Photo Examples
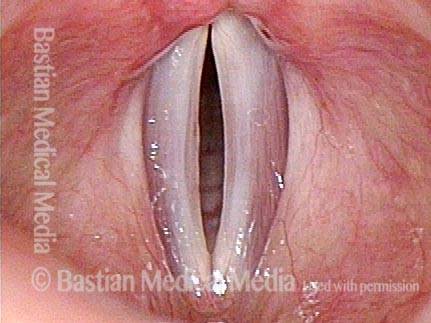
Vocal cord paralysis (1 of 7)
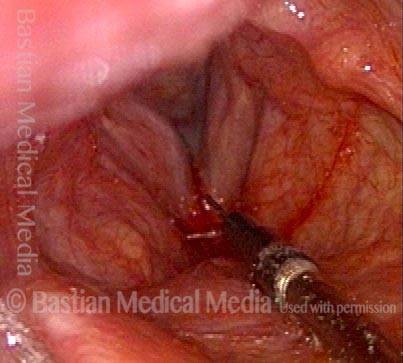
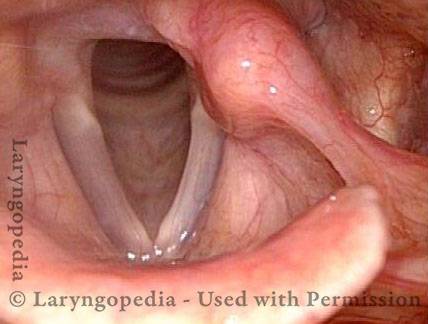
This person has a whispery voice due to right vocal cord paralysis. The right cord (left of photo) does not move from this lateralized position, whether she is breathing or attempting to make voice. The left cord (right of photo) is mobile and lateralized in this breathing position but can come to midline (see photo 3) when she makes voice. Here you see a needle poised to inject the slender, paralyzed lateralized cord with a filler material, in this case voice “gel.”

Voice gel injection (2 of 7)
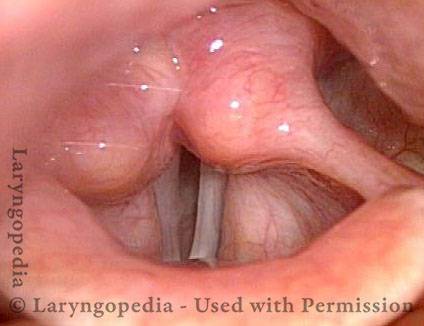
After the cord has been plumped up with injected voice gel. The injected cord is now within reach of the left cord during voicing, and it is also more firm.

Success (3 of 7)
The needle is withdrawn, and the patient is producing strong voice.
Plump right vocal cord (4 of 7)
A month later, as expected, the right cord (left of photo) remains plump.

Posterior gap (5 of 7)
Voice remains very good, due to ability to press the cords together. The upper surface of the injected cord is at a higher level than the left cord, due to the expected bulging “superiorly” and not only medially. Incidentally noted is the posterior gap due to LCA weakness. See the tell-tale lateral turning of the right vocal process at arrow.

PCA Weakness (6 of 7)
A little over a year after injection, the right cord appears to remain somewhat plump, as though some voice gel remains in a “pool” that protects from resorption. Though not well shown here, the right cord does not fully lateralize, suggesting residual PCA weakness.

LCA muscle recovered (7 of 7)
Voice remains very good, and the cords come into good approximation. The upper surface bulging is no longer seen. The most telling finding is that the LCA muscle appears to have recovered, and very likely, the TA muscle with it. Note that the vocal process has come back into line with the rest of the cord (arrow), and the posterior commissure gap seen in photo 5 is no longer seen. The patient’s excellent voice is explained by recovery of voicing muscles (TA and LCA) more than by residual voice gel.

