Nonorganic Breathing Disorder, Tracheal
Nonorganic breathing disorder, tracheal (1 of 2)
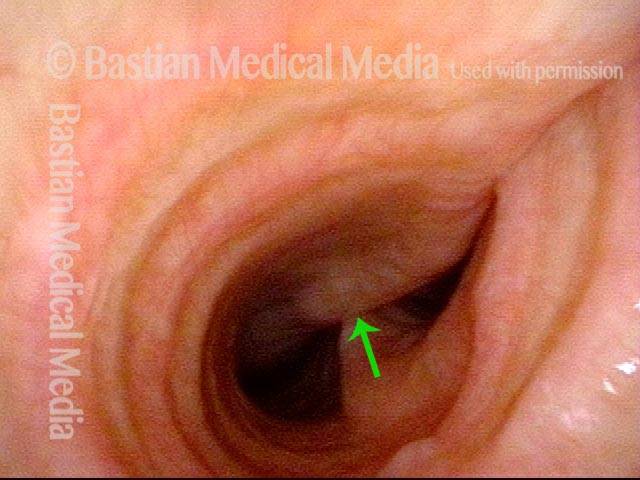
Distal trachea, showing the carina (middle arrow), where the trachea (or windpipe) divides into the two mainstem bronchi. The membranous tracheal wall is flexible, and beginning to bulge forward functionally (under patient control).
Nonorganic breathing disorder, tracheal (2 of 2)
On expiration, there is anterior bulging (arrows) of the tracheoesophageal party wall, to the point of largely obstructing the mainstem bronchi. Air moving through this functionally narrowed space can cause wheezing on a non-organic basis. Wheezing will be much louder with auscultation over the manubrium, than on listening in the peripheral lung fields.
Example 2
Nonorganic breathing disorder, tracheal (1 of 2)
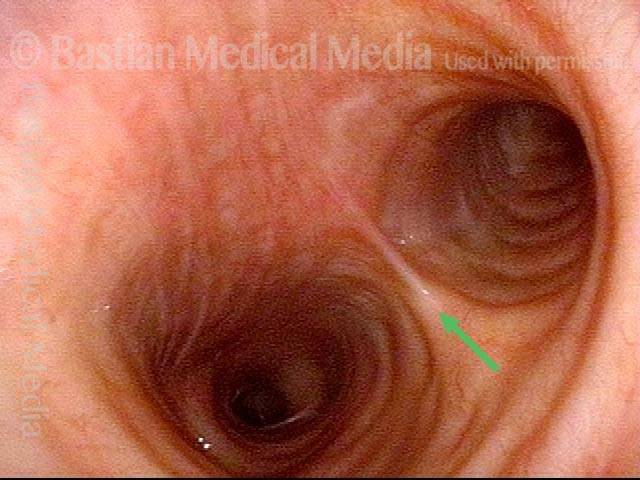
View of the distal trachea in a patient with nonorganic “asthma.” An arrow marks the location of the carina; note how, at this moment, the mainstem bronchi to each side are widely opened.
Nonorganic breathing disorder, tracheal (2 of 2)
Wheezing. (Arrow still at the carina.) One can see that the cause of the wheezing is functional manipulation of the distal trachea, in this case mainly the left mainstem bronchus (right of image); hence, the wheezing is louder over the lung on that side than the other side. Also, unlike with true asthma, the wheezing is much louder over the manubrium than either of the peripheral lung fields.
