Cricopharyngeal Dysfunction, Before & After Myotomy
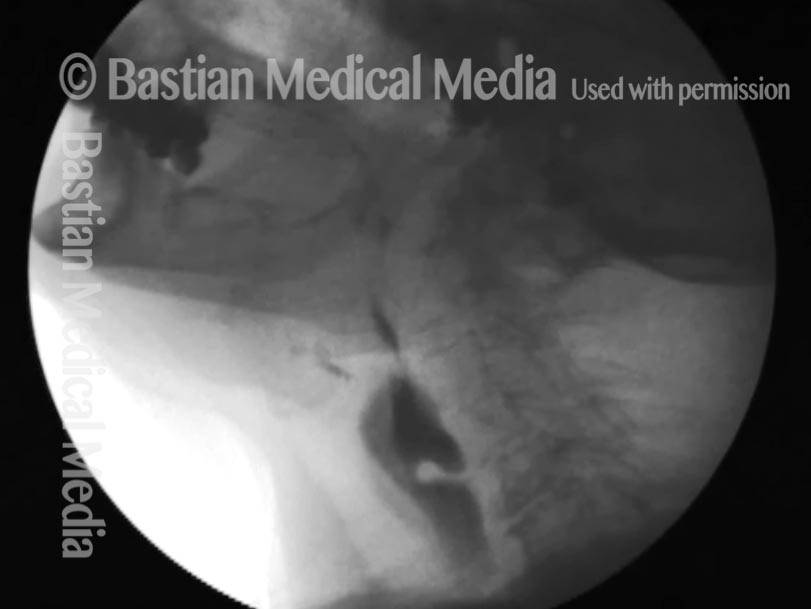
Cricopharyngeal dysfunction: before myotomy (1 of 2)
Lateral x-ray of the neck while swallowing barium (seen as a dark column). The non-relaxing cricopharyngeus muscle (light-grey bulge outlined by a dotted line) is causing narrowing of the upper esophageal passageway, as highlighted by the narrowed stream of dark barium at that point (arrow). Liquids and very soft foods can squeak through this narrow opening, but solid foods tend to get stuck.

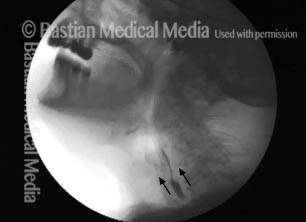
Cricopharyngeal dysfunction: after myotomy, resolved (2 of 2)
After myotomy. The surgically divided muscle can no longer narrow the upper esophageal passageway, as seen by the widened stream of dark barium at the level of the muscle (arrows).

Example 2
Cricopharyngeal dysfunction: before myotomy (1 of 2)
Lateral x-ray of the neck while swallowing barium (the dark material seen here in the throat). The non-relaxing cricopharyngeus muscle (light-grey bulge outlined by a dotted line) is causing narrowing of the upper esophageal passageway, as highlighted by the narrowed stream of dark barium at that point (arrow). Liquids and very soft foods can squeak through this narrow opening, but solid foods tend to get stuck.

Cricopharyngeal dysfunction: after myotomy, resolved (1 of 2)
After myotomy. The surgically divided muscle can no longer narrow the upper esophageal passageway, as seen by the widened stream of dark barium at the level of the muscle (arrows).

R-CPD, Aerophagia and Burping
This lateral x-ray of the neck is part of a swallow study, and illustrates how air can accumulate and need to be burped up. The focus of this photo essay is the esophagus, or “foodway,” that connects the lower part of the throat to the stomach. The esophagus is a muscular tube that remains mostly collapsed—closed—except when food, liquid, or saliva traverses it. Read more about esophageal findings of R-CPD.
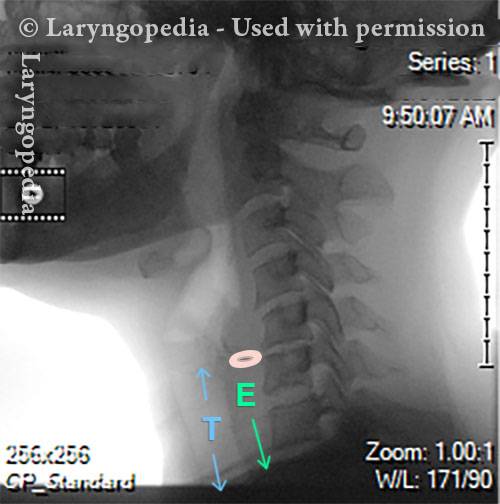
X-Ray of Larynx (1 of 6)
This is a view during quiet breathing (no swallowing in progress.) E overlies the esophagus, which is collapsed / closed in this pre-swallow view. T identifies the trachea which always contains an “air column.” It is “guarded” by the vocal cords which close tightly during each swallow. In this view, the vocal cords and entrance to the trachea are open. The upper esophageal sphincter which is virtually identical to the cricopharyngeus muscle, is in its contracted “rest” (non-swallowing) state, approximately at the circle.
Barium swallow (2 of 6)
In this view, the individual is swallowing barium paste. Barium is used because it is inert (not absorbed by the GI tract), and radiopaque (so it is visible on an x-ray). This swallow of barium is beginning its descent like a long dark sausage, opening the otherwise collapsed esophagus to permit passage. The cricopharyngeus muscle has opened approximately at the circle. One can tell that this is not the first swallow, because a thin dark line is visible near the bottom of the xray (arrow) where barium has passed previously and left a trace inside the esophagus’ collapsed walls.

