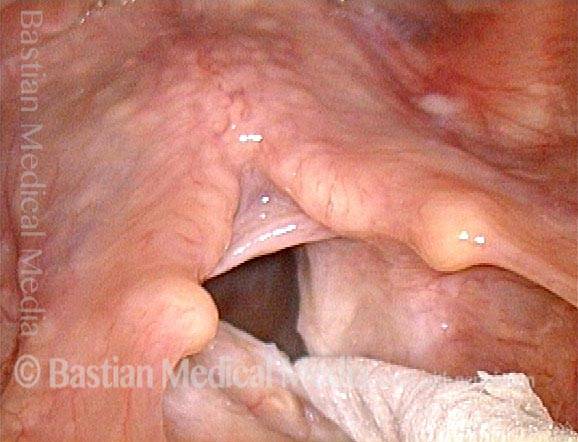
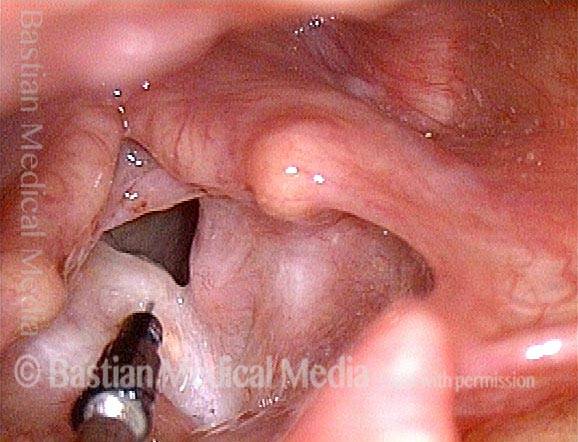
Glottic web (1 of 12)
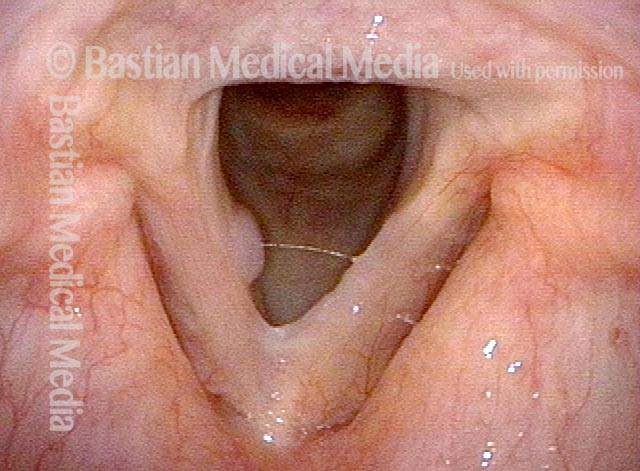
Glottic web, inflammatory, progressive, without antecedent trauma.

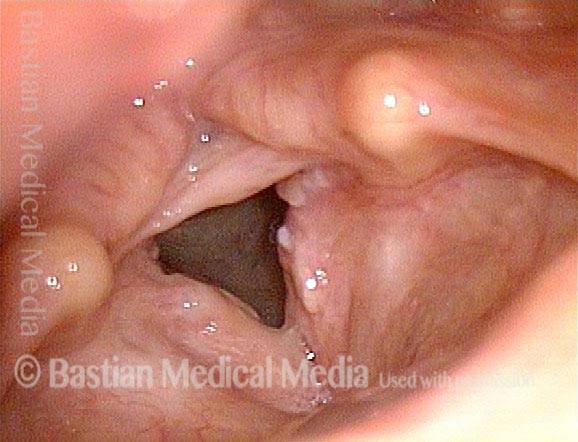
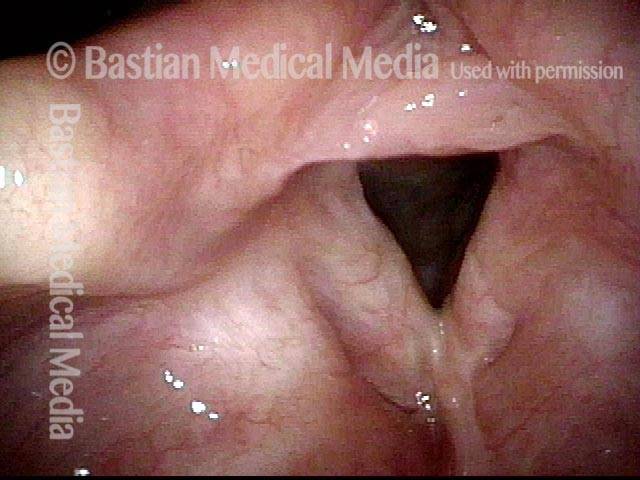
