An Instruction Manual for Botulinum Toxin Injection for Spasmodic Dysphonia
Robert W. Bastian, M.D. — Published: January 14, 2025
ADDUCTORY Spasmodic Dysphonia (AD-SD)
AD-SD is a variant of spasmodic dysphonia in which the spasms push the vocal cords together, choking off or straining the voice.
Which Needle do You Use?
All but the rare patient can be successfully injected using the usual 37mm 25 gauge Teflon-coated needle.
Do you do Unilateral or Bilateral Injections?
I always do bilateral injections. The only unilateral injections are for those whom I “inherit” from elsewhere, where unilateral injections had been done for years. These patients sometimes insist that we continue this strategy, at least for their first shot with me.
What Is Your Starting Dose?
First of all, when we talk about dose with patients, we always speak of the total dose, and patients know it is half of that amount on each side.
For example, a dose of 1 unit means 0.5U per side.
The population dose ranges between 0.25U and 8U. That is 32x difference! The majority fall between 0.7U and 2U. Thus, my first dose is 0.7 U (0.35 U per side), and is always described as a “test dose.”
Dose requirement does not correlate with age, sex, height, weight, etc. That is, you may have a 90-lb 80 year-old woman who needs 2 units and a 240-lb 30-year-old man who needs 0.5 U!
So new patients are advised that if they happen to be unusually sensitive to the effects of botox, it is possible that this test dose is too strong, in which case we would lower the dose next time. Or, if spasms are only muted and duration of benefit is short, the next dose may be increased.
Usually by injection #2 or #3, we arrive at an optimal dose to use for this patient.
How do You get the Patient Ready for the Botox Injection? What kind of Anesthesia do You Use?
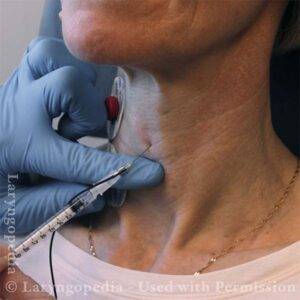
After cleansing the skin with an alcohol swab, I use a 5/8-inch 25 gauge needle, to inject 2% lidocaine into the skin over the cricothyroid membrane and then pass into straight posteriorly into the subglottis to deliver about 1.25 cc into the lumen. This makes the patient cough for a few seconds. The result is topical anesthesia of the mucosa within the subglottis and very high trachea. I leave the room and wait 2 to 5 minutes for that topical anesthesia to settle in.
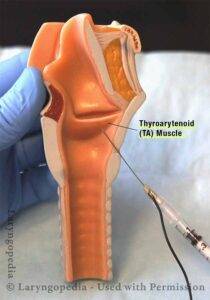
How do you Inject the Thyroarytenoid Muscles?
Having waited for topical anesthesia to begin, I return to the room and attach two gelpads (like EKG pads) to the lateral neck. These serve as the ground and reference electrodes.
The pads are connected to the miniature EMG machine.
The 27-gauge Teflon-coated EMG needle is also plugged into the EMG device.
Right VC injection
The skin is cleansed again with an alcohol swab.
The needle pierces the cricothyroid membrane and travels directly posteriorly until entering the lumen of the airway below the vocal cords.
After inside the lumen about 2mm, the needle is pointed laterally and superiorly into the undersurface of the vocal cord.
Once the crackling signal is heard, botox is injected while moving the needle slightly to distribute throughout the thyroarytenoid muscle.
I inject the right cord first and the left second, because the pinch on the left is often a bit greater than on the right, and referred sensations to the ear, down to the shoulder, etc.
Are There Other Tips and Pointers?
It is important to identify patients whose midline is shifted to the left or right.
Left VC injectionThe angle of injection varies according to laryngeal size and especially “height” of the cricothyroid membrane.
Paradoxically, sometimes men have a narrower cricothyroid membrane than women.
As always, if one finds a particular technique / angle works well, I write it on the working chart so that I don’t have to “reinvent the wheel” each time.
ABDUCTORY Spasmodic Dysphonia (AB-SD)
AB-SD is a variant of spasmodic dysphonia in which the spasms pull the vocal cords apart, causing the voice to drop out or sound weak and breathy.
Which Needle do You Use?
Most patients can be successfully injected using the usual 37mm 25 gauge Teflon-coated needle, but a few patients may need the 50mm length.
Some People Seem Afraid to do Bilateral Injections for Fear of Causing Noisy Breathing. What do You do?