Example 3
Nonorganic breathing disorder, tracheal (1 of 2)
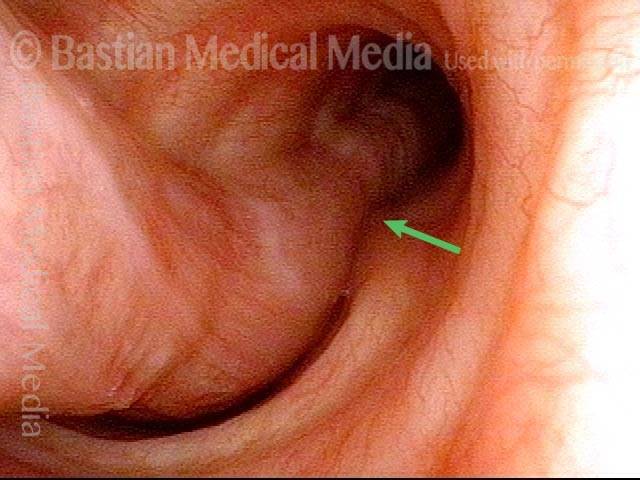
View of the distal trachea at the carina (where the windpipe divides into the right and left mainstem bronchi). Orienting arrow at the base of the carina.
Nonorganic breathing disorder, tracheal (2 of 2)
With exhalation, the tracheoesophageal party wall bulges inward to largely obstruct the right mainstem bronchus. The result is convincing, but nonorganic, wheezing. This is suspected from the patient’s affect (e.g., surprising nonchalance and distractibility) and because the wheezes auscultate more loudly over the central chest than in the periphery. (In this slightly closer view, an arrow again indicates the base of the carina.)
“Functional” Mainstem Bronchial Wheezing Is Easier to Mistakenly Diagnose as Asthma than Tracheal Wheezing
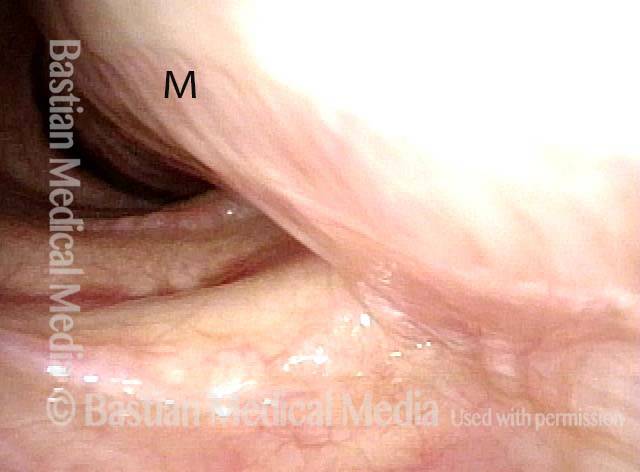
View of trachea during inspiration (1 of 6)
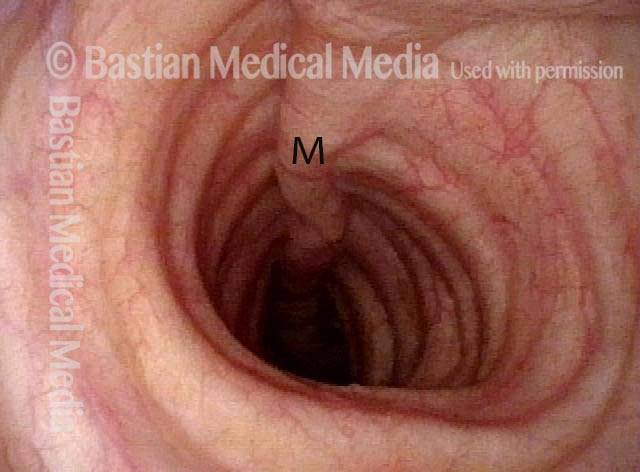
This man has expiratory wheezing but the question of vocal cord dysfunction (which usually causes inspiratory noise) has been raised. The actual problem is not laryngeal, but instead functional/ non-organic large airway wheezing. Here is a view of most of trachea during inspiration. “M” designates membranous portion in all photos of this series.