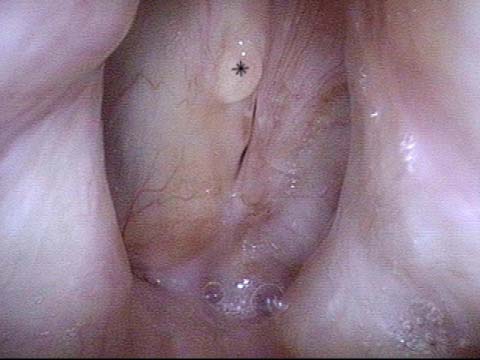
Glottic web (2 of 12)
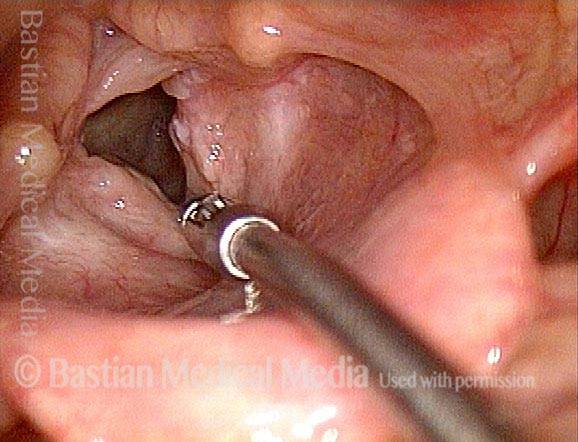
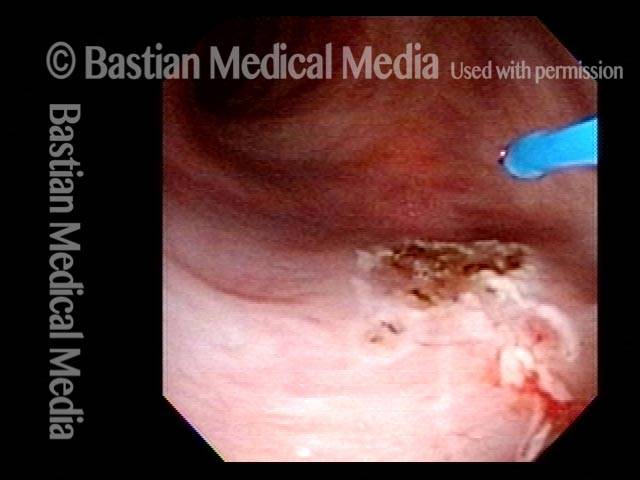
Lab procedure: 11-blade attached to biopsy forceps, wrapped with tape to “guard” all but the tip.

Glottic web (3 of 12)
Web partially divided.
