Leukoplakia (leuko = white; plakia = plaque) is a white patch found on the mucosa anywhere in the body. In the larynx, it is most often seen on the vocal cords, either in long-time smokers or in individuals with some other cause of chronic inflammation, such as (controversially) acid reflux.
Leukoplakia is the visually descriptive term for what, on biopsy, may prove to be keratosis, carcinoma in situ, or carcinoma. Unfortunately, it is a stubborn and frustrating problem in laryngology, with a tendency to recur after removal.
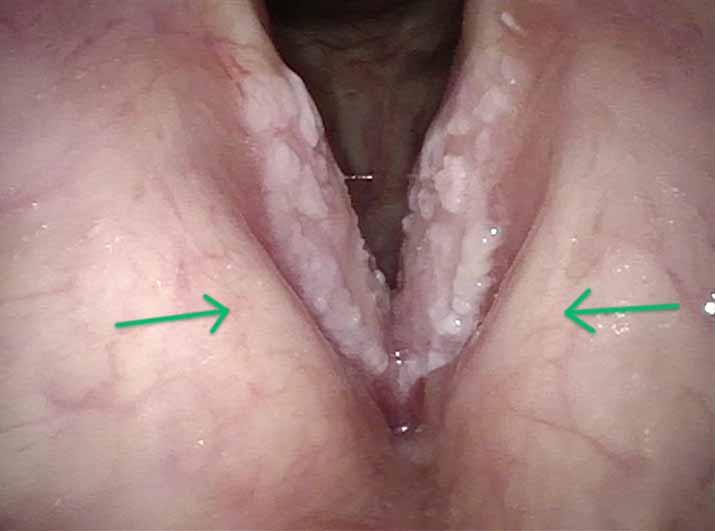
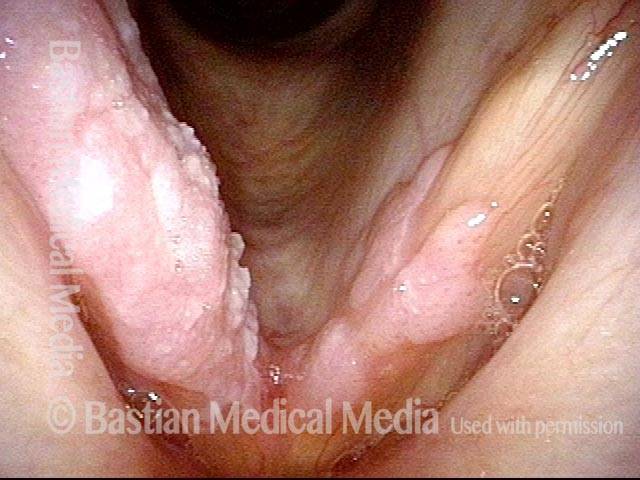
Cake Icing and Spilled Milk Leukoplakia after Covid in a Former Smoker
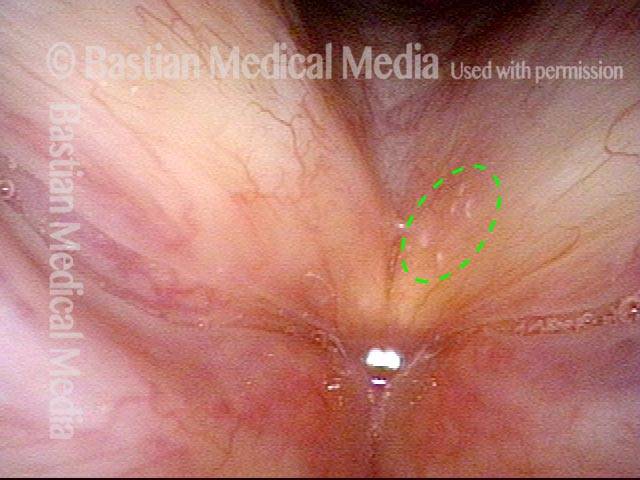
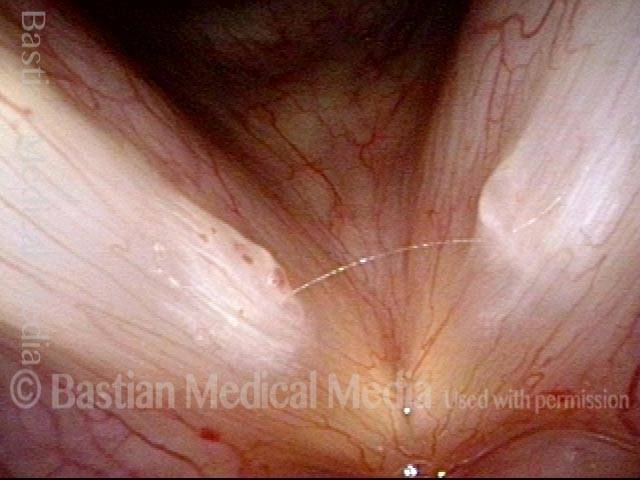
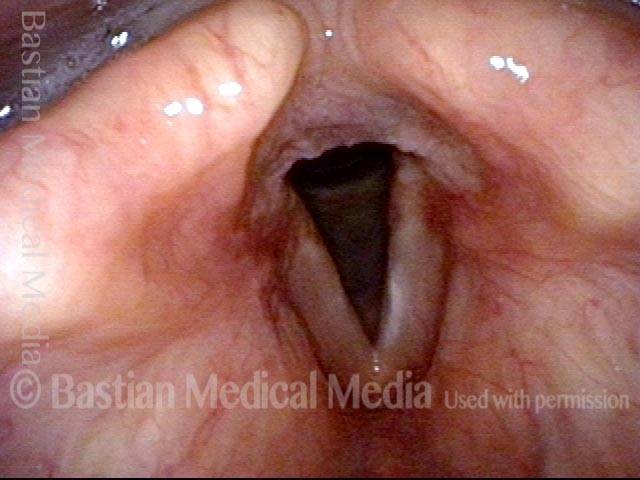
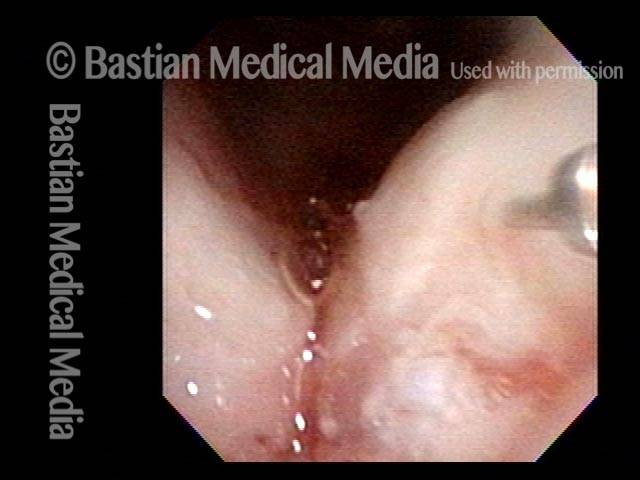
