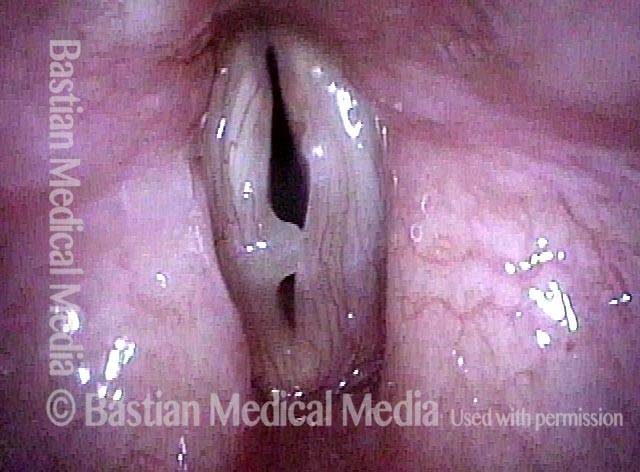
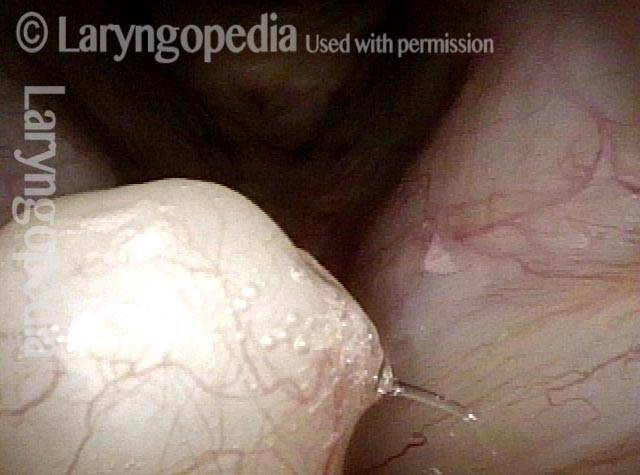
I polipi sono un grande rigonfiamento sulla corda vocale che tipicamente si verifica unilateralmente, cioè senza un rigonfiamento simile sulla corda opposta. Il termine polipo vocale è alquanto impreciso, ma i polipi vocali possono essere distinti da un tipo simile di gonfiore, i noduli vocali, in almeno due modi:
- I polipi tendono ad essere più grandi dei noduli.
- I polipi si presentano unilateralmente o sono notevolmente più grandi di una lesione della corda vocale