Granuloma da Contatto
Un granuloma da contatto è una reazione o crescita benigna del tessuto, tipicamente sul terzo posteriore della corda vocale, che si verifica in risposta a una lesione. I granulomi da contatto sono noti anche come ulcere da contatto, granulomi da intubazione o “carne orgogliosa”. Questo tipo di tessuto cronicamente irritato può essere visto come un’esuberante risposta di guarigione che “non sapeva quando smettere”.
Fonti di Lesioni
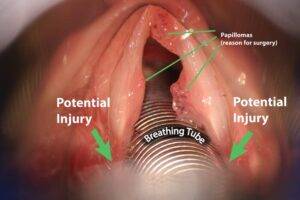
Un tipo di lesione che può portare a un granuloma da contatto è la lesione causata da un tubo endotracheale, poiché il tubo inserito preme e sfrega contro le estremità posteriori delle corde vocali. Un’altra potenziale fonte di lesioni è la tosse cronica e aggressiva o lo schiarimento della gola.
Ancora un’altra potenziale fonte è quella sottoposta a procedure chirurgiche come l’escissione laser di un cancro. Alcuni credono anche che l’irritazione da reflusso acido possa portare a un granuloma da contatto. In molti casi, non esiste una causa evidente per la lesione originale.
La Posizione Tipica
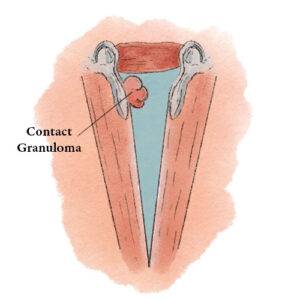
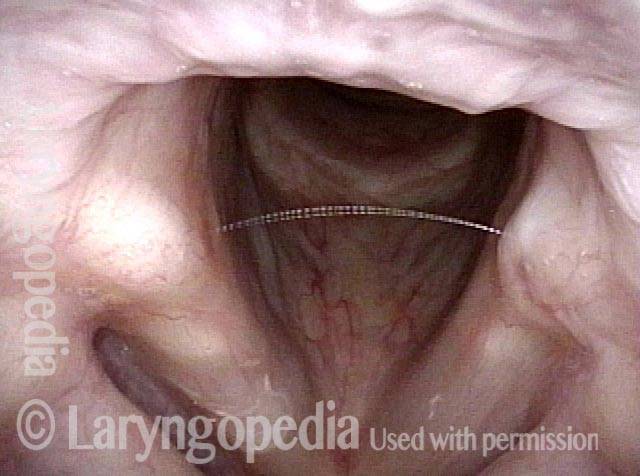
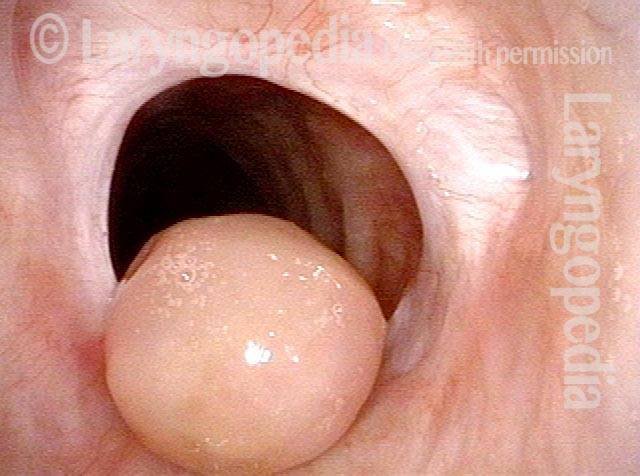
I granulomi da contatto si verificano tipicamente sul terzo posteriore della corda vocale, noto anche come glottide cartilaginea. A differenza degli altri due terzi della corda vocale, questo segmento è abitato da cartilagine (cioè cartilagine aritenoide) e tale cartilagine è ricoperta solo da uno strato relativamente sottile di pericondrio e da uno strato di mucosa.
Questa sottile interfaccia cartilaginea o pericondriale tende a irritarsi e quindi a rispondere con una guarigione esagerata che produce un granuloma da contatto. Pertanto, la maggior parte dei granulomi si verifica in questa posizione.
Sintomi
Alcuni individui con granulomi da contatto non presentano alcun sintomo e scoprono di avere un granuloma solo durante un esame per qualche altro motivo. Altri notano una sensazione di attaccamento o di puntura di spillo, oppure hanno un vago senso di disagio nella zona del collo che si irradia verso l’alto verso l’angolo della mascella.
Occasionalmente, una persona può sviluppare un “blocco” nella voce, tale che ci vuole un secondo per iniziare a parlare chiaramente. Molto occasionalmente, quando una parte del granuloma si stacca (vedi sotto), una persona può tossire sangue o un minuscolo pezzo di tessuto. In generale, i sintomi sono lievi.
Trattamento
Alcuni medici preferiscono trattare i granulomi da contatto eliminandoli. Tuttavia, la piccola lesione o ferita che ne risulta spesso produce un granuloma ricorrente.
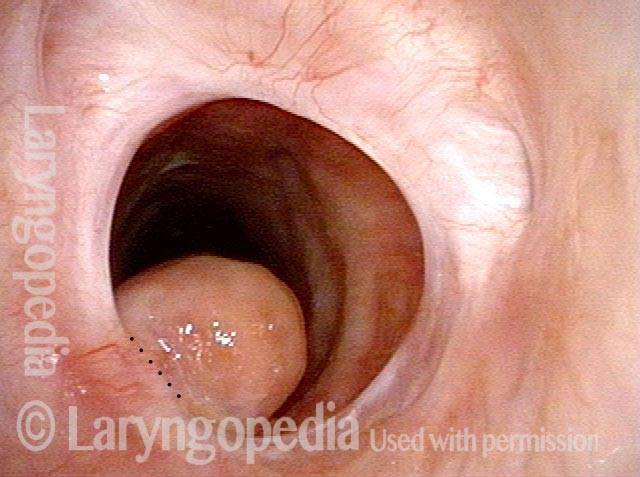
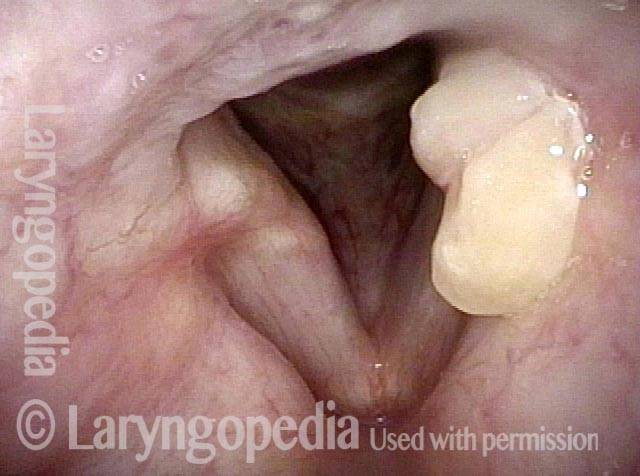
Un approccio migliore è semplicemente aspettare che il granuloma si stacchi da solo. Questo processo di autodistacco, che può richiedere diversi mesi, è come una mela che matura e poi cade dall’albero: il granuloma continua a crescere di dimensioni e, una volta diventato abbastanza grande, il movimento avanti e indietro dell’aria e lo spostamento provocato dal contatto con la cartilagine aritenoidea opposta fa sì che il granuloma si pizzichi lentamente verso l’interno alla sua base e diventi sempre più peduncolato. Alla fine, il peduncolo connettivo non riesce più a sostenere il granuloma e il granuloma si libera. Per un esempio, guarda le foto qui sotto.
Se i sintomi di una persona sono troppo fastidiosi per aspettare mesi, allora il granuloma può essere rimosso chirurgicamente, ma lasciando comunque parte del gambo o della base sporgente dalla superficie, in modo da evitare di ledere nuovamente la cartilagine e il pericondrio, che provocherebbe la formazione di un altro granuloma.