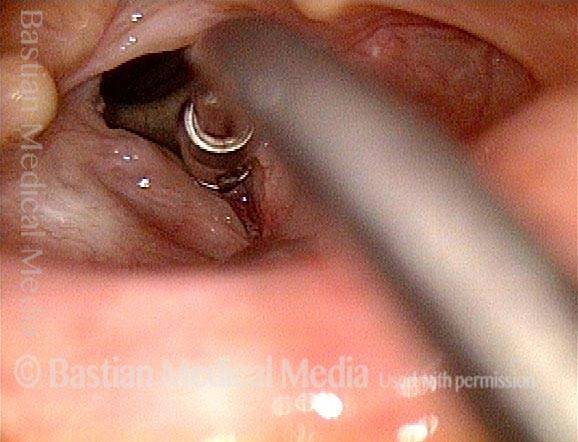
Glottic web (4 of 12)
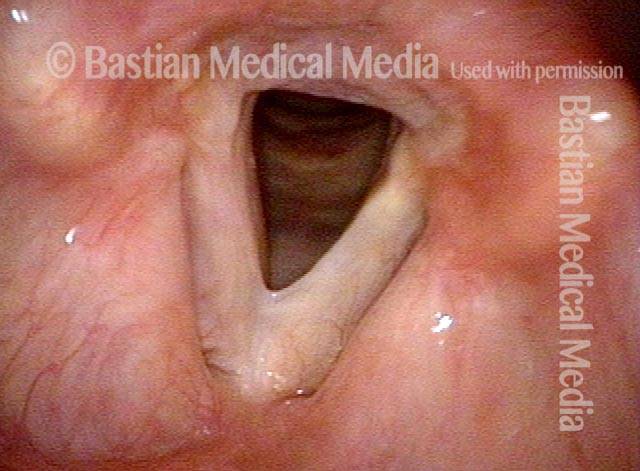
Web fully divided.

Glottic web (5 of 12)
Vocal cords are re-adhering where the web was divided two weeks earlier.
Glottic web (6 of 12)
Biopsy forceps used to separate the adhesion.
Glottic web (7 of 12)
Slight bleeding at point of re-separation of the cords.
Glottic web (8 of 12)
Result (compare with photo 5).

Glottic web (9 of 12)
A depot form of steroid injection in the videoendoscopy laboratory (patient in chair). The intent is to abolish or diminish the inexorable re-adhesion of the vocal cords, sometimes many months after apparent complete healing and re-mucosalization. Note white submucosal material.
Glottic web (10 of 12)
Injection at apex of the web. Note condensed white submucosal steroid, from prior injection.

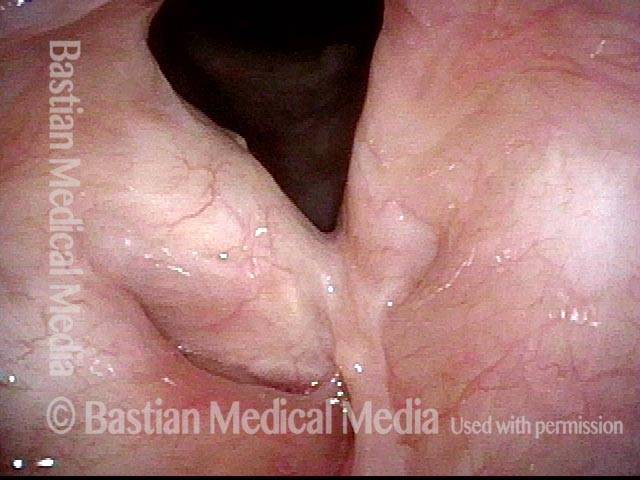
Glottic web (11 of 12)
16 months after last of a series of web divisions as depicted above. The web does not show any sign of re-forming. Compare with photos 1 and 2.
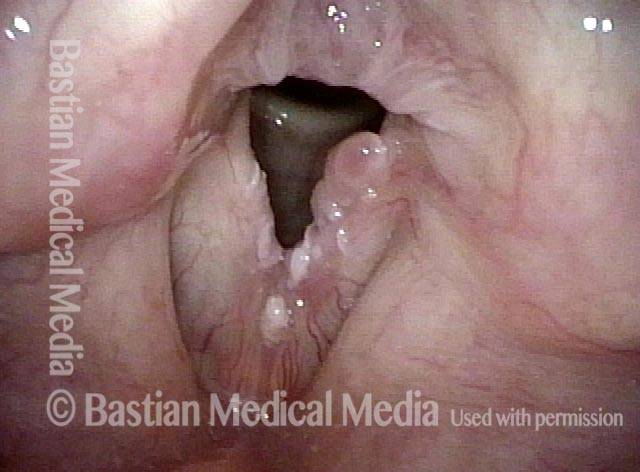
Glottic web (12 of 12)
Closer view, again showing maintenance of the deep "V" shape of the glottic aperture, rather than the short, fat "U" seen before web division. The patient has no shortness of breath.