This is a person who had smoked ½ pack per day for a little over a decade but stopped nearly 15 years ago. Voice was always normal until Covid-19 infection (despite vaccination). Laryngitis occurred during that illness and never resolved across six months to the time of this examination. He is hoarse but voice is functional for basic communication. After supportive (acid reflux, etc.) treatments failed to resolve these lesions, microlaryngoscopy with meticulous “basement membrane” peeling of these lesions will follow.
Leukoplakia (1 of 7)
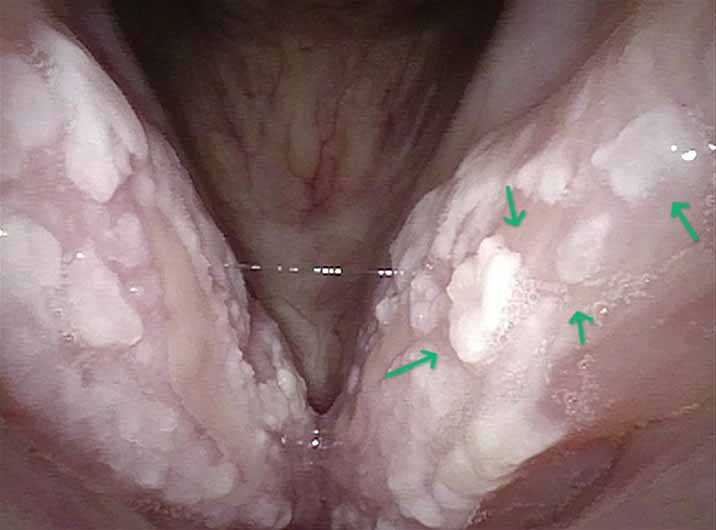
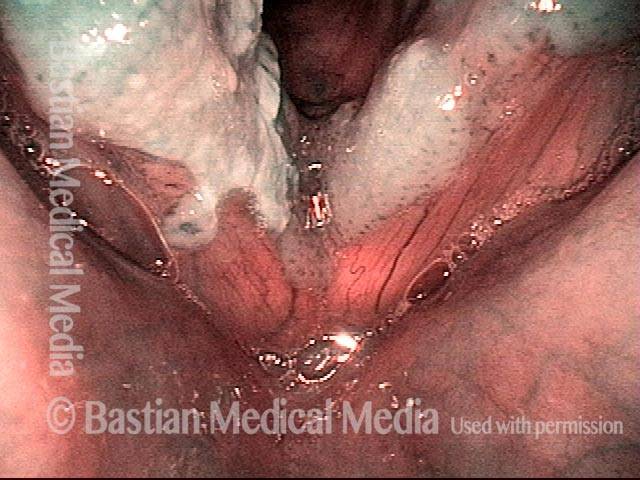
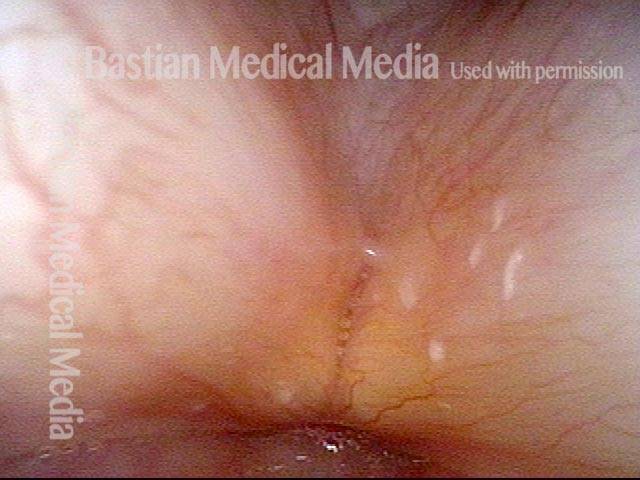
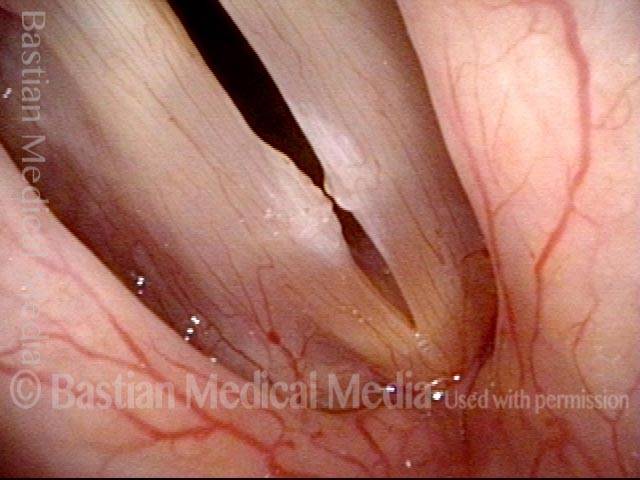
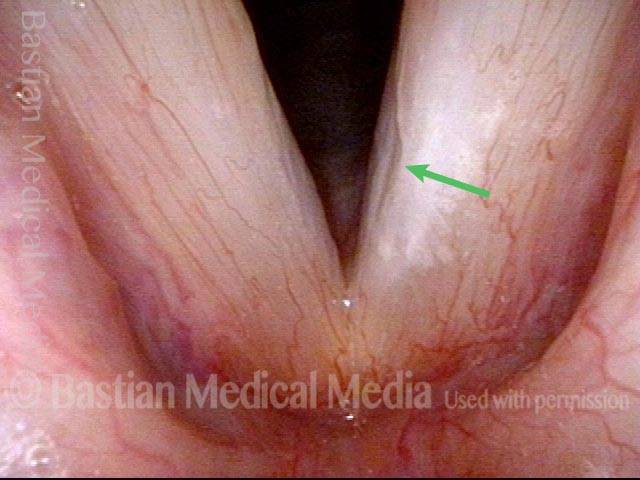
Spilled milk Leukoplakia (2 of 7)
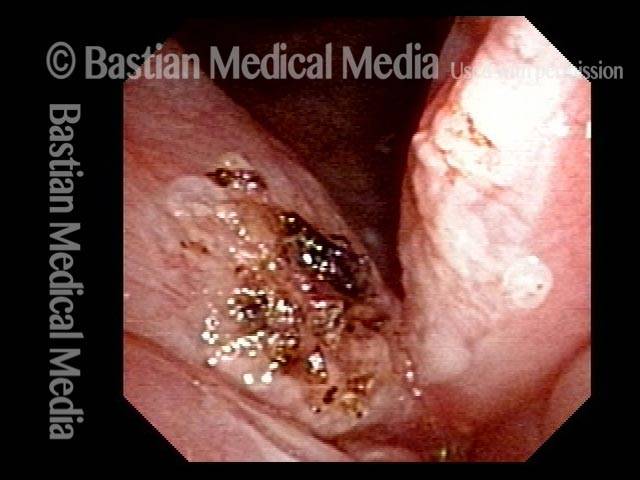
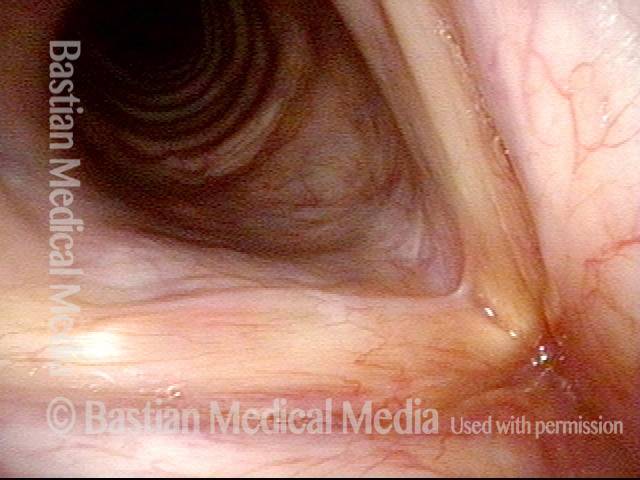
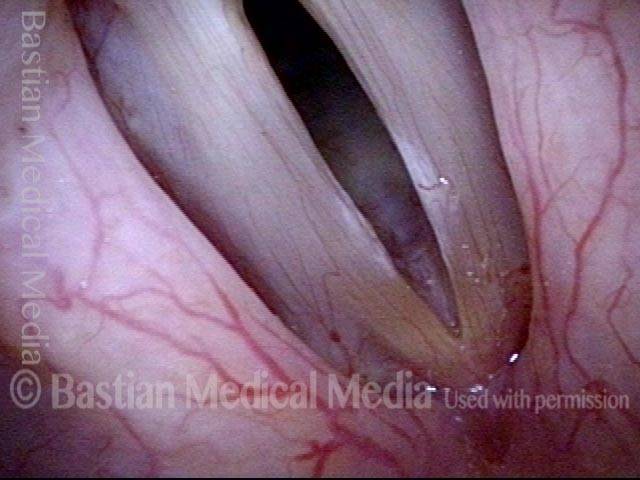
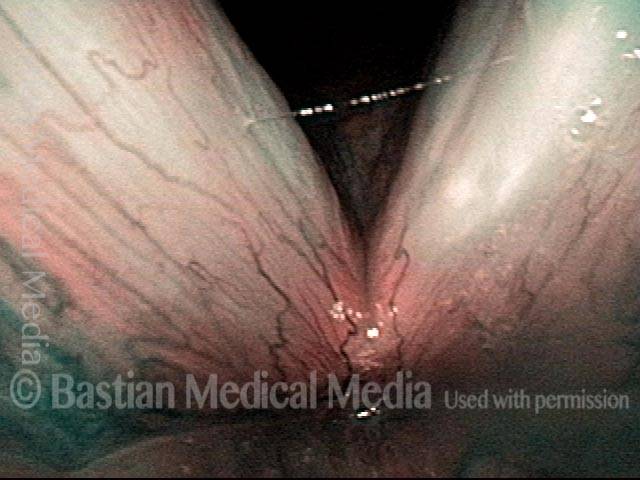
Superficial ulceration (3 of 7)