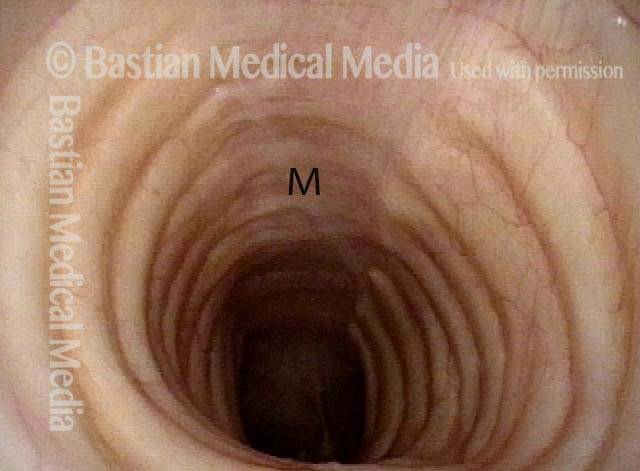
Exhaling forcibly (2 of 6)
When asked to exhale forcibly, marked wheezing is heard. The membranous trachea invaginates but does not appreciably narrow the lumen caliber. Wheezing is NOT from this level of the trachea.
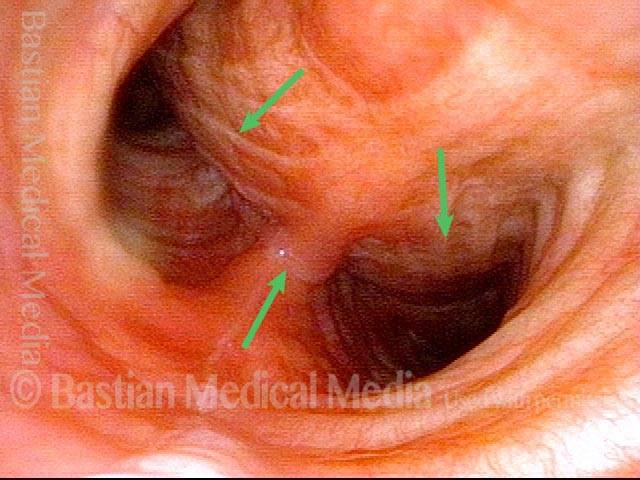
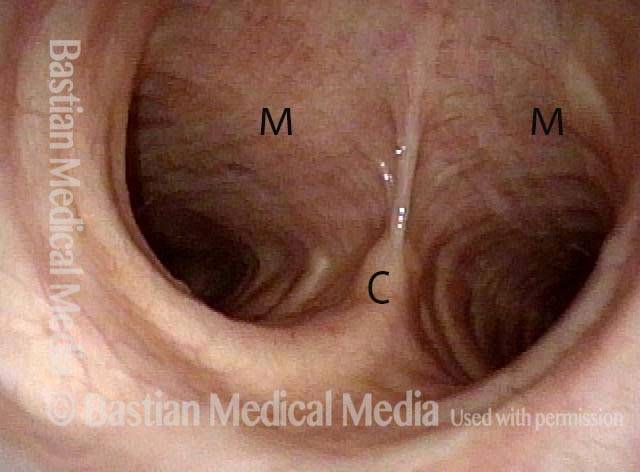
Carina (3 of 6)
Deeper in, with carina in clear view during inspiration (marked with “C” in this and subsequent photos).
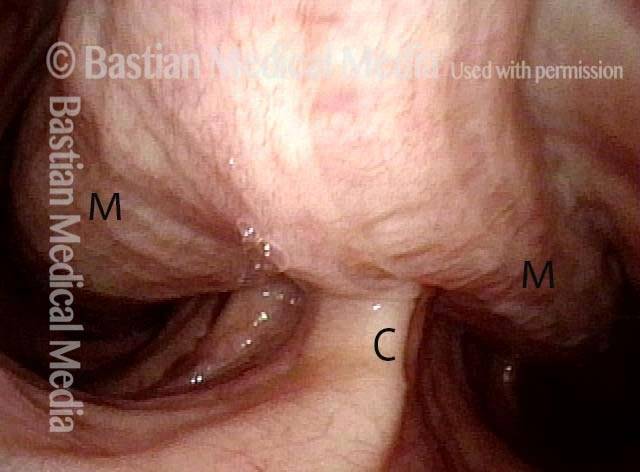
Trachea bulges inward (4 of 6)
With forced expiration, the membranous trachea bulges inward and mostly obscures the carina, but the degree of luminal narrowing is still not sufficient to create significant wheezing at this level.
