Granulation as a Cause of Tracheotomy Dependence
This unfortunate man suffered a severe auto accident, resulting in multi-system injuries, including a cervical spinal cord injury, closed head injury, and multiple fractures. He required an extended ICU stay on a ventilator via an endotracheal tube for his many surgical repairs, and while comatose.
After weeks of stabilization and recovery, he was transferred to a rehabilitation facility. Some weeks later, he developed progressive stridor, requiring an urgent tracheotomy. Though the trach-tube was subsequently removed, soon, increasing breathing difficulties necessitated its reinsertion. Due to his paralysis (para/quadriplegia), he continued to live in a longterm nursing facility. The tracheotomy remained for suctioning access and easier breathing.
He was able to occasionally plug the tube, using his voice by occluding the trach with a finger. However, 2 ½ years later, he completely lost the ability to speak and could no longer breathe through his nose or mouth when the trach tube was plugged.
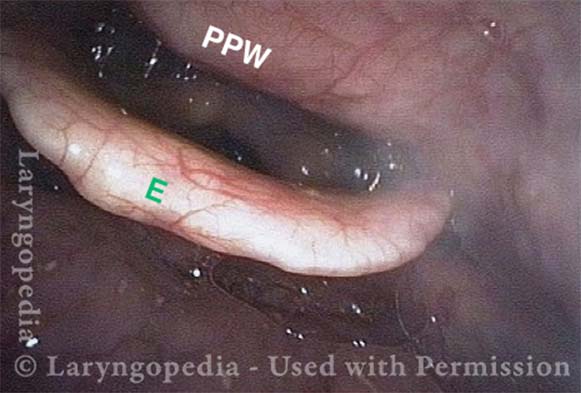
Narrow Hypopharynx (1 of 4)
Endotracheal tube injury (2 of 4)

Severe Granulation (3 of 4)
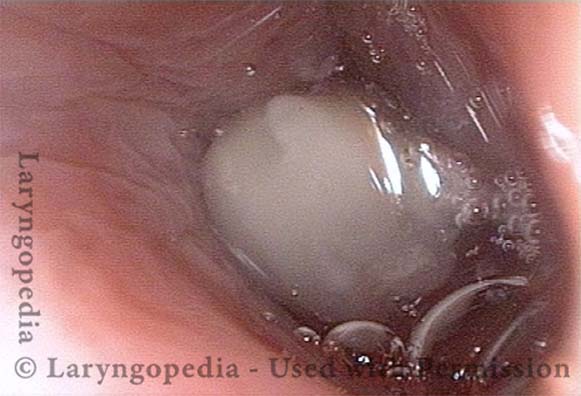
Avascular granuloma (4 of 4)