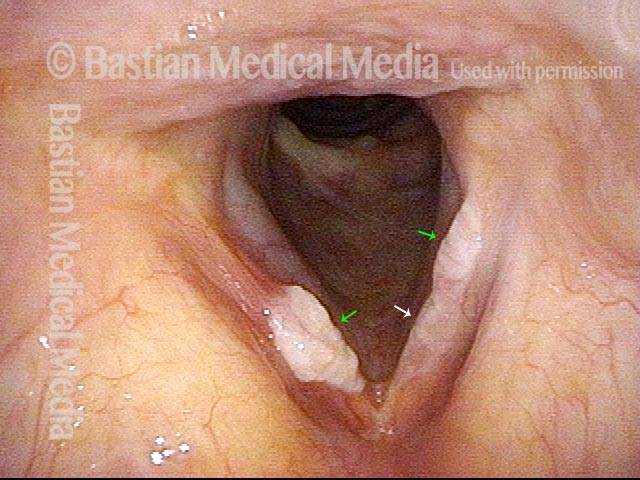
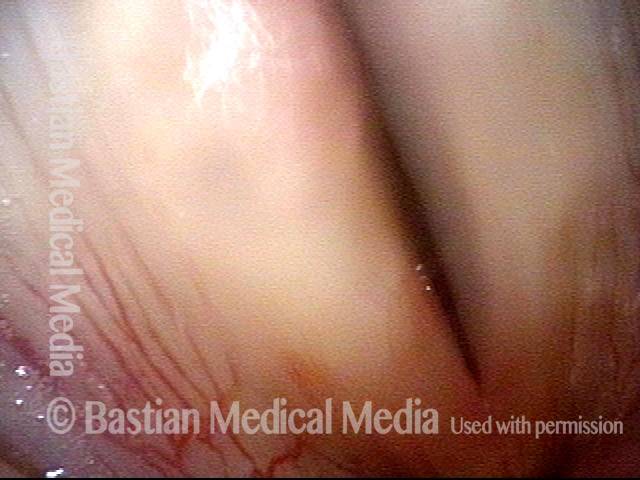
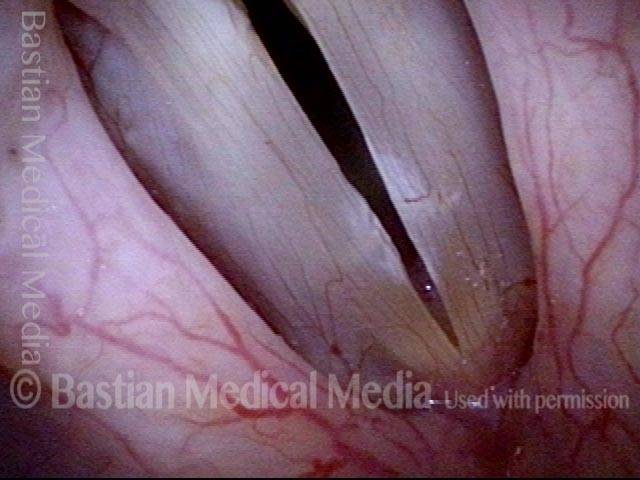
Closed phase of vibration (4 of 7)