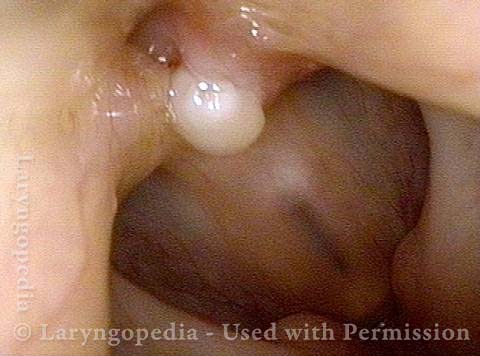
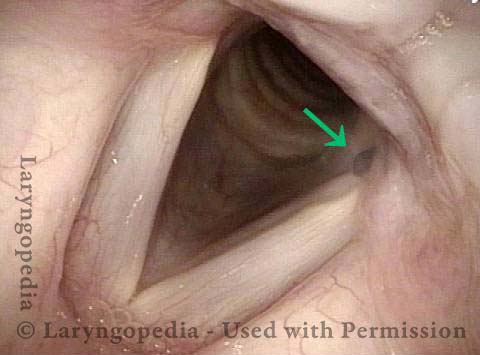
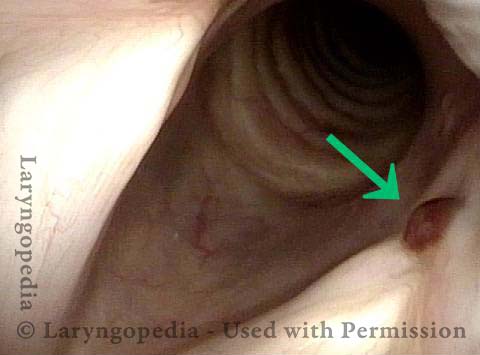
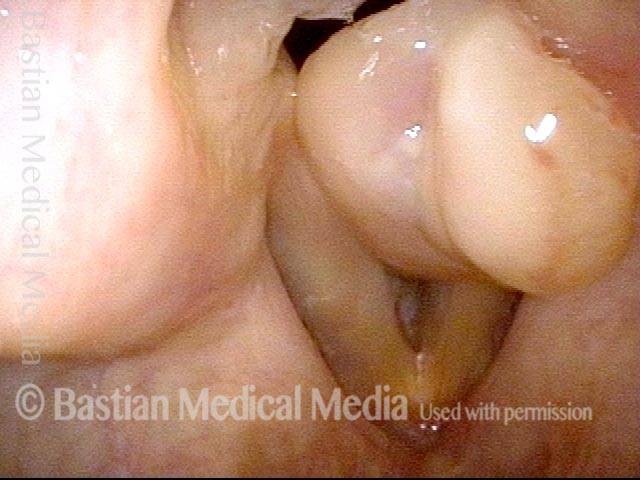
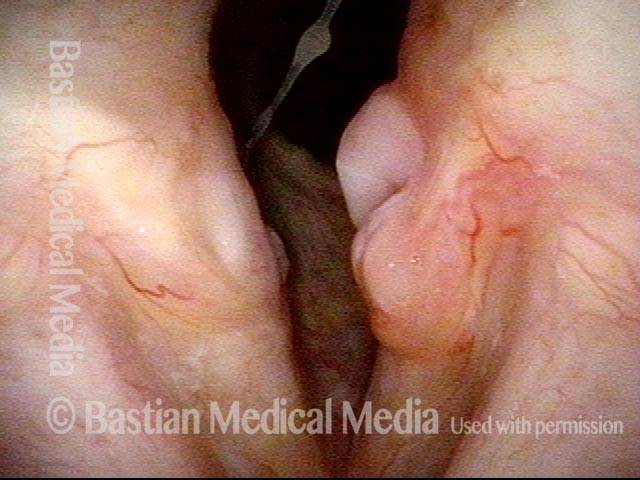
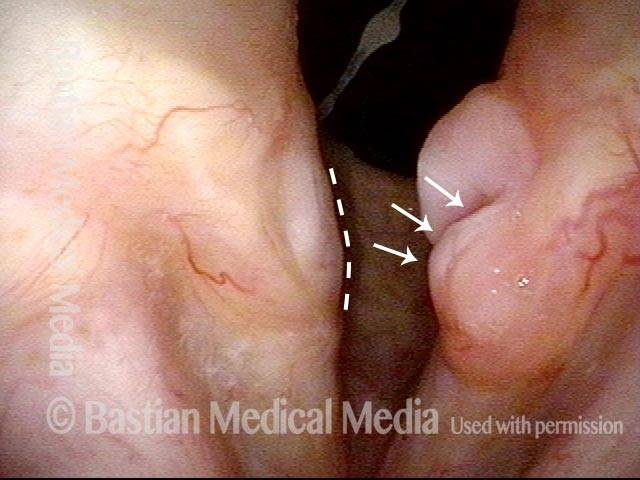
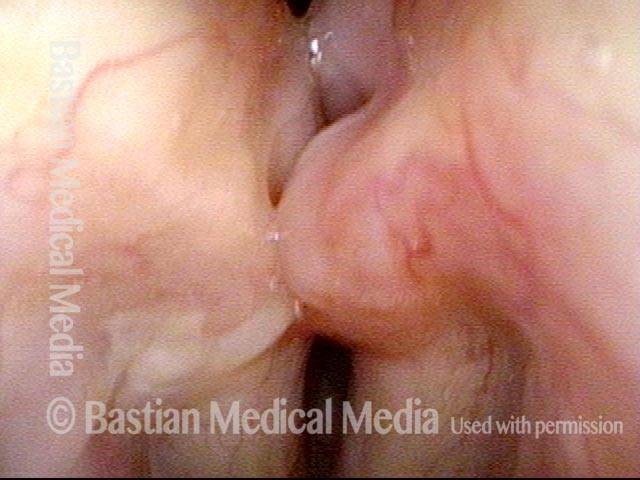
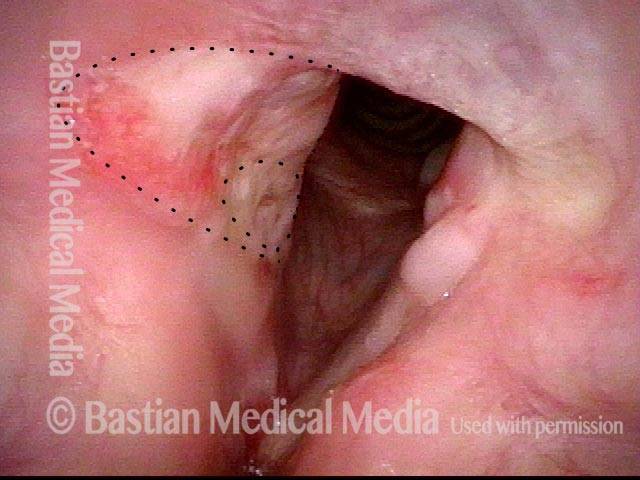
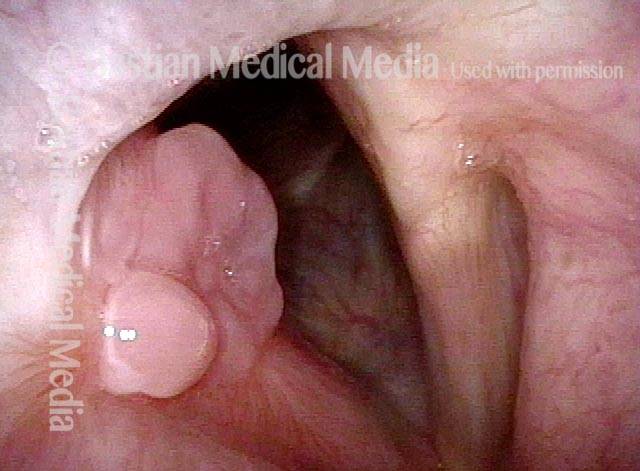
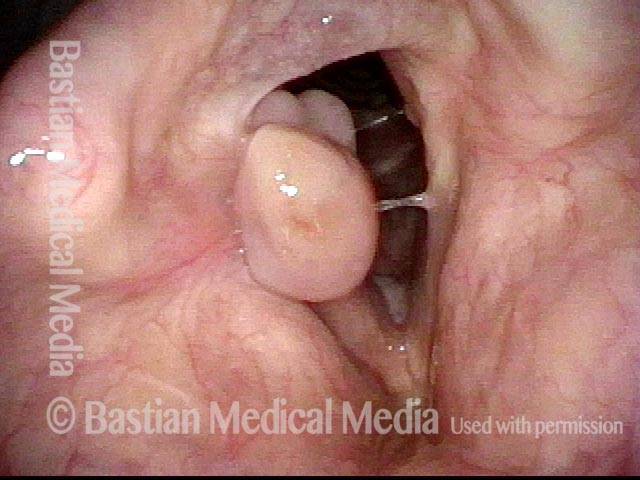
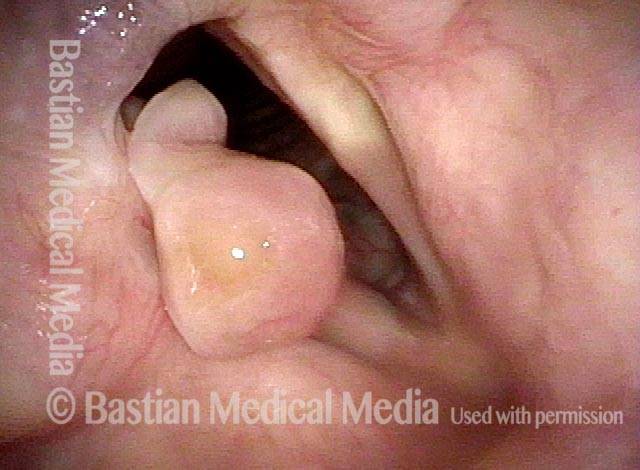
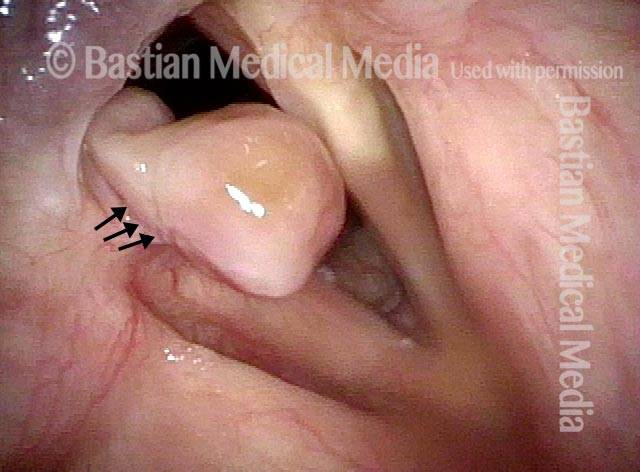
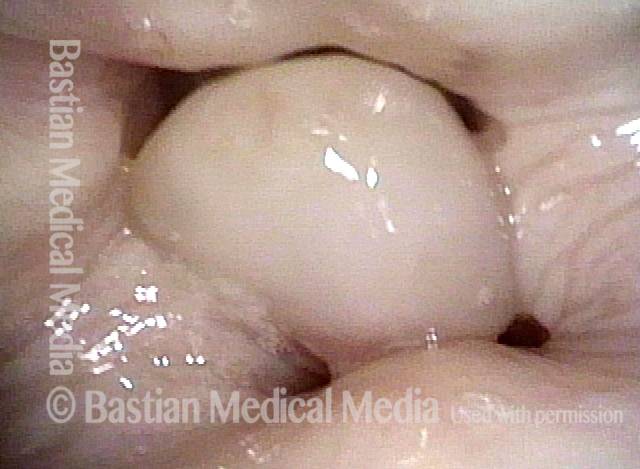
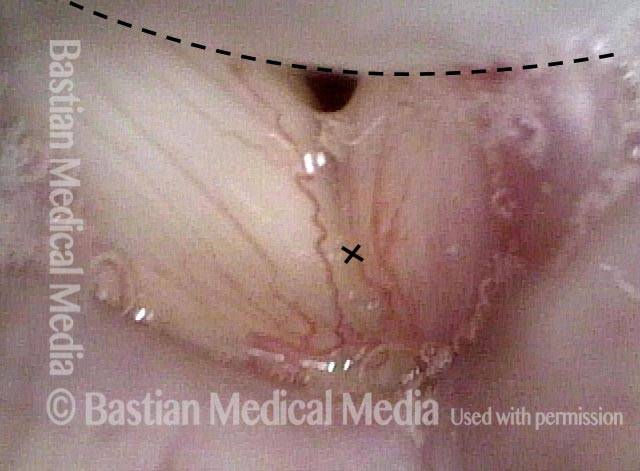
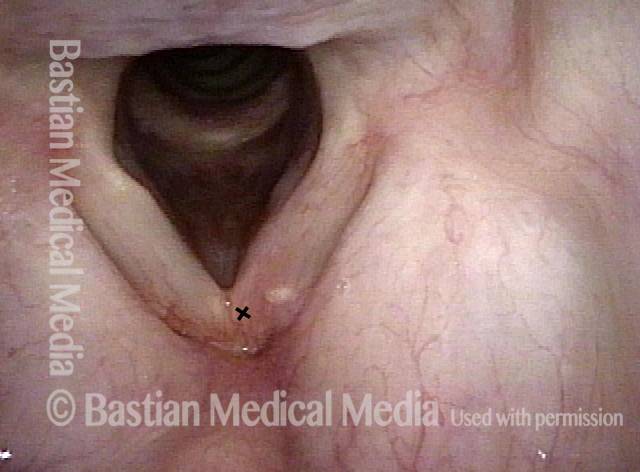
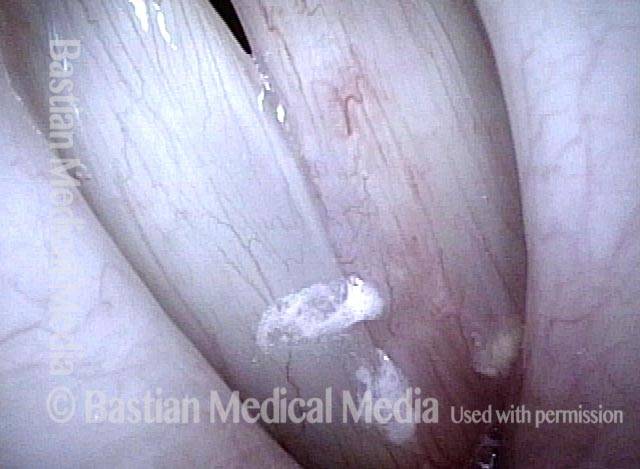
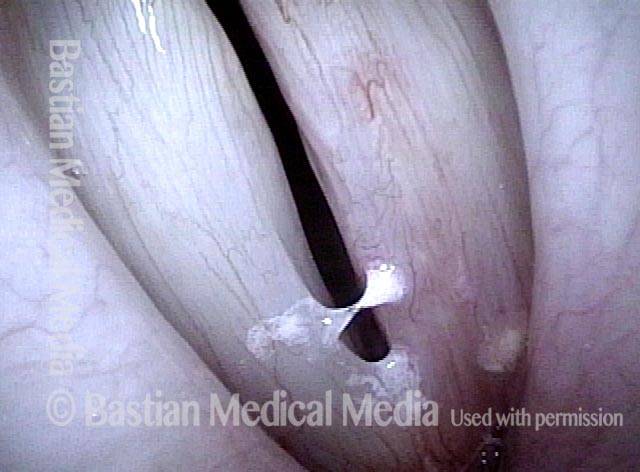
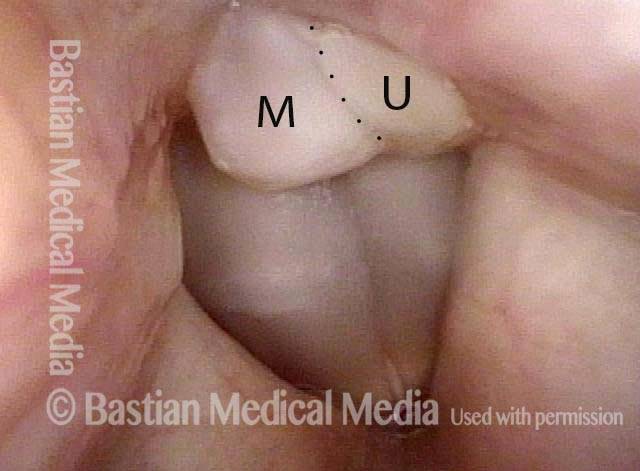
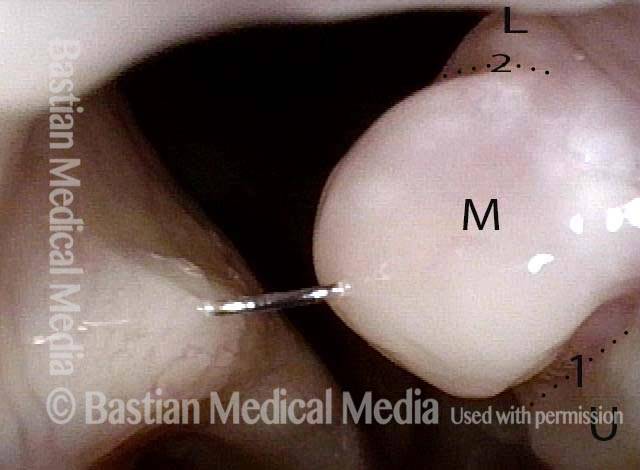
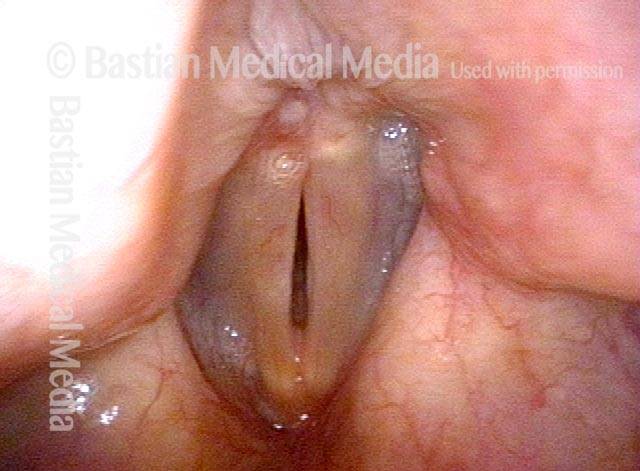