Inflammatory Glottic Web Without Known Cause
Inflammatory web (1 of 4)
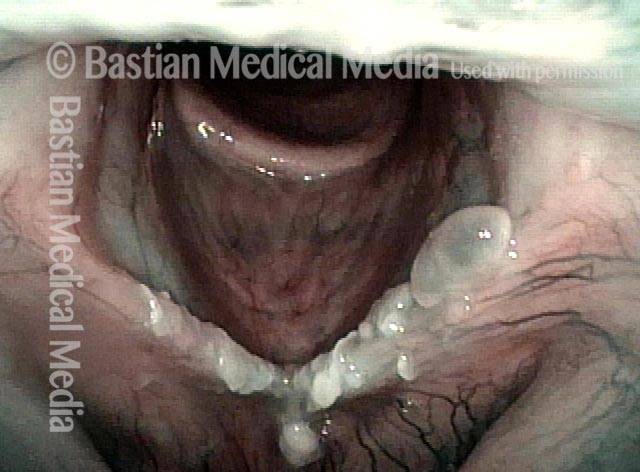
Chronic hoarseness and peculiar inflammatory web in a woman who has never smoked. Acid reflux has been put aside as a cause, too. Biopsies show severe inflammation and dysplasia. HPV subtyping was negative.
Closer view (2 of 4)
Closer view under narrow band illumination shows the combination of inflammation, granulation, and leukoplakia.
After treatment (3 of 4)
Soon after superficial peeling of the abnormal tissue, kenalog injection, and mitomycin C application. The web is less; voice is much better, but inflammation remains significant.
Closer view (4 of 4)
A closer view of the chronically inflamed cords. In cases of idiopathic (unknown cause) inflammatory webs of this sort, the rule is gradual recurrence of the web not in the early postoperative period as is seen with conventional webs, but instead across many months. Occasionally, transformation to CIS or early cancer then opens the door to radiation therapy.

Web After Radiotherapy
Post radiation (1 of 2)
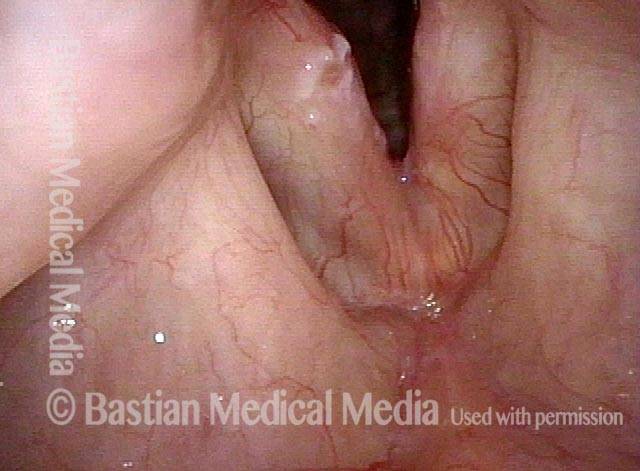
More than a year after radiation and chemotherapy for HPV-induced larynx cancer, voice is serviceable but still hoarse. The vocal cord mucosa would have been raw from the radiation, and fused together anteriorly.
Anterior band (2 of 2)
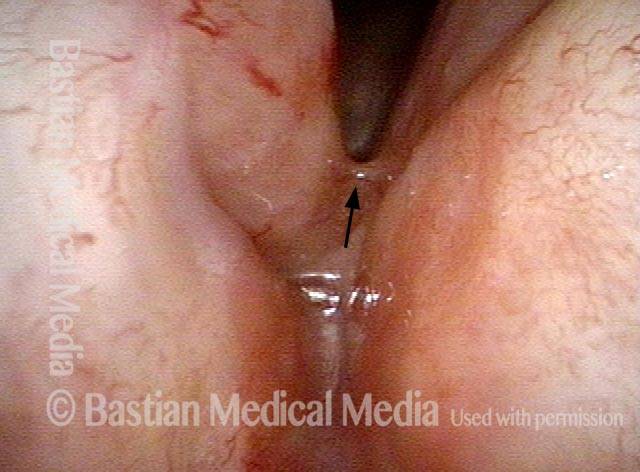
At closer range, the band between the anterior vocal cords is clearly seen. The vocal cords should be unattached to approximately the tip of the arrow.