Stiff mucosa limits vibration (5 of 7)

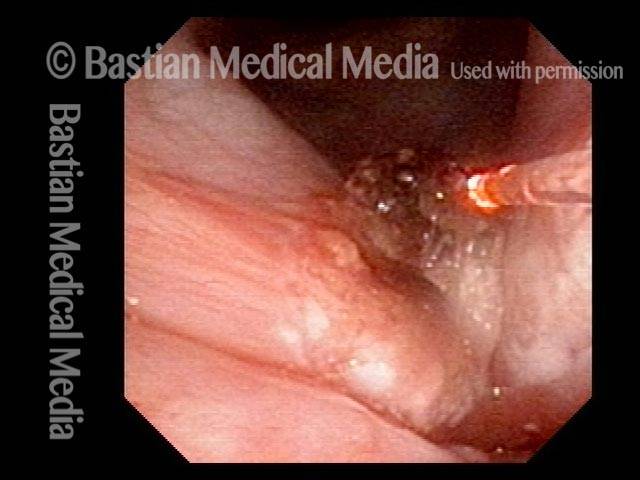
Leukoplakia diminishes (6 of 7)

Residual leukoplakia (7 of 7)

More examples of Leukoplakia
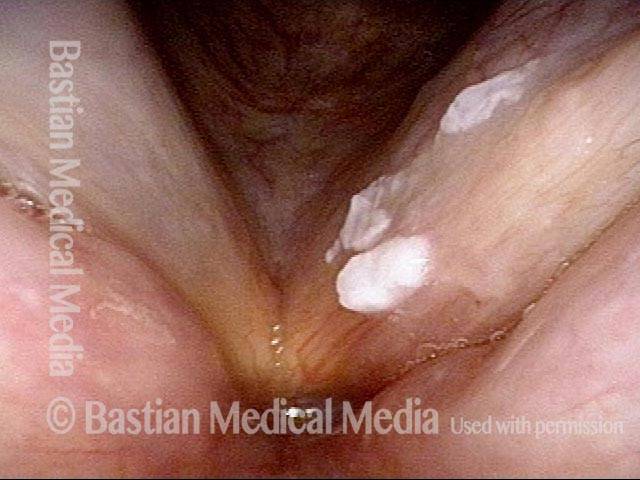
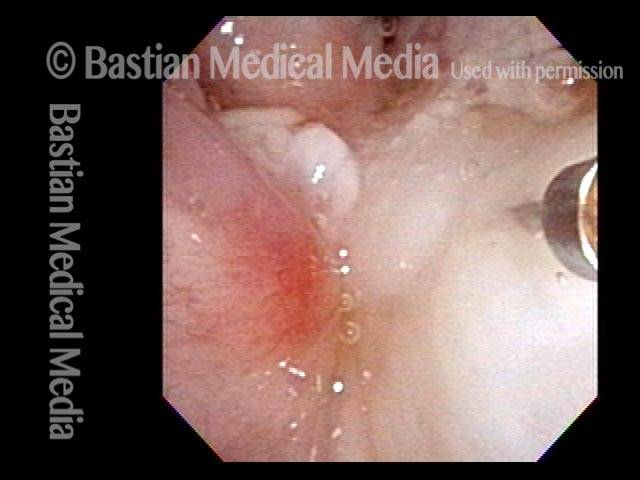
Cake-icing Leukoplakia (1 of 4)
Hazy Leukoplakia (2 of 4)
Leukoplakia (3 of 4)

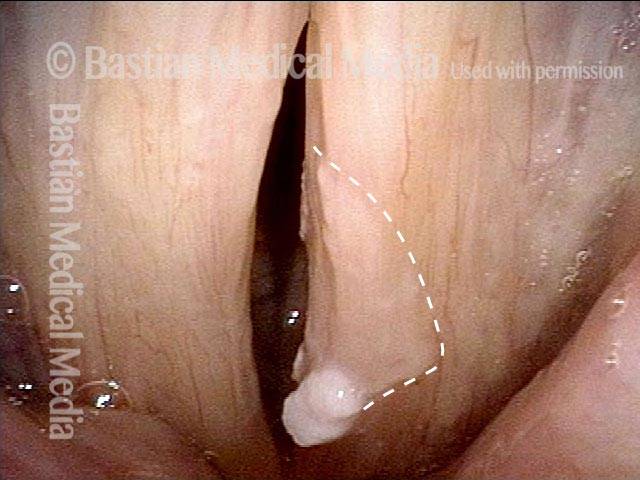
Closer look (4 of 4)

Example 2
Leukoplakia (1 of 2)

Leukoplakia (2 of 2)

Leukoplakia, Before and After Surgical Removal
Diffuse Leukoplakia (1 of 4)
HPV effect (2 of 4)
Leukoplakia, after surgical removal (3 of 4)

Leukoplakia, after surgical removal (4 of 4)

Leukoplakia Battled Over Time
Leukoplakia (1 of 8)
Spilled Milk (2 of 8)

Thulium laser (3 of 8)
Coagulated tissue (4 of 8)
Leukoplakia (5 of 8)

Detachment (6 of 8)
Superficial vascular pattern (7 of 8)
Coagulated tissue (8 of 8)

Leukoplakia, Before, During, and After Laser Coagulation
Leukoplakia, not yet seen (1 of 6)
Leukoplakia (2 of 6)
Leukoplakia (3 of 6)
Leukoplakia, coagulated by laser (4 of 6)