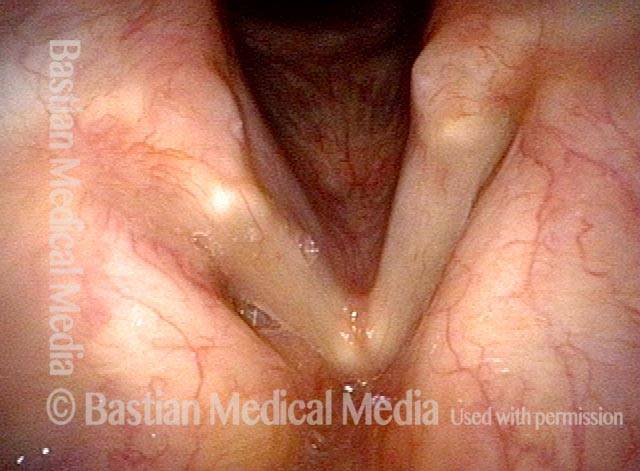
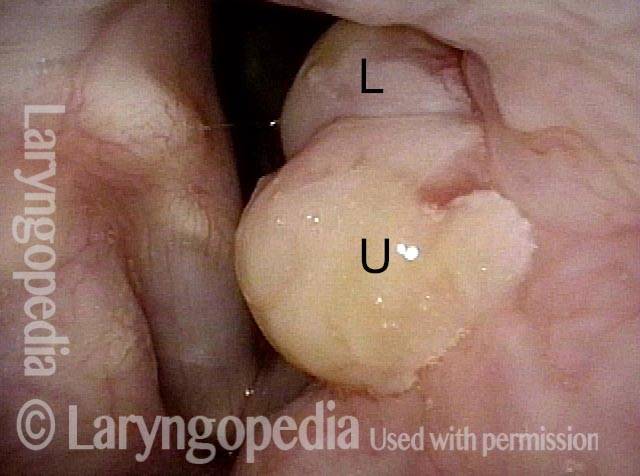
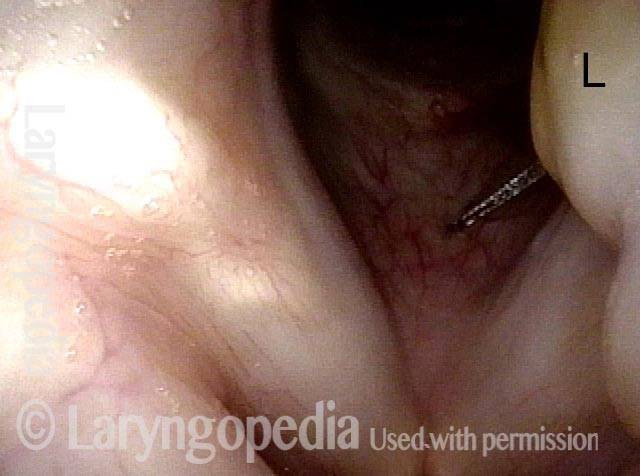
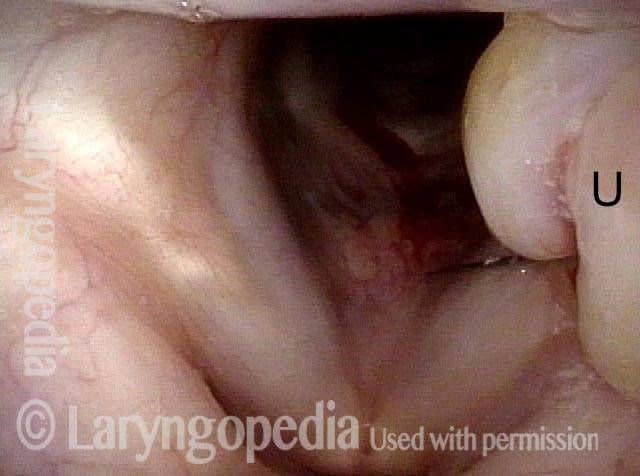
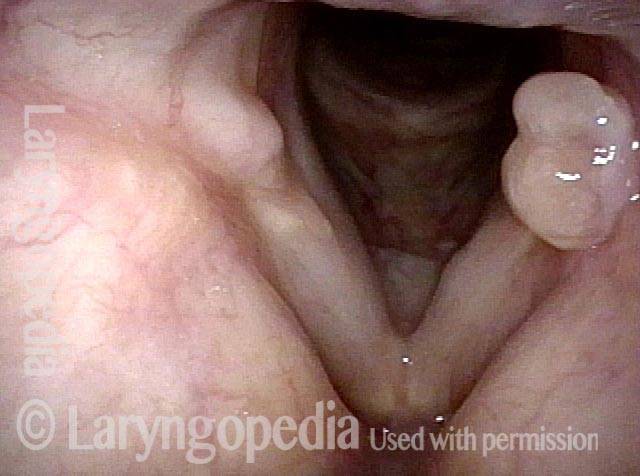
Inserimento “Maschio e Femmina” di un Granuloma da Contatto Bilobato
Quest’uomo sperimenta un dolore acuto e momentaneo quando parla per la prima volta dopo un intervallo di silenzio. È stato sottoposto a biopsia altrove ma la lesione (un granuloma da contatto) è ritornata, come ci si aspetterebbe, a causa di una nuova lesione del pericondrio aritenoideo.
Come spiegato altrove, i granulomi da contatto possono essere diagnosticati in base a “certi” criteri visivi e possono maturare e staccarsi spontaneamente, senza necessità di rimozione se non in circostanze insolite.
Tongue and groove (1 of 4)