Glottic Web from Birth
Glottic web (1 of 4)
This younger woman has been hoarse from birth and has had four prior procedures elsewhere for her congenital glottic web. Here, note that the web attaches most of both vocal cords together. She is very hoarse. The large and small dots are for orienting purposes with following photos. The recommendation: start with simple outpatient web division.
Surgical division of web (2 of 4)
A few weeks after surgical division of the web, topical mitomycin C, early postop voice use to prevent reattachment. Voice is already noticeably improved. As expected, there is a small web re-forming, but well below the margins of the cords (at 'X').
Polyp-like mounds (3 of 4)
Under strobe light, the stretched web tissue has retracted after division into polyp-like mounds, especially on the right side (left of photo).
Complete healing (4 of 4)
Four months later, with complete healing and a residual subglottic web that does not interfere with vibration. The patient says voice improvement is “moderate” for both quality and effort required. She also noted that “people no longer ask me if I’m sick.” She does not feel the need to attempt any further improvement via trimming for better match.
Glottic Web After Surgery
Cyst and web (1 of 4)
After surgery elsewhere, a glottic web and mucus cyst. The original laryngeal condition that led to surgery is not known.
Surgical division of web (2 of 4)
A few weeks after surgical division of the web, topical mitomycin C, early postop voice use to prevent reattachment. Voice is already noticeably improved. As expected, there is a small web re-forming, but well below the margins of the cords (at 'X').

Coagulating cyst (3 of 4)
Given her prior bad experience with surgery, the patient was unwilling to go to the operating room to address the web, but was willing to address the cyst in the voice lab, using the Thulium laser. The cyst originates from well below the vocal cord, and can therefore be coagulated without risk to voice.
Complete healing (4 of 4)
Four months later, with complete healing and a residual subglottic web that does not interfere with vibration. The patient says voice improvement is “moderate” for both quality and effort required. She also noted that “people no longer ask me if I’m sick.” She does not feel the need to attempt any further improvement via trimming for better match.
Glottic web—Take A Simple Approach First, Not A Keel

Nuances “Gleaned” From Daily Examinations
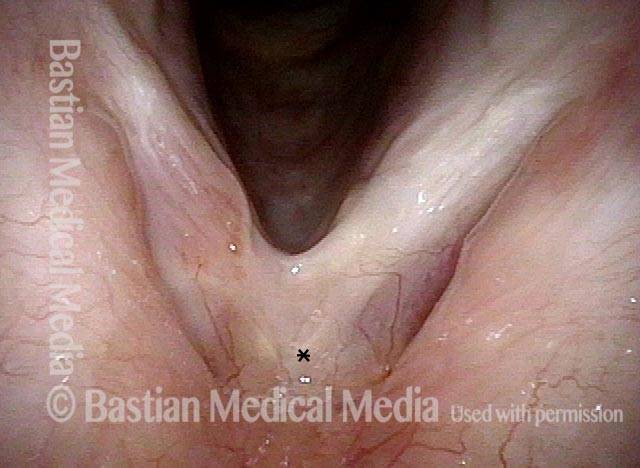
Vocal "overdoer" (1 of 4)
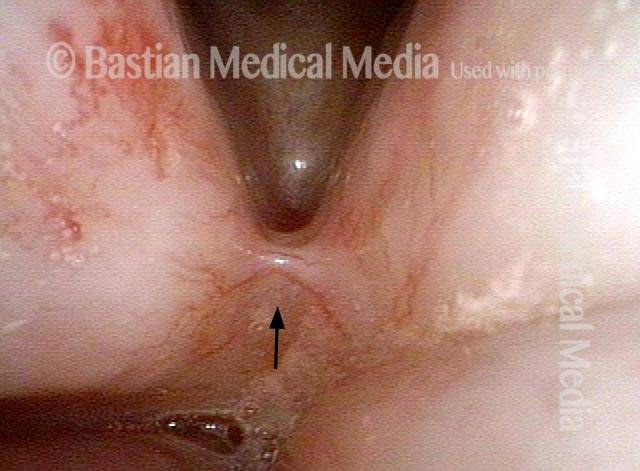
A vocal “overdoer” with hoarseness. Note broad-based swelling of both vocal cord margins. A microweb, thought to be congenital, is also seen at the arrow. Tiny dots indicate a subtle wrinkle or shallow sulcus.
