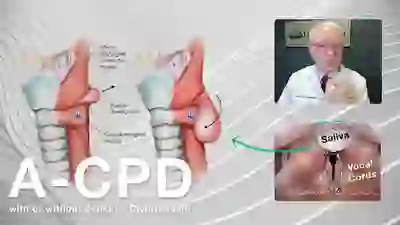
Early A-CPD
The cricopharyngeus muscle (CPM) and upper esophageal sphincter (UES) are virtually synonymous terms. That muscle/sphincter is located at the junction between the lower throat (pharynx) and upper esophagus.
When not in use it is (paradoxically) contracted. It only relaxes, momentarily, when one swallows saliva, liquid, food, pills, etc. (It must also relax momentarily to permit burping or vomiting. Those who swallow normally but can’t burp have retrograde cricopharyngeus dysfunction [R-CPD], described elsewhere.)
What Are the Symptoms of A-CPD?
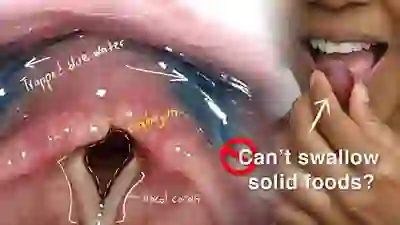
In some people, the muscle begins failing to relax completely when swallowing. Across many years, the degree of relaxation for the moment of swallowing progressively decreases. At first, one may experience lodgment at the level of mid-to-lower neck of pills, steak, etc. After a few years, the person begins to eat only soft, well-chewed food, avoiding things like meat and bread. As time passes, even formerly easy foods become difficult.
If the problem is ignored long enough, the person becomes limited to (in the words of one elderly patient who had been symptomatic for 20 years), “cream of wheat and canned peaches.”
Fortunately, the problem can be resolved by cricopharyngeus myotomy. That is mostly done endoscopically (through the mouth) using a laser. This procedure has been described elsewhere.
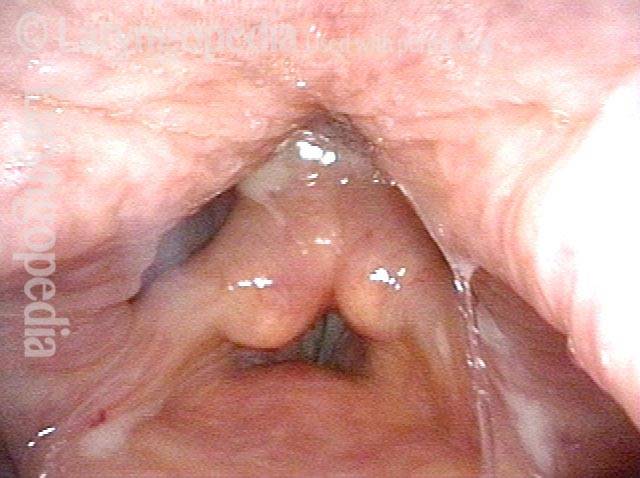
CP Thumb (1 of 4)

Bottleneck in X-ray (2 of 4)

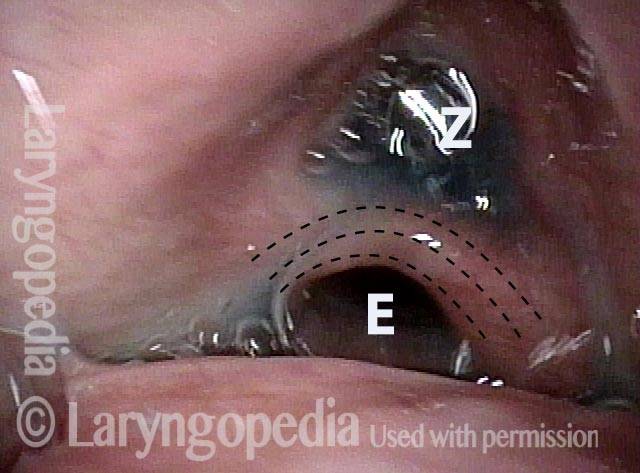
Incipient Zenker’s Diverticulum (3 of 4)

Swallow-To-Swallow variability (4 of 4)