Leukoplakia, 3 months after laser treatment (5 of 6)
Leukoplakia, 3 months after laser treatment (6 of 6)
Vocal Nodules, Leukoplakia, and Capillary Ectasia
Vocal nodules, leukoplakia, and capillary ectasia (1 of 4)
Vocal nodules, leukoplakia, and capillary ectasia (2 of 4)
Vocal nodules, leukoplakia, and capillary ectasia: 6 months later (3 of 4)
Vocal nodules, leukoplakia, and capillary ectasia: 6 months later (4 of 4)
Glottic Furrow / Leukoplakia / Acid Reflux
Glottic furrow / Leukoplakia / Acid reflux (1 of 4)
Leukoplakia (2 of 4)
Glottic furrows (3 of 4)
Gap during closed phase (4 of 4)

Thulium Laser Surgery, With Local Anesthetic Injection, to Treat Leukoplakia
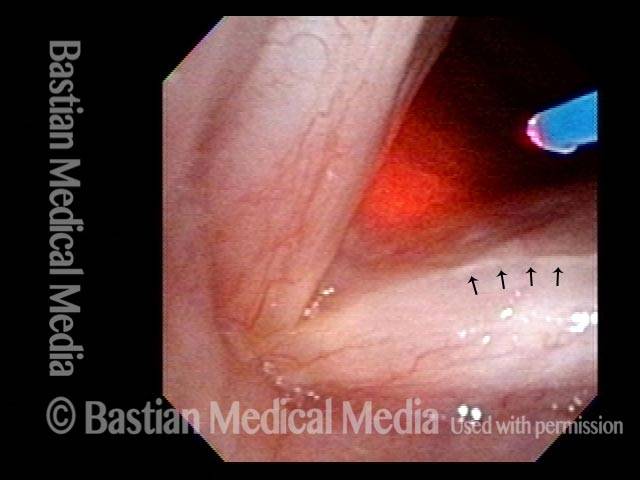
Leukoplakia, about to be treated with laser (1 of 4)

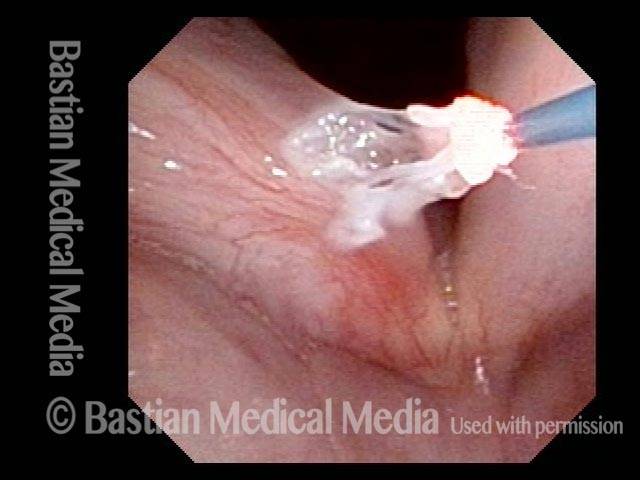
Injection of local anesthetic (2 of 4)
Injection of local anesthetic (3 of 4)
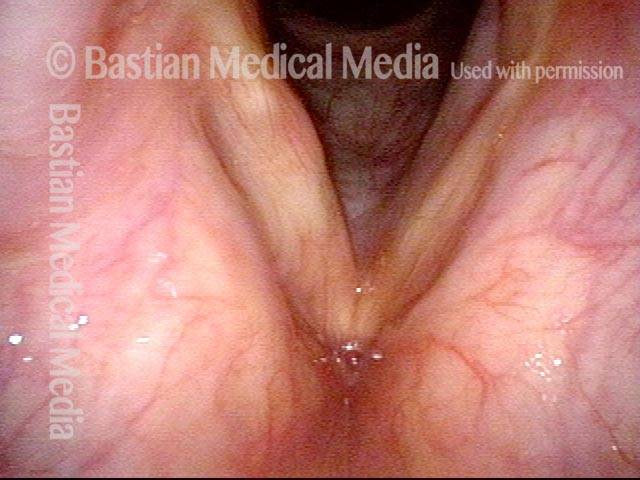
Right after thulium laser treatment (4 of 4)

Leukoplakia Biopsy
HIV Testing (1 of 2)

Biopsy (2 of 2)

Narrow-band vs. Standard Light: Leukoplakia
Narrow-band vs. standard light: leukoplakia (1 of 2)

Narrow-band vs. standard light: leukoplakia (2 of 2)