Inspiratory phonation (2 of 4)
The patient has been asked to produce inspiratory phonation to reveal the translucent polyp and “sulcus,” again at tiny dots.
Translucent polyp (3 of 4)
Under strobe light, the translucence of the polypoid elevation is seen more clearly.

Open phase (4 of 4)
At open phase of vibration again under strobe light, the broad based left vocal cord elevation is also seen.

Glottic Web Management Without A Keel
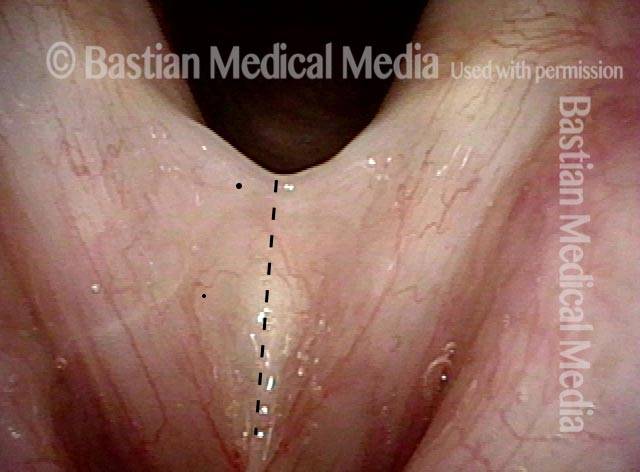
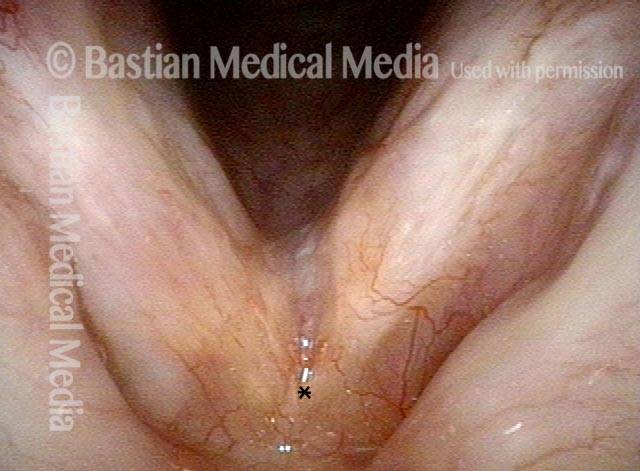
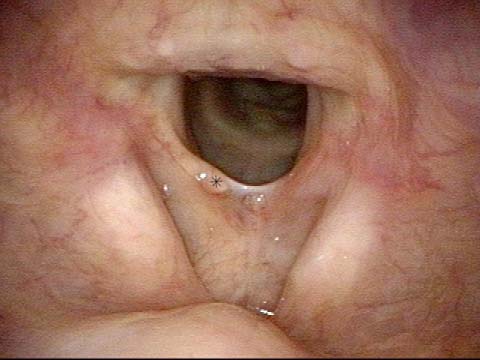
Glottic Web (1 of 7)
More than a year after laser excision elsewhere of a small vocal cord cancer, this man has a web joining the anterior half of the vocal cords. Voice is a whisper. A simple division with a microscissor is worthwhile before contemplating something more invasive, such as insertion of a keel.
