Indicator lesions are visual findings of vibratory injury in a person who has no current voice complaints, and whose “swelling checks” are normal.
Background:
Individuals who fit the “vocal overdoer profile” may only notice vocal limitations caused by vibratory injury on an occasional and transient basis. These episodes may be brushed off as insignificant, because they are so brief, and recovery so complete. Even while asymptomatic, however, such individuals may have subtle visual findings of vibratory injury—“Indicator lesions.” Unless discovered during a screening examination for entry to music studies, the individual may be unaware of these findings. What if indicator lesions are found? Suggested responses:
1. Make sure the individual understands that these are indicator lesions and as such constitute a “yellow flag” suggesting at least occasional overuse of voice.
2. Define the “vocal overdoer syndrome” for the person as the combination of and interaction between an expressive, talkative, extroverted personality and a “vocally busy” life. Said another way, there may be both intrinsic, personality-based and extrinsic, vocal commitment based reasons that amount and forcefulness of voice may be excessive. A 7-point talkativeness scale can be used to estimate the intrinsic risk, where “1” represents Clint Eastwood, “4” the averagely talkative person, and “7” the life of the party. The extrinsic risk is addressed by making a list of vocal commitments such as for occupation, childcare, hobbies, social activities, religious practice, athletics/ sports, and rehearsal and performance.
3. Discuss the symptom complex of mucosal injury:
a) Loss/ impairment of high, pianissimo singing;
b) Day-to-day variability of vocal clarity and capability;
c) A sense of increased effort to produce voice;
d) Reduced mucosal endurance, or becoming “tired” vocally from amount/ manner of voice use that does not seem to induce this in others;
e) Phonatory onset delays—the slight hiss of air that precedes the beginning of the sound, especially if high and soft. Speaking voice hoarseness can be a fairly late and gross symptom of mucosal injury.
4. Talk about managing the amount, manner, and spacing of voice use to reduce unnecessary wear and tear on the vocal cord mucosa.
5. Teach vocal cord swelling checks as a means of detecting even subtle injury. Respond to what they tell you!
Singers are understandably distressed when they discover even the tiniest mucosal swelling such as indicator lesions. That is because for true singers, singing is not just what they do; the term “singer” also defines who they are. So injury threatens both activity and identity. Consequently, discuss indicator lesions with great care and sensitivity. Keep in mind that some doctors speak of “small vocal nodules that do not interfere with singing.”
Small nodules that are but a tiny step above indicator lesions, especially when spicule-shaped rather than fusiform, always exact a penalty to the singing voice (see #3 above), but limitations can often be concealed by warming up, and singing more loudly. Singers often say “I have a big voice that doesn’t do pianissimo.” That is, pp becomes p; mp becomes p; mf becomes f; and so forth. Alternatively, the singer considers the missing pianissimo to be a technical fault.
Indicator Lesions and MTD
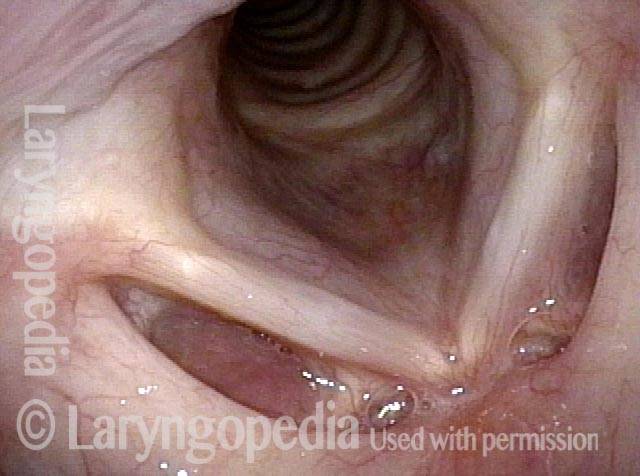
Breathy voice (1 of 6)
Phonation (2 of 6)

Open phase (3 of 6)
Closed phase (4 of 6)
Open phase, indicator lesions (5 of 6)