A-CPD, before, during, and after Myotomy.
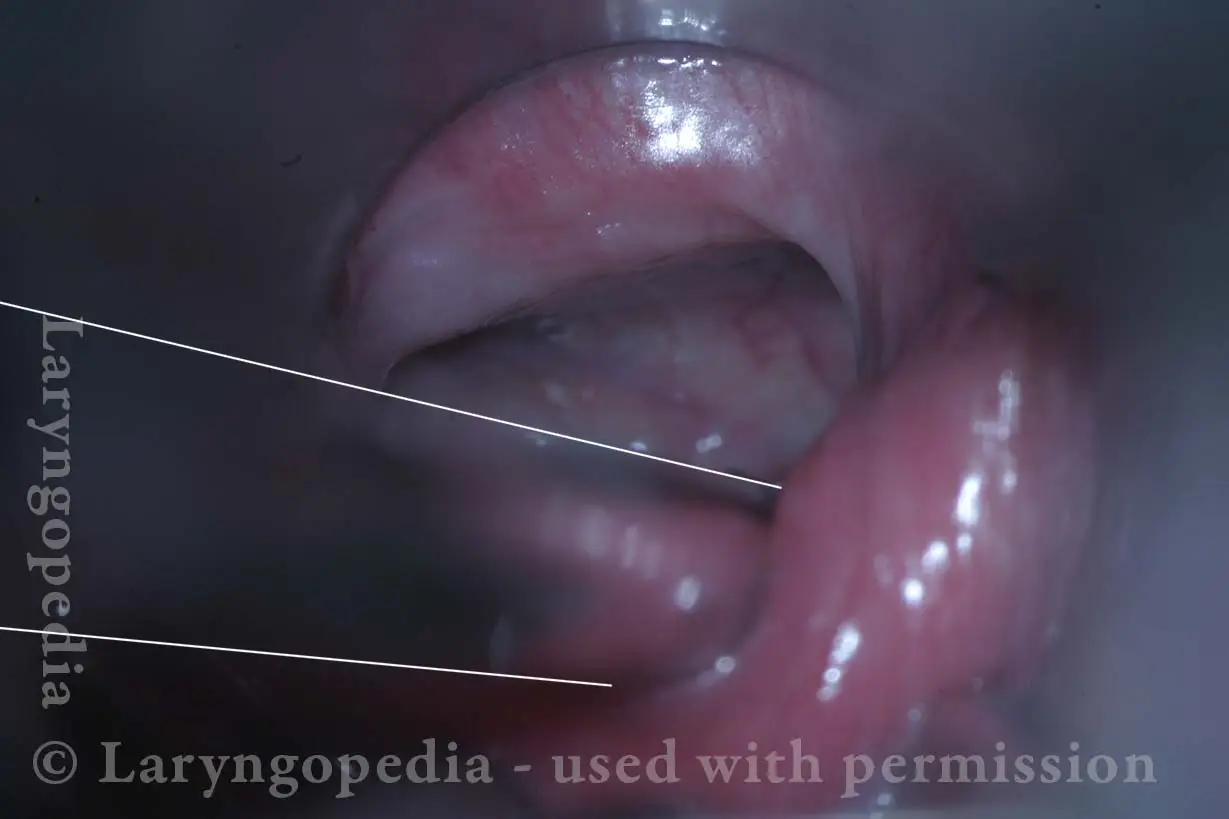
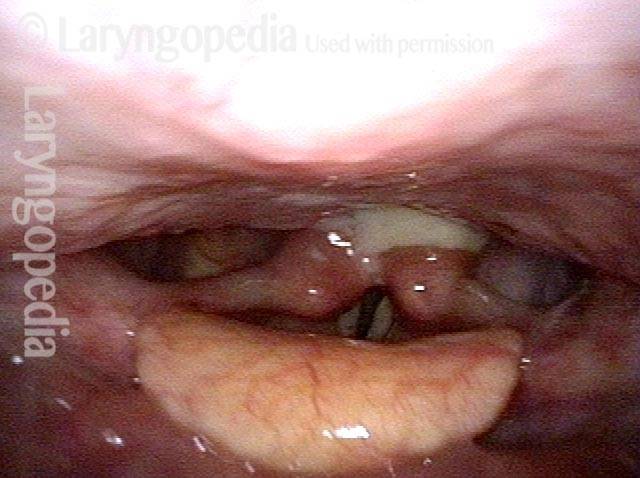
Non-relaxing cricopharyngeus muscle (1 of 4)

