
TA-only Paresis after Botox Injection for Spasmodic Dysphonia
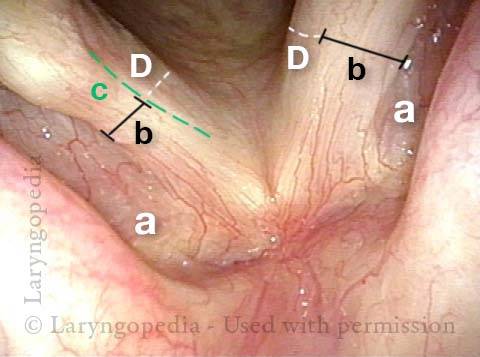
This man with adductory spasmodic dysphonia (AD-SD), has had consistent results during 15 years of botulinum toxin injections, administered several times per year. After his most recent (routine, and unremarkable) injection with his longstanding dose, his initial weakness was exaggerated and is only beginning to subside after six weeks. This dramatic “outlier” result that cannot be attributed to botox targeting. As seen in the photos below, the explanation is instead a right TA-only paresis.
The only reasonable interpretation is that the needle tip has “sheared” the branch of the recurrent laryngeal nerve supplying the thyroarytenoid muscle (leaving branches to the posterior cricoarytenoid and lateral cricoarytenoid muscles (PCA + LCA) undisturbed.
In a practice that supplies treatment to approximately 100 patients per month and ~1200 injections per year, this phenomenon occurs perhaps twice per year. The voice “always” recovers back to baseline SD symptomatology, but excessive breathiness starts to resolve only 6 weeks after the injection.
Right Thyroarytenoid Atrophy (1 of 3)
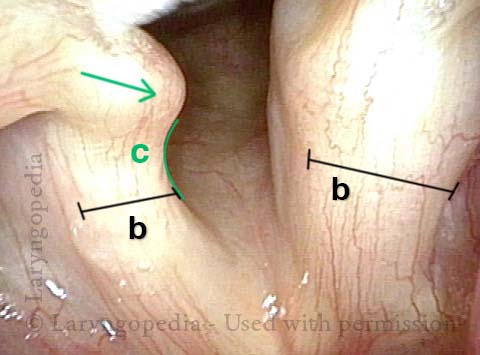
Sharp medial turning (2 of 3)
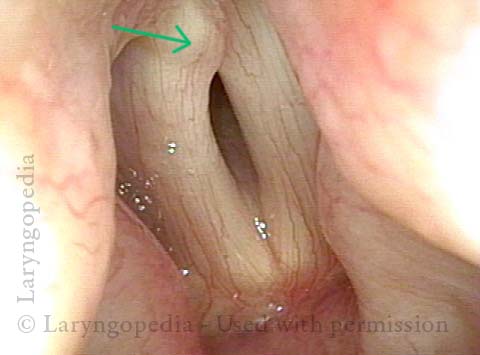
Right vocal process overlaps left vocal process (3 of 3)
Lifting the CPM for a R-CPD Injection
These are intra-operative photos of one of nearly 1500 persons treated for R-CPD as of September 2023. This sequence shows several things: The dilated, “always open” esophagus distal (below) the muscle; how to identify the cricopharyngeus muscle; and one way of injecting it.Above the CPM (1 of 5)

Ridge of the CPM (2 of 5)

Exposed CPM ( 3 of 5)

CPM Palpated ( 4 of 5)

Botox injection ( 5 of 5)