Example 2
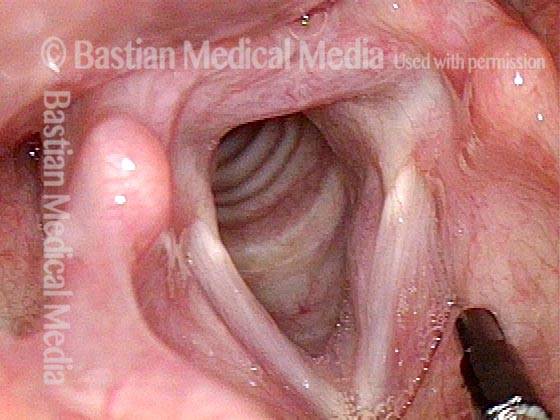
Paresis, TA + LCA (1 of 5)
Right vocal cord paresis (left of image). Note marked atrophy as compared with the left cord. Highly lateralized position denotes some persistent action of the right posterior cricoarytenoid muscle.

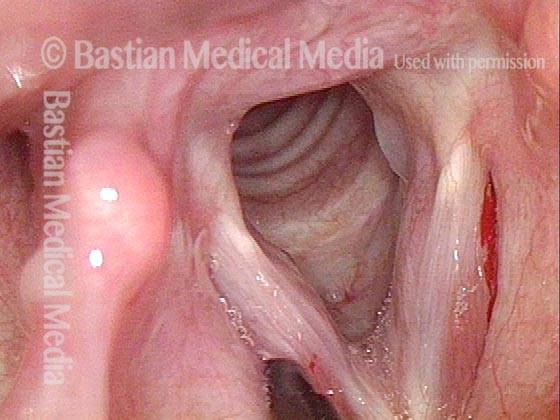
Paresis, TA + LCA (2 of 5)
Initiation of phonation. Note medical turning off left vocal process of arytenoid (right of image), and absent movement of the right vocal cord. Neither thyroarytenoid nor lateral cricoarytenoid muscles are innervated.

Voice gel injection (3 of 5)
Immediately following injection of right vocal cord (left of image) with voice gel, with patient in videoendoscopy room chair, under topical anesthesia. Note bulging of right vocal cord.
1 month after injection (4 of 5)
A month later, showing plumping up of the right vocal cord (left of image) with voice gel. Vocal cord continues to abduct fully, due to functioning posterior branch of recurrent nerve, which innervates the posterior cricoarytenoid muscle.

Phonation 1 month after injection (5 of 5)
Phonation. There is some movement to the midline due to the bilaterally innervated interarytenoid muscle. The lateral cricoarytenoid muscle is paralyzed, as seen in lateral turning of the vocal process. Voice is dramatically improved as compared with pre-injection. The voice gel will be expected to gradually absorb over three to nine months, during which time the anterior branch of the recurrent nerve may recover its function.
Injection Laryngoplasty with Temporary Gel
Laryngoplasty (1 of 4)
This person awakened with a weak, whispery voice after emergency abdominal surgery. Now 3+ months later, voice is returning by degrees but is still very weak. In this photo, the patient is breathing quietly. The weak left vocal cord is more bowed than the right.
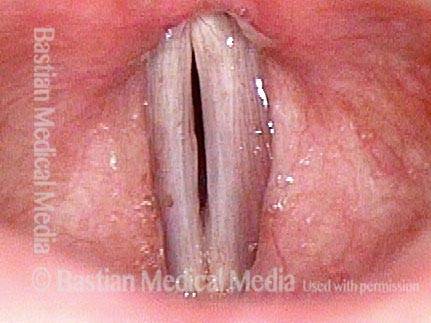
Reason for air-wasting (2 of 4)
When she tries to produce voice, the left vocal cord comes only part of the way to the midline, leaving a large gap, and explaining her whispery air-wasting voice quality.
Voice gel injected into vocal cord (3 of 4)
On the same day, due to pressing patient need, the left vocal cord was “plumped” with voice gel. That material typically provides temporary benefit of 6 to 12 weeks, gradually absorbing during that time.

Vocal cords close completely (4 of 4)
Voice is dramatically improved, now that her vocal cords can more fully close to reduce the air-wasting and transform the voice from whispery to strong. Compare with photo 2.