"Closed" phase, MTD (6 of 6)
Indicator Lesions
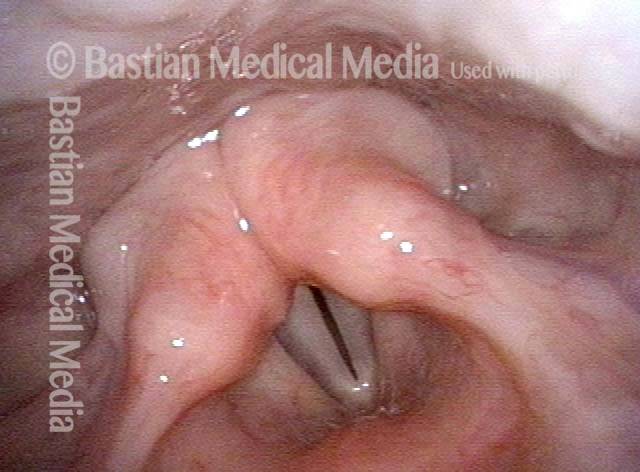
Middle-aged teacher (1 of 4)
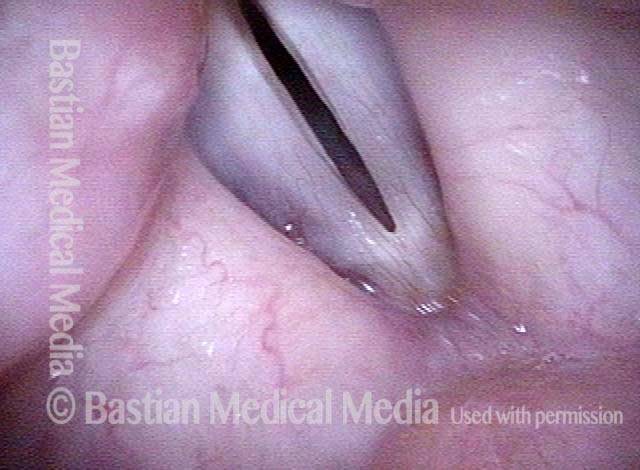
Phonatory view (2 of 4)

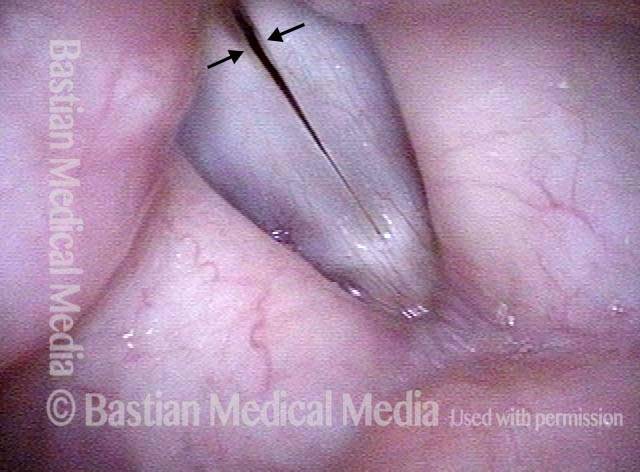
Pre-phonatory instant (3 of 4)
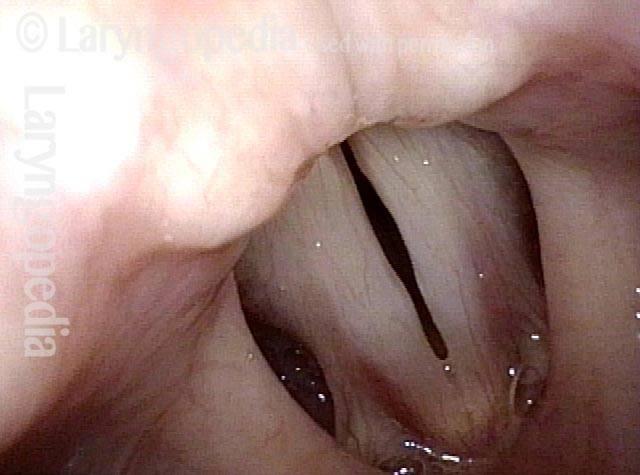
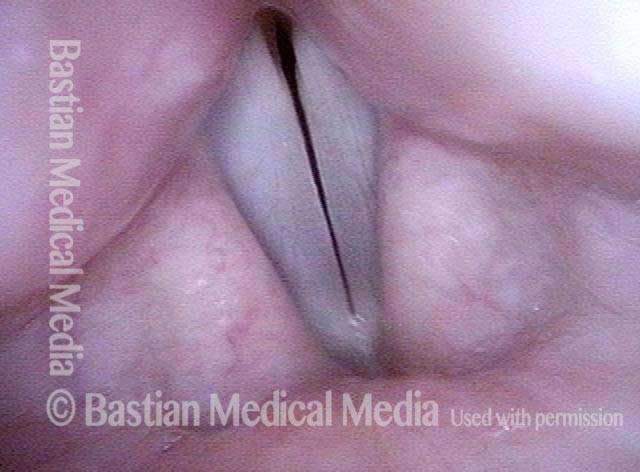
Indicator swellings (4 of 4)