Collapsed esophagus (3 of 6)
Here the slender tail of a swallow of barium is disappearing into the mid-esophagus below. The esophageal walls have collapsed back together. The airway has reopened. There is a trace of barium in the vallecula or “little valley” between base of tongue and epiglottis.

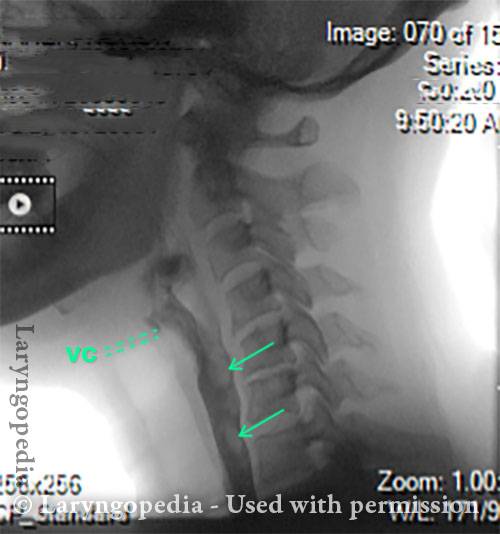
Air is swallowed (4 of 6)
Here, this person is swallowing thinner (less dense) barium material. The entrance to the larynx (and trachea) are being guarded by closed vocal cords (vc). Note that there is some air within the stream of barium at the arrows. If a little bit of air accompanies each swallow, and that air accumulates to a sufficient amount, it will need to be burped up.
UES refuses to open for a burp (5 of 6)
In this view, air that has been swallowed in “bits and pieces” (see prior image) has coalesced into an “air sausage” that wants to move upwards and be released as a “burp.’ If the cricopharyngeus muscle refuses to “let go,” then the air continues to build up, making the “air sausage” in the esophagus wider and longer like a progressively-inflated balloon. Some air will be kept in the stomach by the over-accumulated, trapped esophageal “air sausage,” eventually stretching the stomach too. And when sufficient air accumulates in the stomach, it begins to pass into the small intestines and then colon, eventually (finally…) emerging as flatulence.

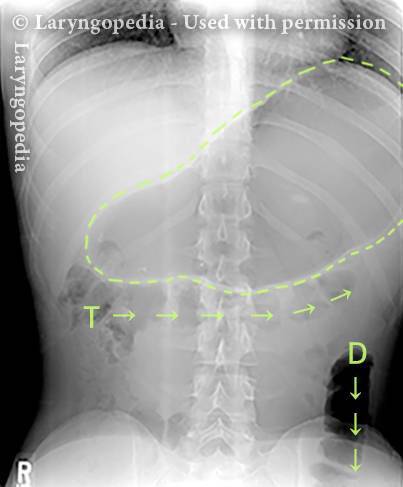
Abdominal Distention from R-CPD (6 of 6)
Here in an anterior view of the abdomen and chest, you see the result if that esophageal “sausage of air” cannot be released via burping and if the person continues to swallow air reflexively due to discomfort, pumping themselves ever more full of air. The stomach is dramatically dilated. And you can see a lot of air in the transverse (T) and descending colon (D), which must now be released as flatulence.
Post-swallow Hypopharyngeal Reflux (Zenker’s Diverticulum): VESS vs. VFSS
VESS (1 of 7)
In a patient with a known Zenker’s Diverticulum, who has just finished swallowing blue-stained applesauce during VESS.

Reflux (2 of 7)
Less than a second later, the applesauce and some saliva bubbles reflux upwards from the Zenker’s sac into the postarytenoid area.

Post-swallow (3 of 7)
Here, the patient has just swallowed a cheese cracker.
Reflux of cracker (4 of 7)
About a second and a half later, this material, mixed with saliva, returns from the sac.