Opening the esophageal orifice (2 of 4)
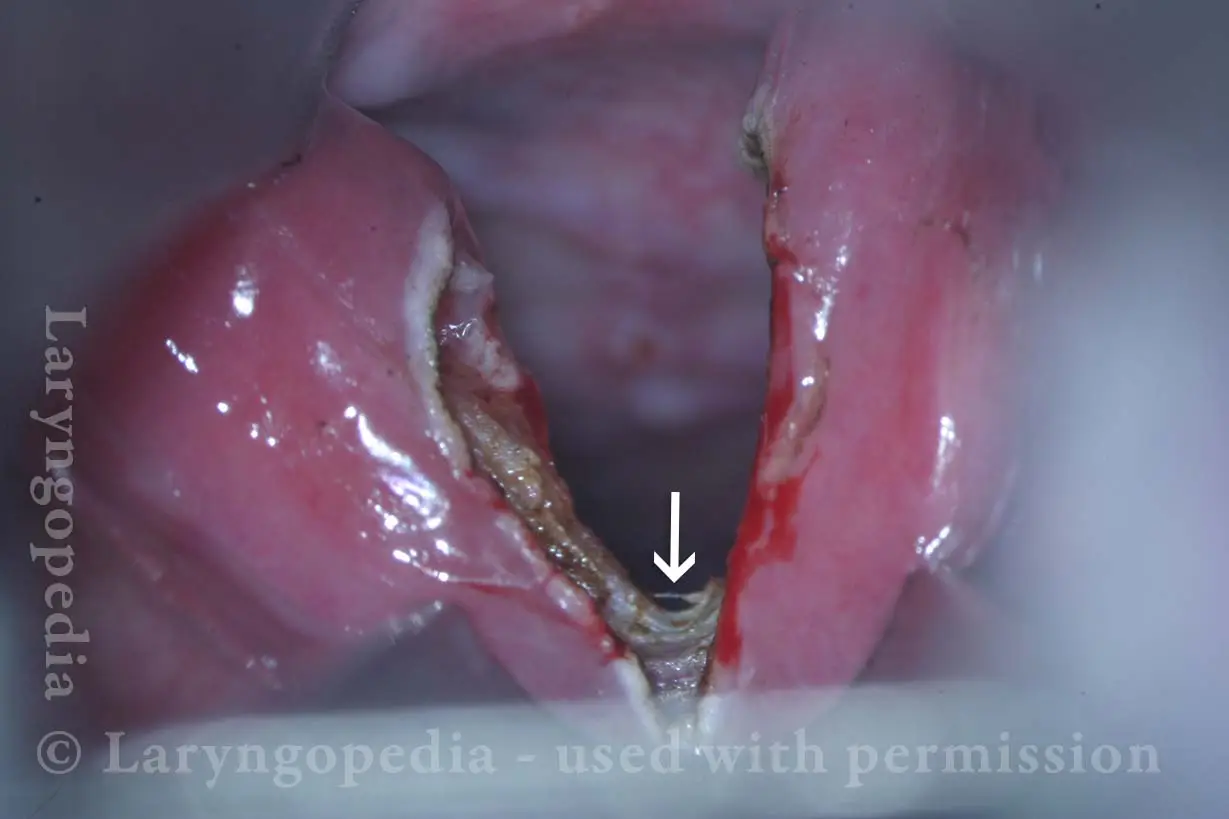
Laser cricopharyngeus myotomy (3 of 4)