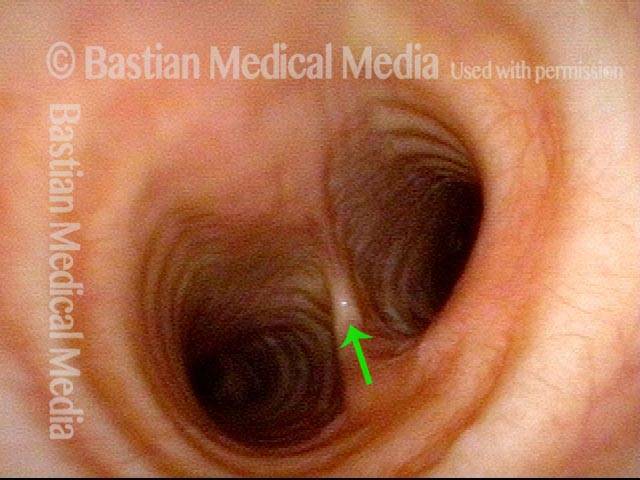
Right mainstem bronchus during inspiration (5 of 6)
Now viewing even farther down, into the right mainstem bronchus, with base of the carina still barely in view (again at “C”).
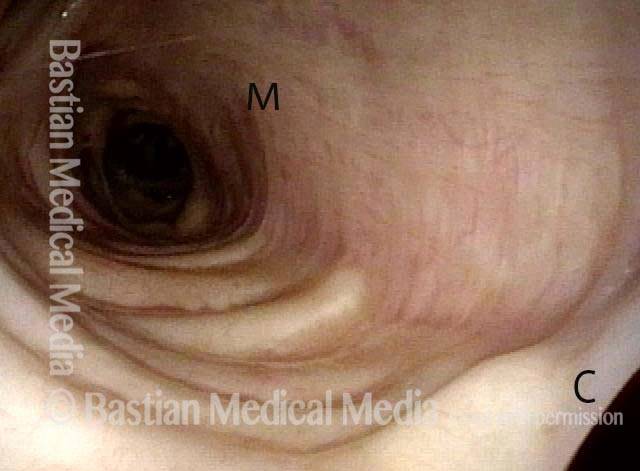
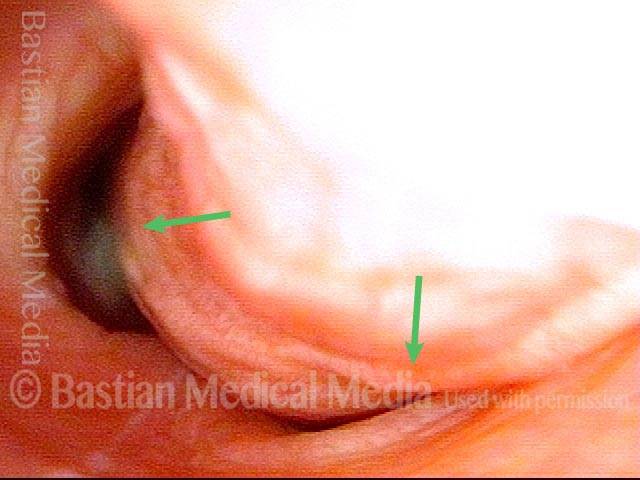
Wheezing origin (6 of 6)
The membranous right mainstem bronchus bulges inward and leaves only a small dark crescent of space for out-rushing air. THIS is where the wheezing is originating. Wheezing noises from distal trachea and mainstem bronchi will be transmitted to the lungfields better and more closely mimic asthma, as compared with wheezing that originates in the trachea; which is much louder on auscultation at the sternal notch than in the peripheral lungfields.