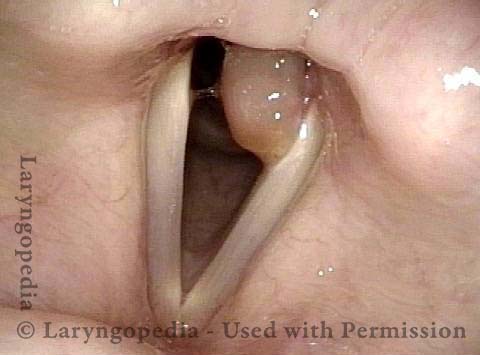
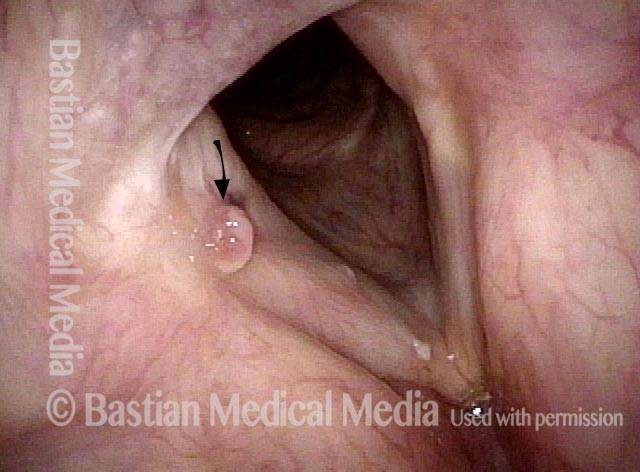
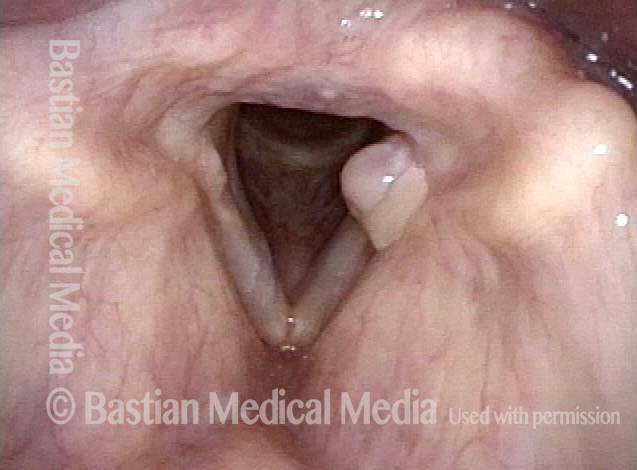
Bi-lobed lesion (2 of 4)