I always do bilateral injections. This not infrequently causes some inspiratory noise. One patient told me he arrives first early in the morning and gets the lap pool to himself for a week after each injection, because others walk in and then leave when they hear his noisy breathing.
A few have, in good humor, said things like “My spouse has to do the vacuuming for a week or two after each injection.”
I only had one patient ever complain significantly when she got bronchitis right after a shot and each post-cough inspiration was very loud. And just for your information, I teach everyone with AB injections the technique of straw breathing, just in case…
What Is Your Starting Dose?
Typically 1 u unit per side for total dose of 2 units. Depending on response, I may reduce if noisy breathing in the first week or two is troublesome. Or I may increase the dose if there is no noisy breathing, or if the voice benefit is inadequate. I would say the eventual dose is usually between 2 and 3.5 units, total (split equally between the two sides).
How do You get the Patient Ready for the Botox Injection? What Kind of Anesthesia do You use?
After cleansing the skin with an alcohol swab, I use a 5/8-inch 25 gauge needle, to inject 2% lidocaine into the skin over the cricothyroid membrane and then pass into straight posteriorly into the subglottis to deliver about 1.25 cc into the lumen. This makes the patient cough vigorously for 10 or 20 seconds. The result is topical anesthesia of the mucosa within the subglottis and very high trachea. I leave the room and wait 2 to 5 minutes for topical anesthesia to settle in.
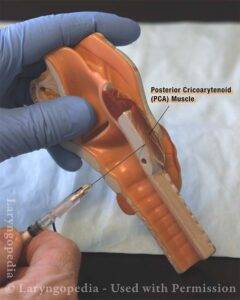
How do you Inject the Posterior Cricoarytenoid Muscle?
Having waited for topical anesthesia to begin, I return to the room and attach two gelpads (like EKG pads) to the lateral neck. These are ground and reference electrodes.
The pads are connected to the miniature EMG machine.
The 27-gauge Teflon-coated EMG needle is also plugged into the EMG device.
The skin is cleansed again with an alcohol swab.
The needle pierces the cricothyroid membrane and travels directly posteriorly until entering the lumen of the airway below the vocal cords.
The angle of the needle is commonly approximately 5 degrees down and 25 degrees laterally.
After the first or second injection of a patient, a different pair of angles may work better. For example, a particular patient might need an angle of 0 degrees horizontally and 35 degrees laterally.
Once you feel the needle go through the posterior cortex of cricoid you start having them sniff. If you get a signal, you begin to inject. Sometimes more than one pass of the needle is necessary to find a good signal.
Are There other Tips and Pointers?
It is important to identify patients whose midline is shifted to the left or right.
As many as one of every four or five patients gets a cartilage plug, making it impossible to inject the botox. In that case, you may have to change needles. But don’t give up too quickly. If you push the hub and needle tightly together and then exert sustained pressure on the plunger most times you can get the Botox in though very slowly.
If a patient has a barrel chest, the larynx and trachea will tend to be tilted toward you from high to low and the needle may be better angled superiorly by 5 degrees or so.
If a female patient has a very large cricothyroid space, I insert the needle low, just above the cricoid ring, to remain consistent each time.
As always, if one finds a particular technique that works well, I write it on the working chart so that I don’t have to “reinvent the wheel” each time.
 Which Needle do You Use?
Which Needle do You Use?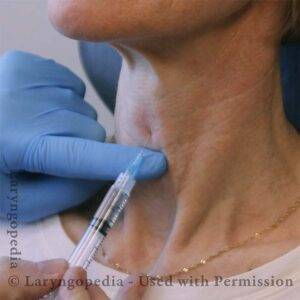 How do You get the Patient Ready for the Botox Injection? What kind of Anesthesia do You Use?
How do You get the Patient Ready for the Botox Injection? What kind of Anesthesia do You Use?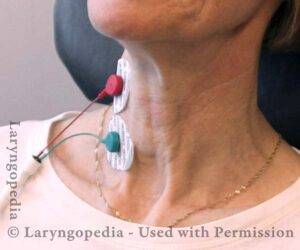 How do you Inject the Thyroarytenoid Muscles?
How do you Inject the Thyroarytenoid Muscles?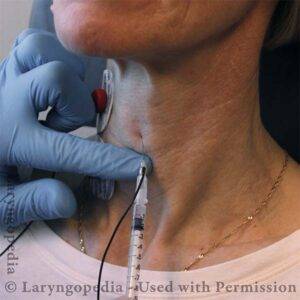
 Which Needle do You Use?
Which Needle do You Use?