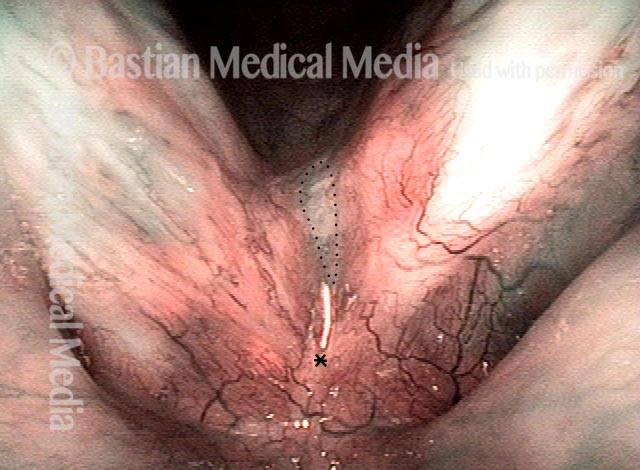
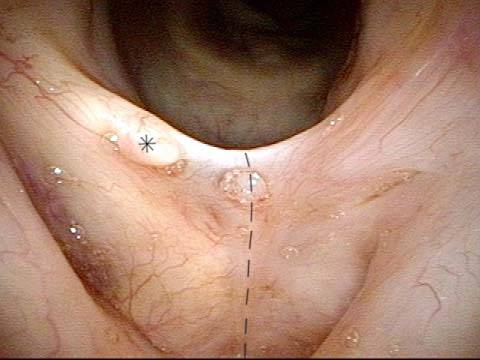
Glottic Web (2 of 7)
A closer view. The dotted line indicates the proposed division. The tag of extra tissue at * in all photos is not to be disturbed, preferring to preserve all tissue until the mucosa’s vibratory ability could be assessed.
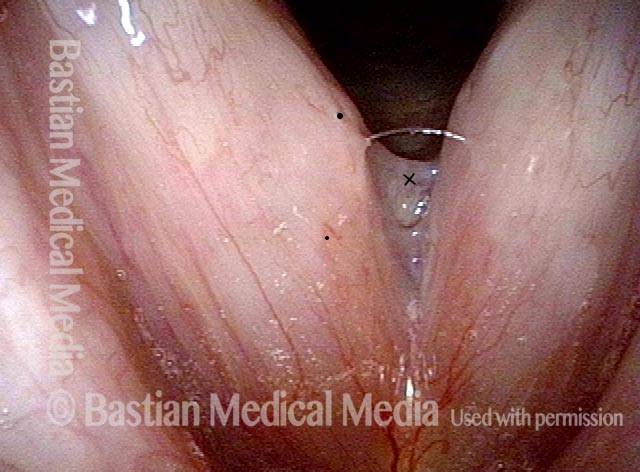
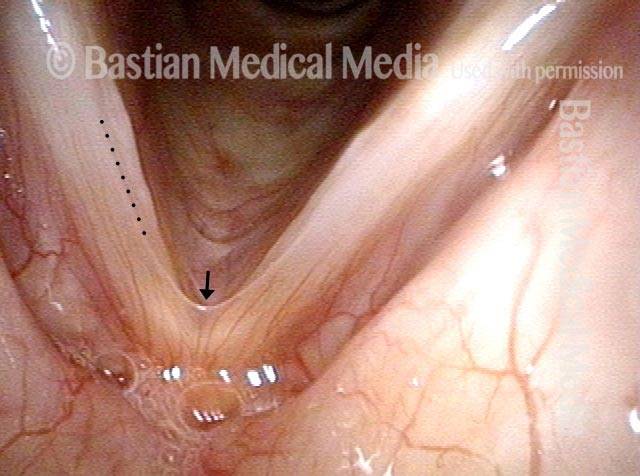
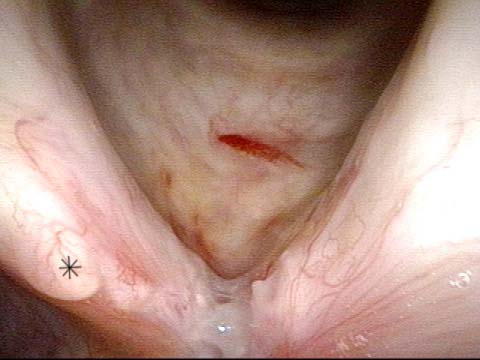
Glottic Web (3 of 7)
A week after that simple endoscopic division of the web, steroid injection, and topical mitomycin C application. The anterior vocal cords have not yet re-mucosalized. Voice is remarkably functional.