Congenital Glottic Sulcus & Bowing, before and after Injection
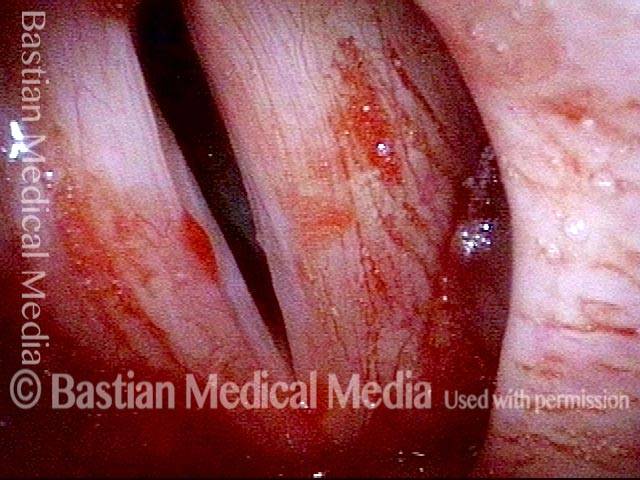
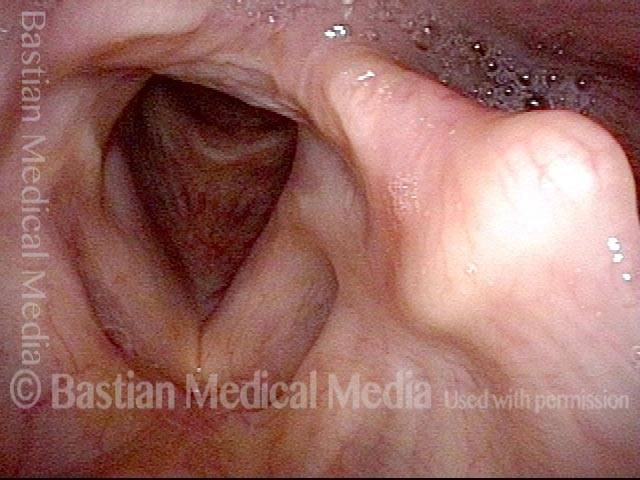
Glottic sulcus (1 of 10)
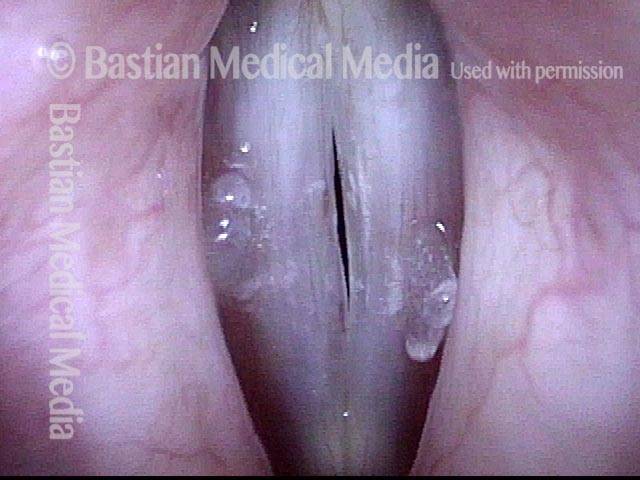
This young patient has a husky, air-wasting voice quality. View of the vocal cords, in breathing position. An abnormality can be seen, especially on the right cord (left of photo, at arrows).

Glottic sulcus (2 of 10)
Under strobe lighting, during phonation, open phase of vibration, at a normal speech frequency (pitch), showing an unusually large amplitude of vibration.