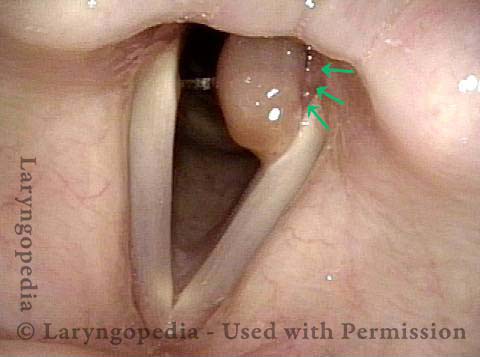
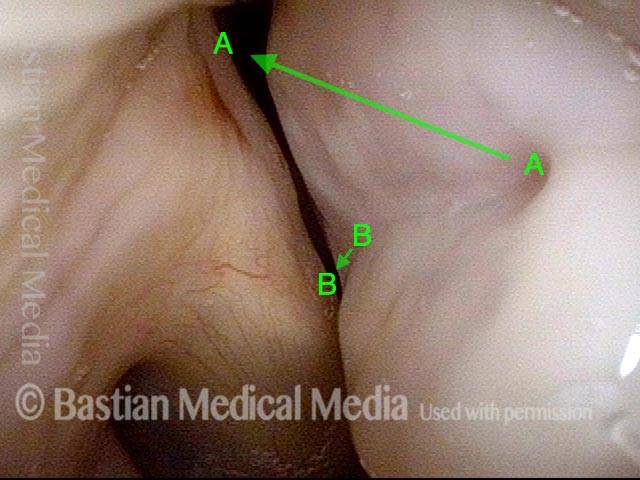
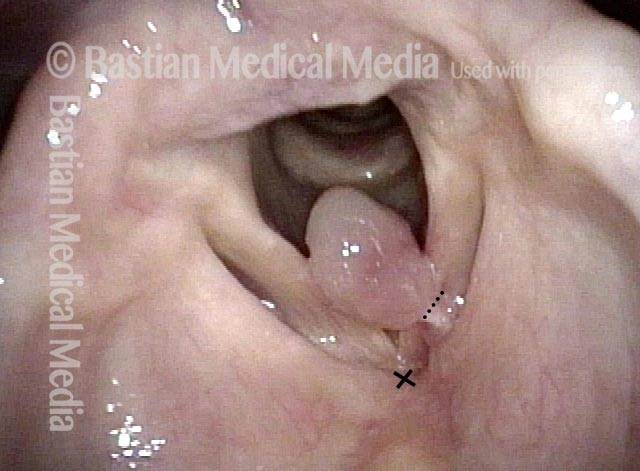
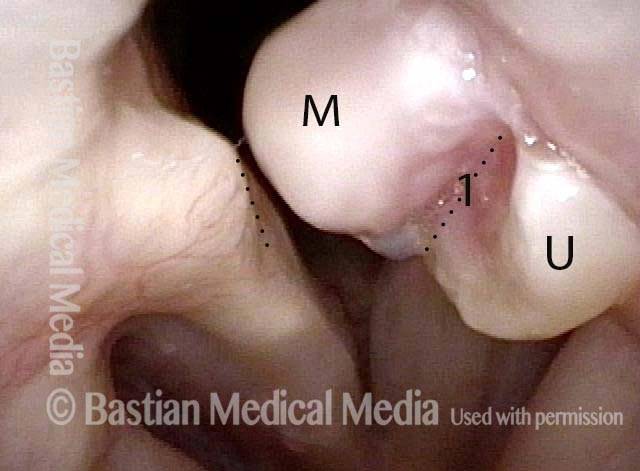
Bi-lobed morphology of granuloma (3 of 4)