Cricopharyngeus myotomy nearly complete (4 of 4)
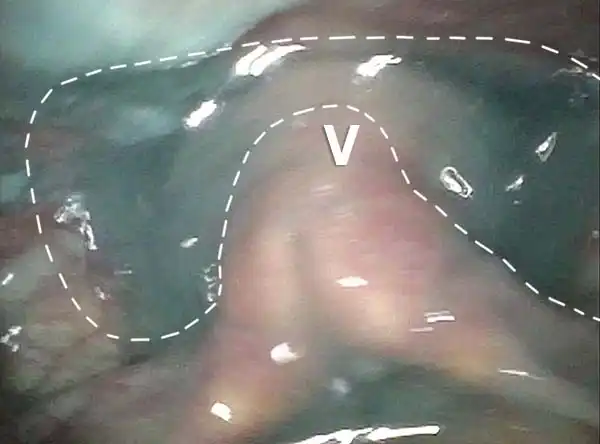
The Cricopharyngeus Muscle Seen During Swallowing
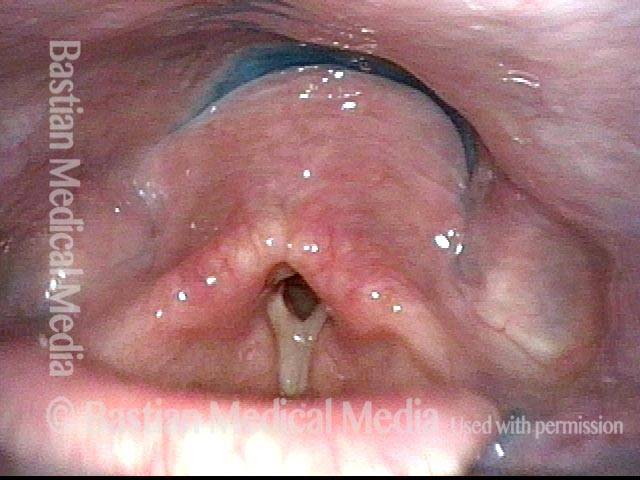
This person struggles to swallow due to a combination of prior tongue cancer surgery decades ago, and longterm radiation effects. Solid foods are the most problematic, and so this sequence shows an attempt to swallow water stained with blue food coloring.
Swallowing crescent (1 of 5)
Swallowing water (2 of 5)
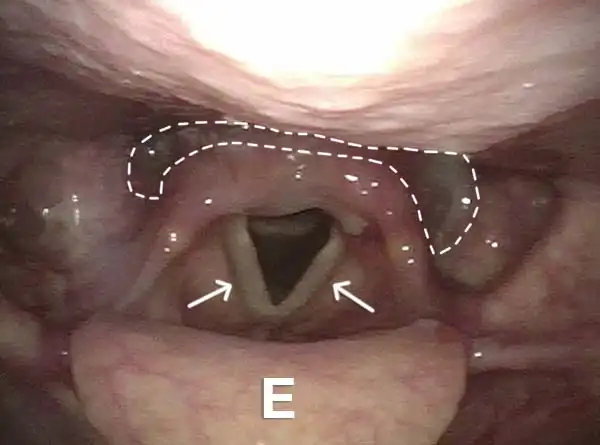
Cricopharyngeus muscle (3 of 5)
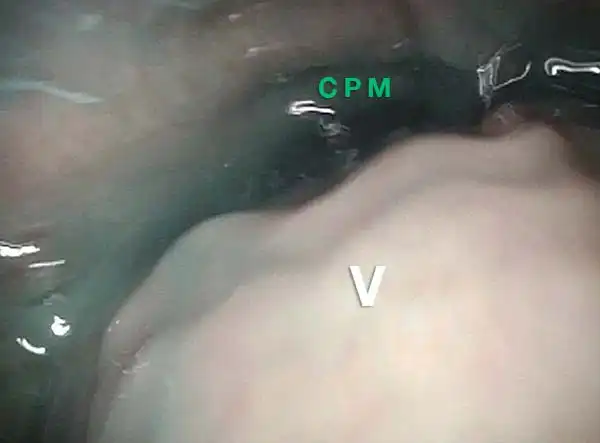
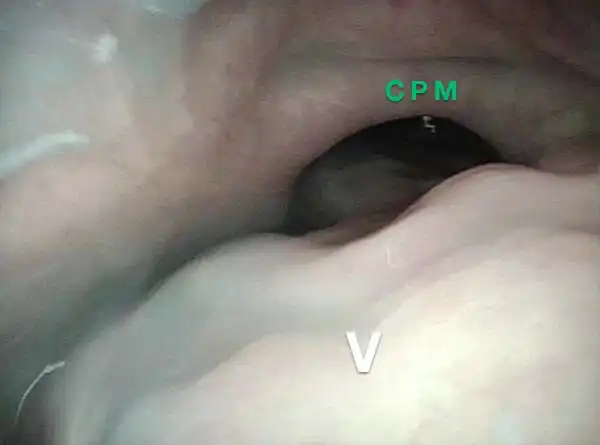
Relaxed CPM (4 of 5)