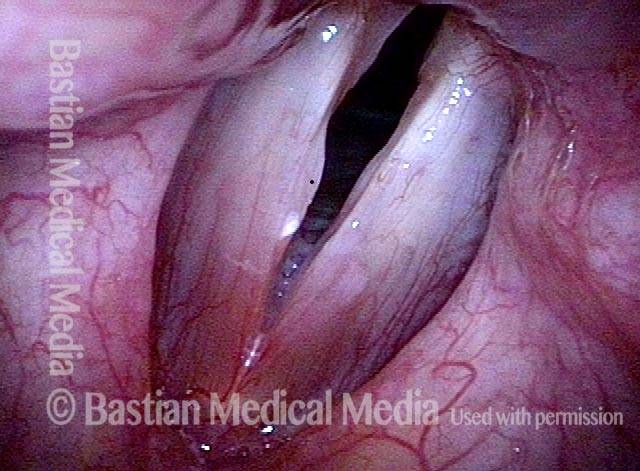
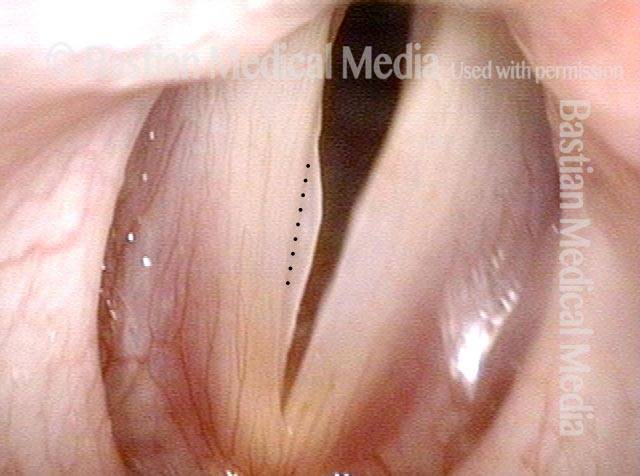
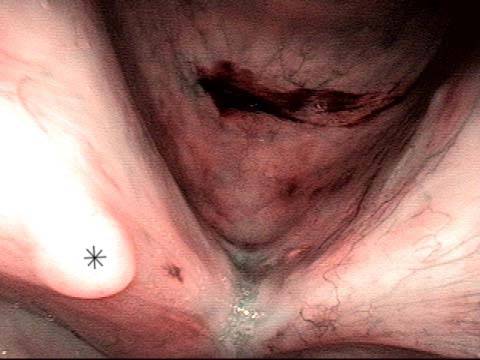
Glottic Web (4 of 7)
Approximately 3 weeks after division, voice remains very good. Compare with photo 1.

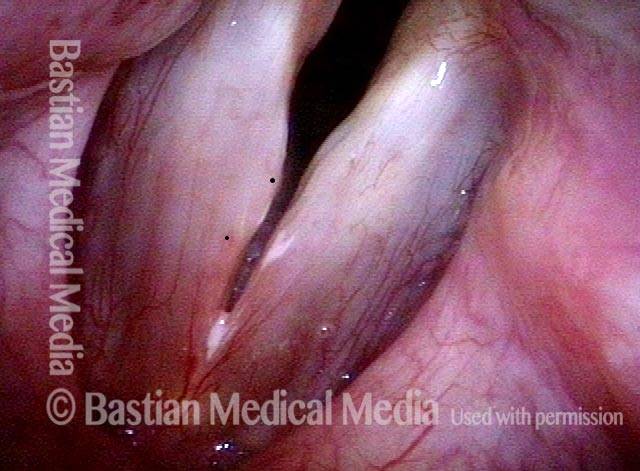
Re-grown mucosa (5 of 7)
Only a small part of the cut surface is not yet covered with new mucosa. This photo is illuminated with narrow band (blue-green) light to accentuate capillaries on re-grown mucosa.
Closed phase of vibration (6 of 7)
Under strobe light, the closed phase of vibration.
Restoration of oscillatory ability (7 of 7)
Open phase of vibration, showing restoration of oscillatory ability on both cords. Voice remains rough but highly functional without syllable dropouts or “effort” in the quality.