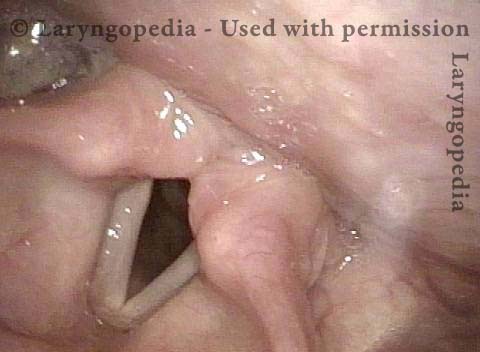
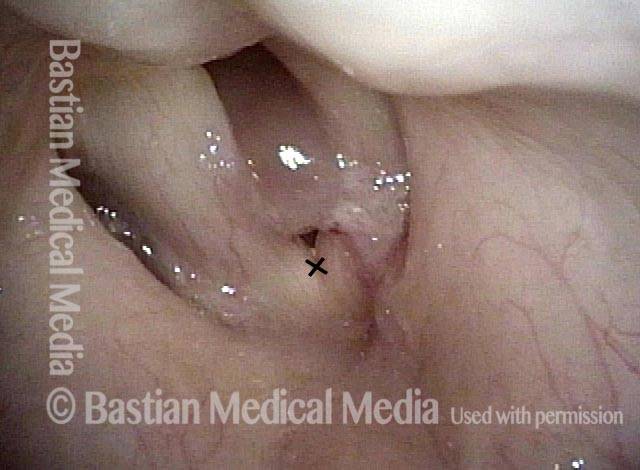
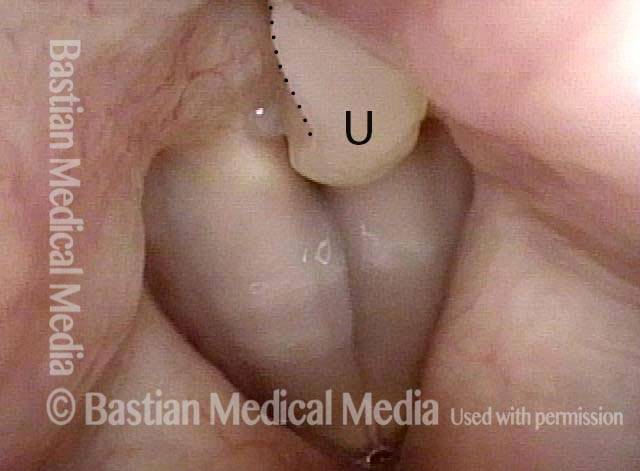
Tongue and groove fit between cords (4 of 4)
“Tatuaggio” di sangue dopo distacco di granuloma da intubazione
Intubation granuloma (1 of 5)
Pedunculation in process (2 of 5)
Granuloma is gone (3 of 5)
Blood tattoo (4 of 5)
Blood Tattoo (5 of 5)
Granuloma da Contatto
Residual haziness (1 of 2)
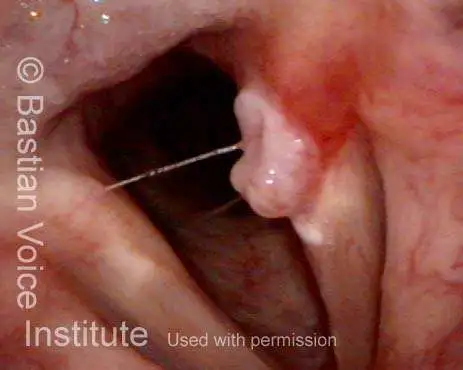
Bi-lobed granuloma (2 of 2)