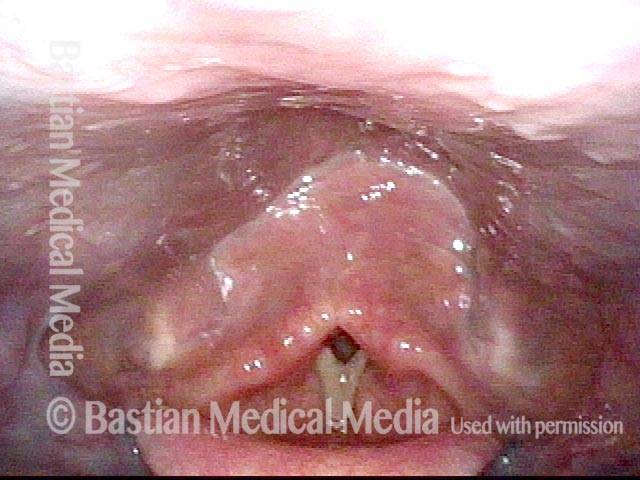
Partially open esophagus due to A-CPD (5 of 5)
A-CPD, Before and After Myotomy
Cricopharyngeal dysfunction: before myotomy (1 of 2)

Cricopharyngeal dysfunction: after myotomy, resolved (2 of 2)

Example 2
Cricopharyngeal dysfunction: before myotomy (1 of 2)

Cricopharyngeal dysfunction: after myotomy, resolved (1 of 2)

Very High-pitched Voice Elicits the Same Pharynx Contraction as Swallowing
Secretions (1 of 4)
Contracted pharynx (2 of 4)
Cracker residue (3 of 4)
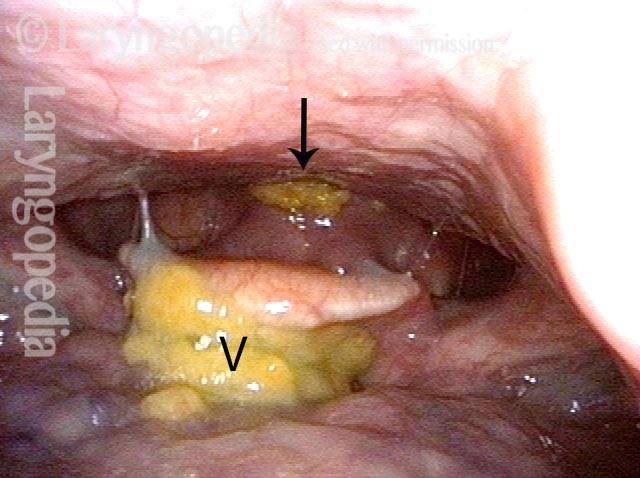
Pharyngeal walls (4 of 4)
Reflux Into Hypopharynx, Characteristic of Antegrade Cricopharyngeal Dysfunction
Reflux into hypopharynx (1 of 3)
Water flows into the swallowing crescent (2 of 3)
Larynx opens up (3 of 3)

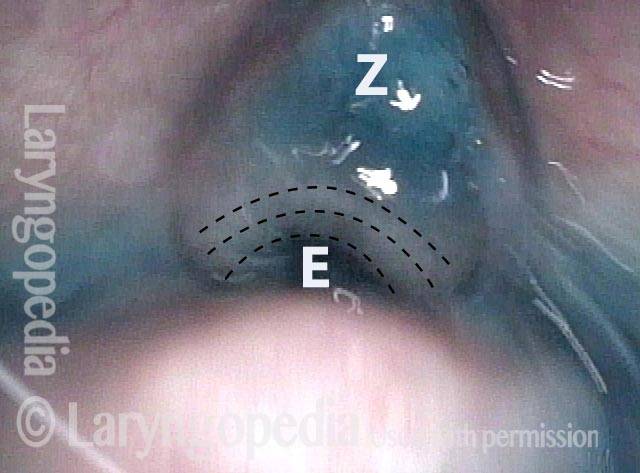
Cricopharyngeus Non-Relaxation and Zenker’s Sac Seen During VESS
Immediately after swallow (1 of 4)

One second later (2 of 4

Un-relaxed cricopharyngeus muscle (3 of 4)
More water (4 of 4)