Glottic sulcus (3 of 10)
Closed phase of vibration, but not quite closing completely.
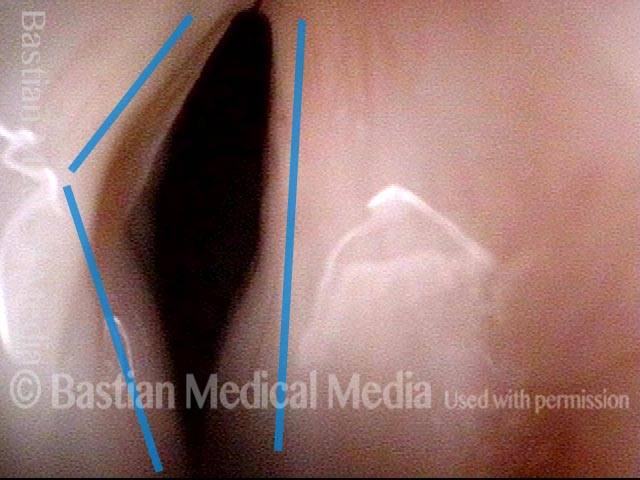
Glottic sulcus (4 of 10)
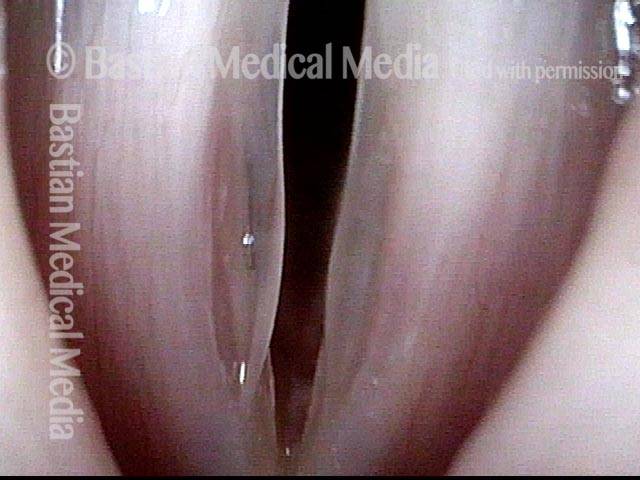
Closer view, during inspiratory phonation, reveals very clearly that this patient has sulci on both cords, with the open pocket especially visible on the right cord (left of photo).
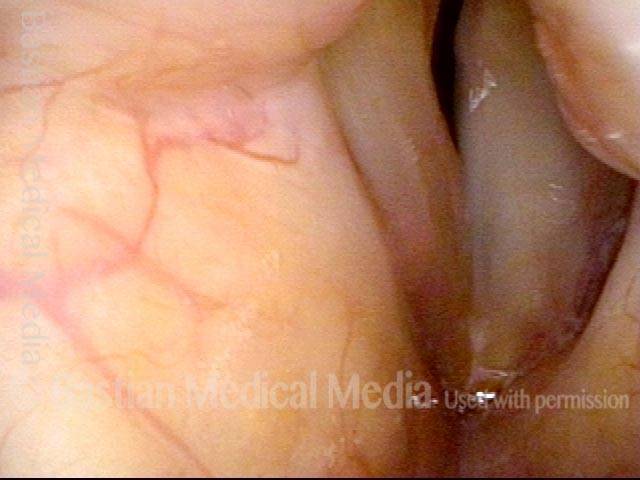
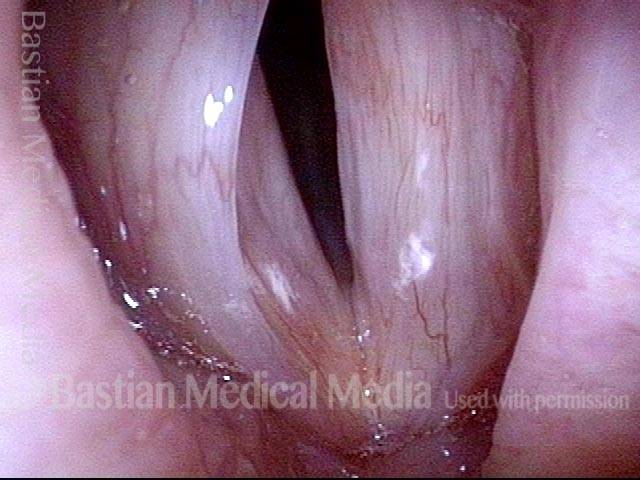
Sulcus with bowing, just prior to injection (5 of 10)
At the prephonatory instant, under standard light. In addition to a sulcus, this patient has congenital bowing.
Sulcus with bowing, just prior to injection (6 of 10)
Phonation, under standard light, at the pitch E-flat 4 (~311 Hz). Notice in particular the generous width of the zone of vibratory blurring, which correlates with the flaccid, large-amplitude vibration seen in photo 2’s strobe view.