VFSS (5 of 7)
Just after the patient has swallowed a bolus of barium.

X-Ray (6 of 7)
A second later, barium is “squishing” upwards from the sac.

Continued reflux (7 of 7)
Additional barium has come upwards into the postarytenoid area (compare with Photos 2 and 4).

Great View of Fresh Cricopharyngeus Myotomy Surgical Wound
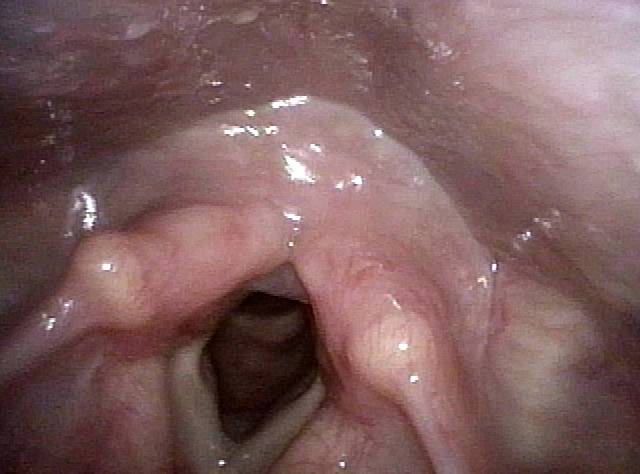
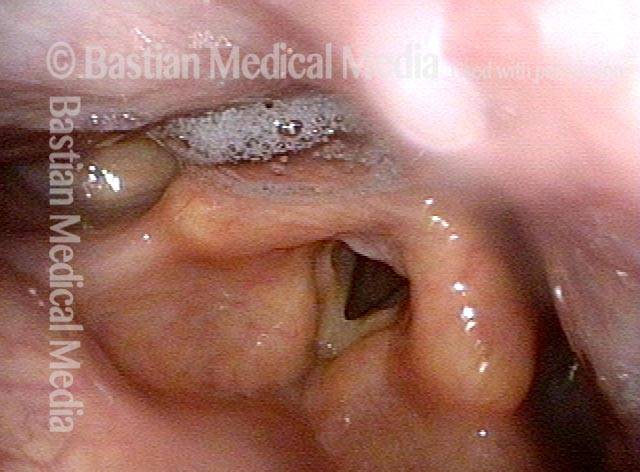
CPM dysfunction (1 of 4)
After administration of blue-stained applesauce during VESS, small and organized residue in the post-arytenoid area suggests possible cricopharyngeus muscle dysfunction. At this time, the patient noted only occasional pill lodgement.
VFSS six years later (2 of 4)
Six years later, the patient returned saying that swallowing had gradually become extremely difficult. Swallowing pills and eating food were nearly impossible. A VFSS shows narrowing of the barium stream at the arrow, due to a cricopharyngeus bar or “thumb” at *.