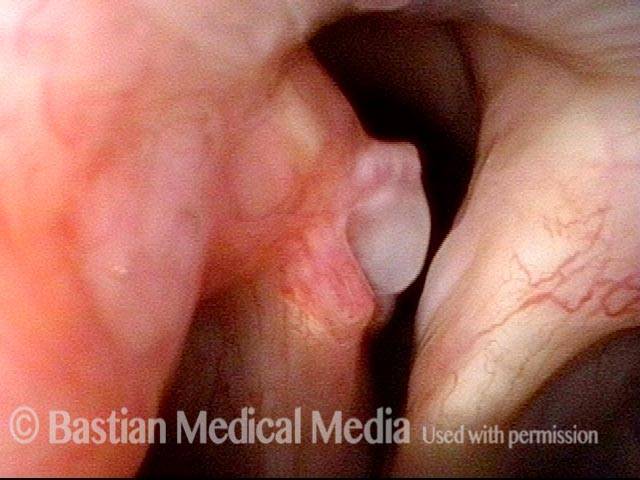
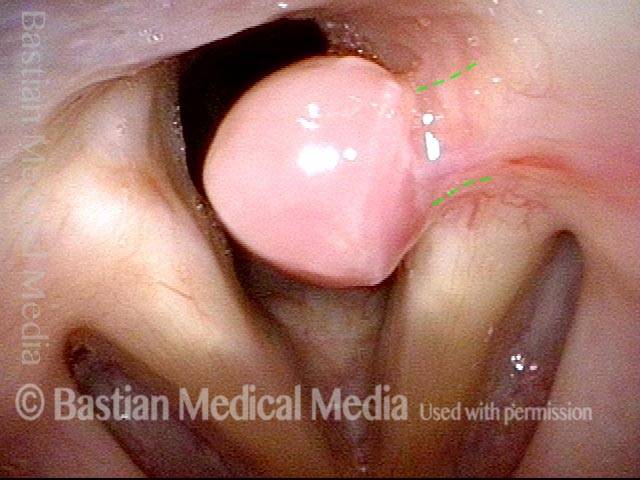
Esempio 2
Bi-lobular Granuloma (1 of 2)