Voice gel injection (7 of 10)
The left vocal cord (right of photo) is now being injected with voice gel. The injection is centered so that the undersurface, free margin, and ventricle all show evidence of bulging.
Voice gel injection (8 of 10)
The other vocal cord is now being injected.
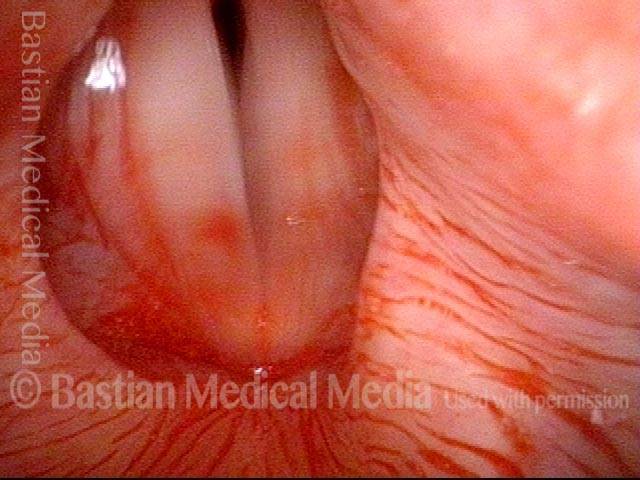
After the injection (9 of 10)
After voice gel injection is completed. At the prephonatory instant. Notice the reduced gap between the vocal cords (compare with photo 5).
After the injection (10 of 10)
During phonation, under standard light, again at E-flat 4 (~311 Hz). The width of vibratory blurring is reduced (compare with photo 6), consistent with reduced amplitude of vibration and reduced air-wasting.

Paresis, TA + LCA, before and after Injection of Voice Gel
Normally functioning PCA muscle (1 of 8)
Panorama shows normally functioning PCA muscle (supplied by posterior branch), indicated by abduction of both vocal cords to a fully lateralized position.
Paresis, TA + LCA (2 of 8)
As vocal cords just begin to move to adducted, phonatory position, note that the left cord (right of image) leads medially with the tip of the vocal process, while right vocal process remains turned laterally due to paralysis of the LCA muscle.

Paresis, TA + LCA (3 of 8)
Close-up of posterior commissure during phonation shows continuing lateral pointing of the right vocal process (left of image), again due to a paralyzed LCA muscle.
Lateral buckling (4 of 8)
Panoramic view during phonation shows lateral buckling due to flaccidity of paralyzed TA muscle, left vocal cord (right of image).
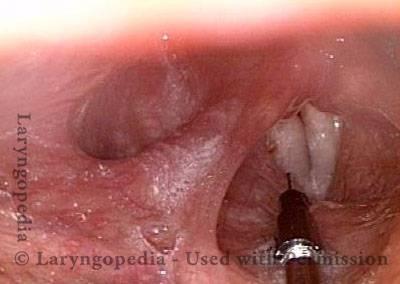
Voice gel injection (5 of 8)
A needle is being inserted into the TA muscle to inject voice gel as a temporary implant to plump up the cord so that the left cord (right of image) will be able to ” reach” it during phonation—and also, to counteract the flaccidity seen in photo 4 above.

After voice gel injection (6 of 8)
After plumping of the right vocal cord (left of image) with voice gel is completed.

After injection (7 of 8)
Phonation after voice gel injection, standard light. Note better closure of the cords.
Strobe light after injection (8 of 8)
Phonation under strobe light, open phase of vibration. This view shows that the voice gel has abolished the flaccidity seen above in photo 4.