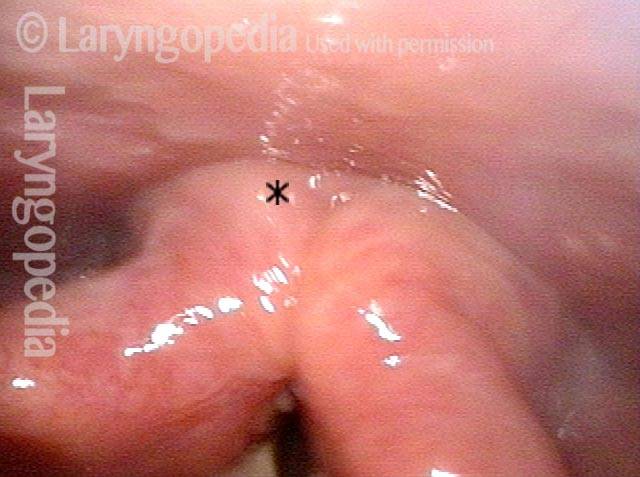
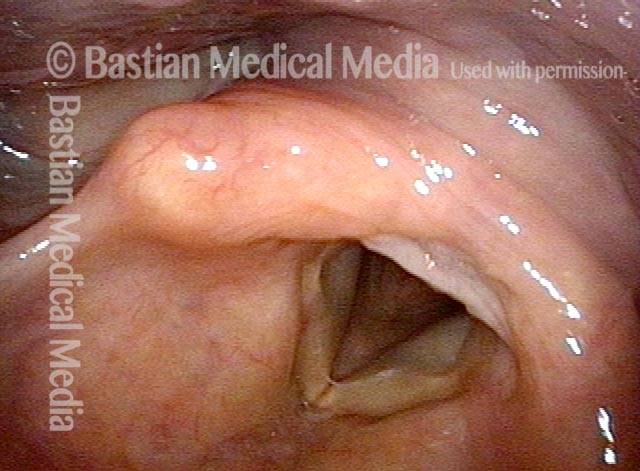
Five days post-op (3 of 4)
Five days after endoscopic laser cricopharyngeus myotomy, the patient says that while surgical pain is still significant, she can already swallow pills and solid food easily, a dramatic change from 5 days earlier. The area of surgery is not seen in this resting view. The * is for orientation with the following photo.
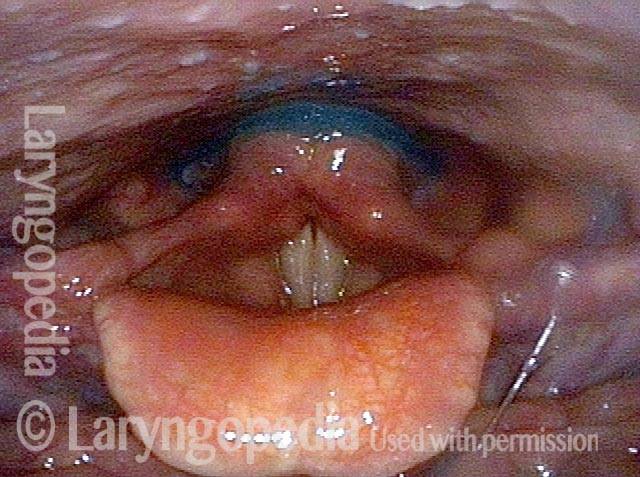
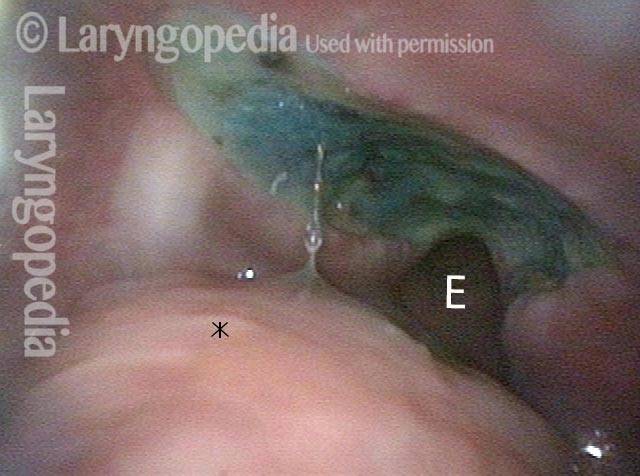
Cervical esopagus (4 of 4)
The patient is puffing her cheeks and this is enough to open the cervical esophagus (E). This allows visualization of the raw surface where the muscle was divided with the laser. It is stained by recently administered blue applesauce. The * is for orientation with the prior photo.
98 Year-old before and after Myotomy
Immediately after swallowing (1 of 10)
This 98 year-old woman experiences dysphagia that is most noticeable for solids. She is also aware of constant “phlegm” in her throat. In this photo, she has just completed a swallow of her own saliva. See what happens a moment later in the next photo.
Zenker’s (2 of 10)
A second later, saliva emerges from below, as her known Zenker’s diverticulum discharges some of its contents upwards into the hypopharynx rather than downwards into the esophagus.
Dysphagia (3 of 10)
During VESS, part 2, she has just completed a swallow of blue-stained applesauce without leaving any immediate post-swallow residue.
Residue from Zenker’s (4 of 10)
A second later, the applesauce and saliva retained in her Zenker’s diverticulum is pushed upwards from below.

X-ray showing Zenker’s (5 of 10)
An x-ray image showing the Zenker’s diverticulum immediately following her swallow.
Moments later (6 of 10)
A moment later, some swallowed barium has discharged upwards into the hypopharynx.
After myotomy (7 of 10)
A week after endoscopic cricopharyngeus myotomy. The patient says her swallowing has become normal. This view verifies her observation. Here, she has just completed a swallow and after waiting considerable time, no saliva reappears. Compare with photo 2.
No residue (8 of 10)
After not only blue-stained applesauce, but also a cheese cracker, there is no return of material and only a fleck of cracker in the left pyriform sinus (arrow). Compare with photo 4.

Zenker’s gone (9 of 10)
After myotomy, note that the Zenker’s sac only puddles at its apex, because the rest of the sac has been marsupialized into the esophagus. Patients with this finding have no swallowing symptoms. Compare with photo 5.

No barium in hypopharynx (10 of 10)
While watching throughout the study, no barium ever emerges upwards into the hypopharynx, in constrast to pre-operatively. Compare with photo 6.