Arytenoid cartilage fits into cleft (2 of 2)
I Granulomi da Intubazione Possono Essere Lasciati soli a Maturare e a Staccarsi Spontaneamente
Intubation Granuloma (1 of 3)

Pedunculated Granuloma (2 of 3)

Pedunculation in process (3 of 3)
{kind=link}
Granuloma di Contatto, Gradualmente Peduncolato e Poi Distaccato
Bi-lobed granuloma (1 of 11)

Granuloma displaces upwards (2 of 11)
Vocal process fits in granuloma cleft (3 of 11)
Granuloma doesn’t affect voice (4 of 11)

2 months later (5 of 11)
Granuloma slowly penduculates (6 of 11)

2 months later (7 of 11)

Granuloma detached (8 of 11)
5 months later (9 of 11)

One year later (10 of 11)

One year later (11 of 11)

“Vestibilità Key-in-lock”
Bi-lobed granuloma (1 of 3)
Key-in-lock granuloma (2 of 3)
Cleft and bi-lobularity (3 of 3)
La Sequenza di Guarigione della Granulazione
Large tumor, before removal (1 of 8)
After tumor removal (2 of 8)
2 months after surgery (3 of 8)
5 Months after surgery, a granuloma is seen (4 of 8)
7 months after surgery (5 of 8)
Pedunculation (6 of 8)
One year after surgery (7 of 8)
15 months after surgery (8 of 8)

Corda Vocali “Lacrima” e Granuloma
Intubation injury (1 of 8)
Granuloma drawn into glottis (2 of 8)
Phonation (3 of 8)
Anterior commissure (4 of 8)
Granuloma detached (5 of 8)
Vocal cord blurring (6 of 8)

Closed phase (7 of 8)
Open phase (8 of 8)
Granuloma da Contatto Trilobato
Panoramic view (1 of 6)
Upper and middle lobule, cleft 1 (2 of 6)
Phonation (3 of 6)
Lower lobule (4 of 6)

Upper and middle lobule, Cleft 2 (5 of 6)
Tri-lobed (6 of 6)
Tipo Ulcera con Bordo Arrotolato
Persistent granuloma (1 of 4)
Narrow band light (2 of 4)
Phonation (3 of 4)
One year later (4 of 4)
Evoluzione della Cicatrice Tracheale Circolare Compreso il Granuloma
Two weeks post-op (1 of 4)

Six weeks post-op (2 of 4)
Inhaling (3 of 4)
Rapid inhalation (4 of 4)

I Granulomi Maturano e Cadono da Soli, ma l’iniezione di Steroidi può Aiutare…
“Third” granuloma (1 of 6)
Injection into lower lobe (2 of 6)
Injection into upper lobe (3 of 6)
Five weeks later (4 of 6)
Six months post-injection (5 of 6)
One year post-injection (6 of 6)