opposta, mentre i noduli si presentano in coppie e sono generalmente di dimensioni simili.
I polipi e i noduli vocali sono causati almeno in parte da traumi vibratori, dovuti a un uso eccessivo della voce acuto (con polipi) o cronico.
Un polipo vocale disturba la chiarezza della voce e altre capacità interferendo con l’approssimazione accurata delle corde vocali durante la fonazione. Un polipo può anche aggiungere massa alle corde vocali, riducendo così la gamma tonale disponibile per la voce. I polipi possono essere definiti emorragici, peduncolati e così via.
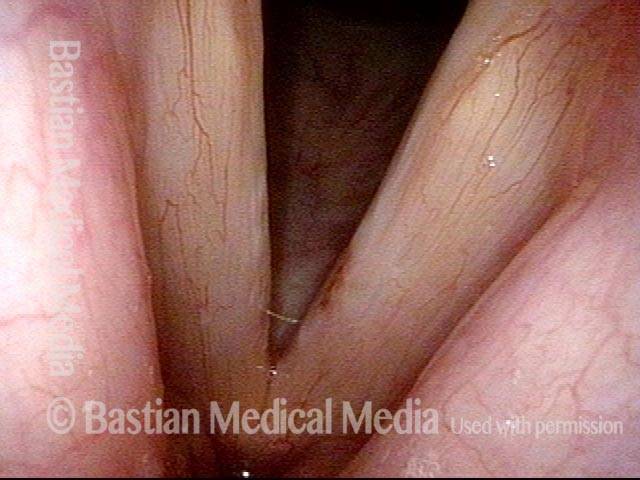
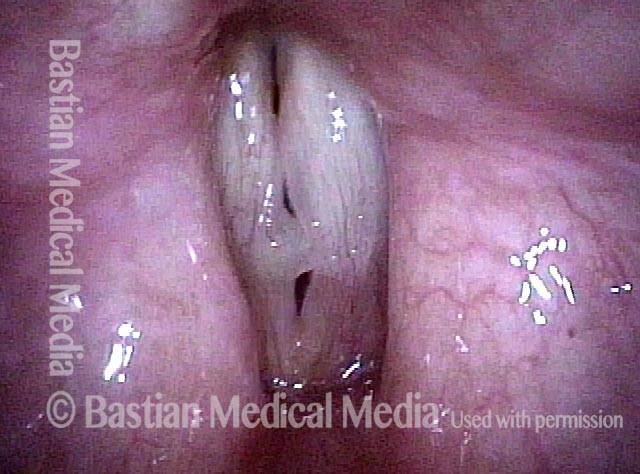
Polipi vocali rimossi e poi ricorrenti
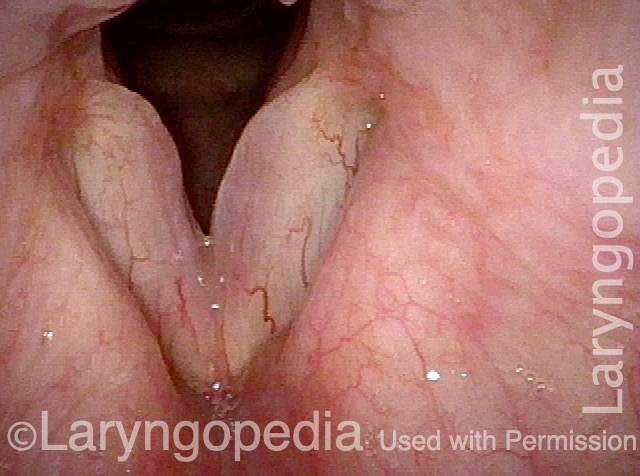
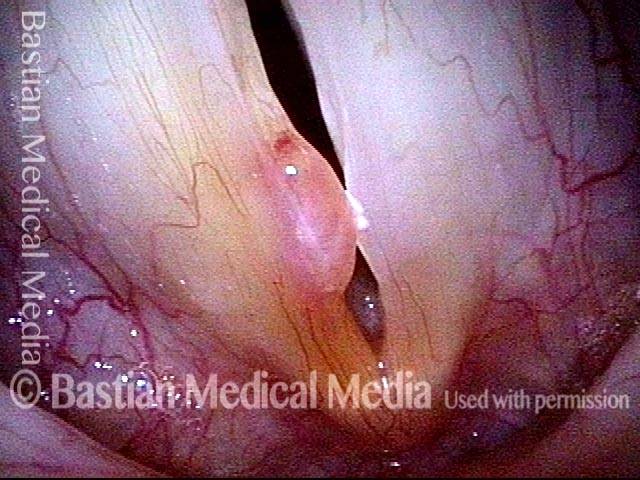
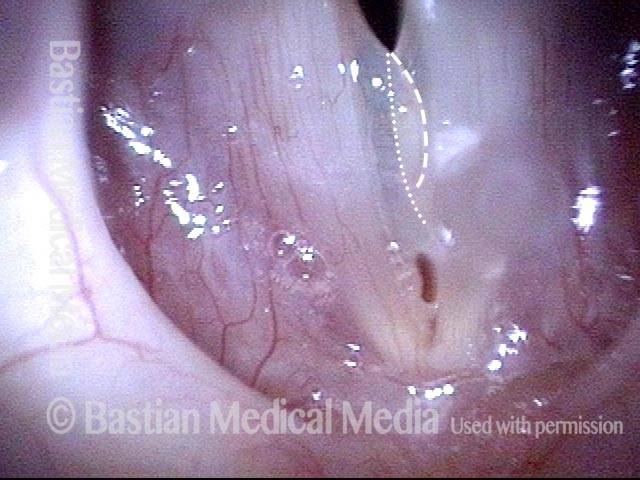
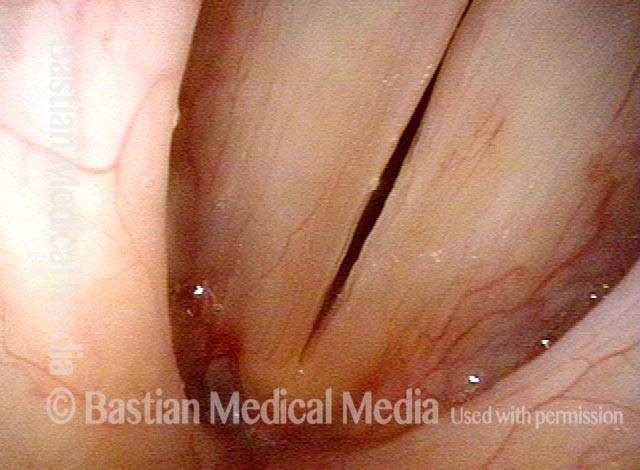
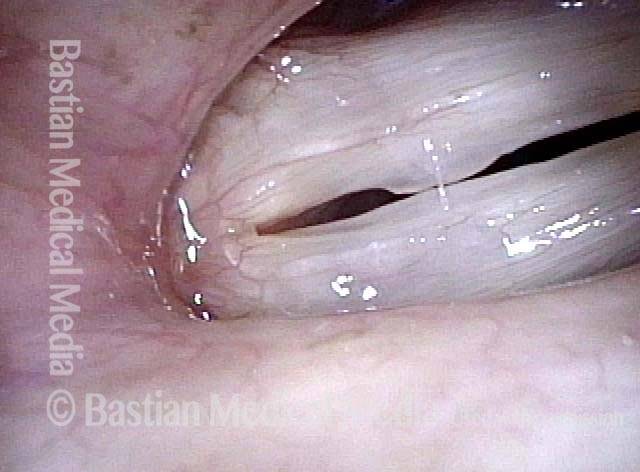
Vocal polyp (1 of 4)
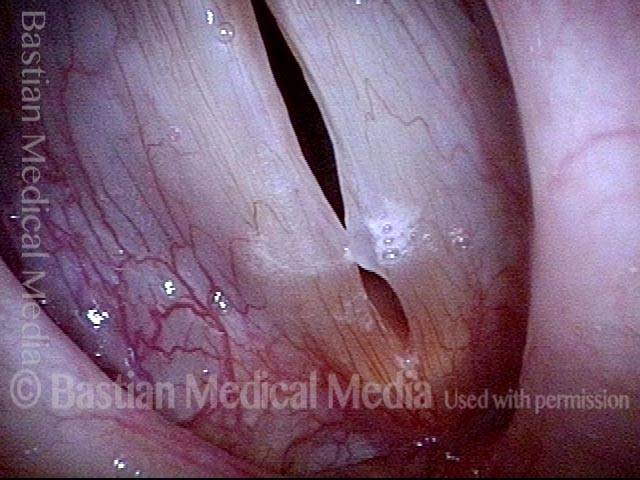
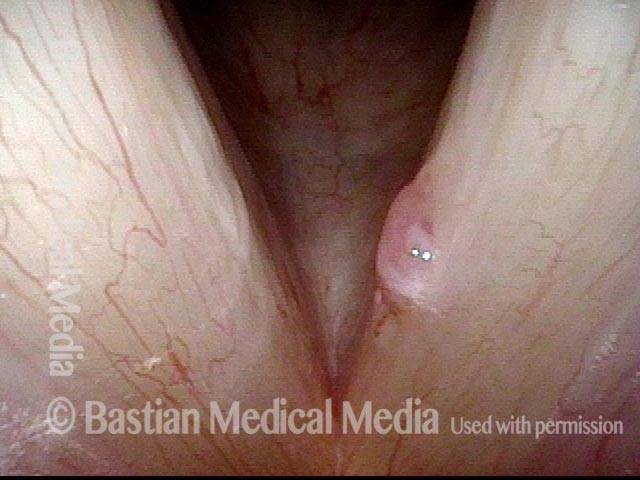
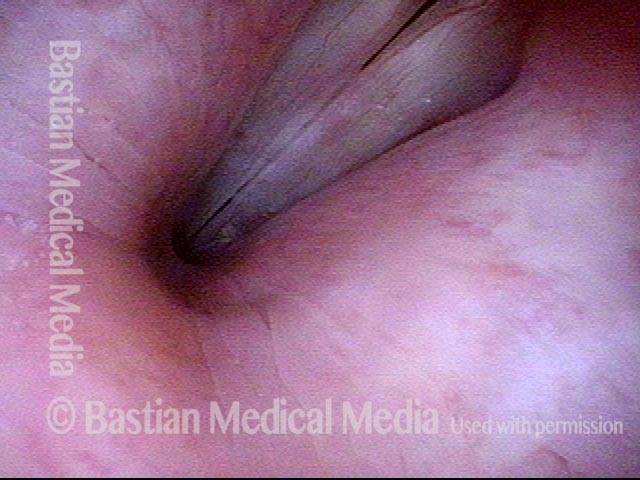
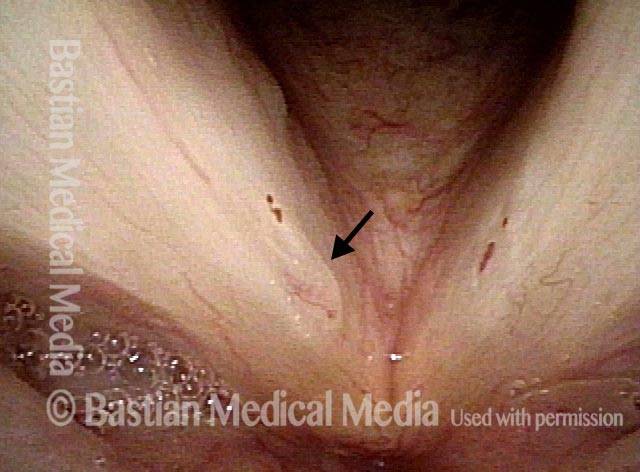
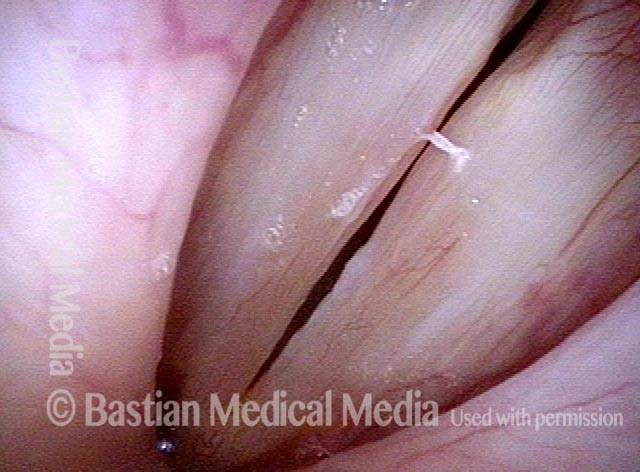
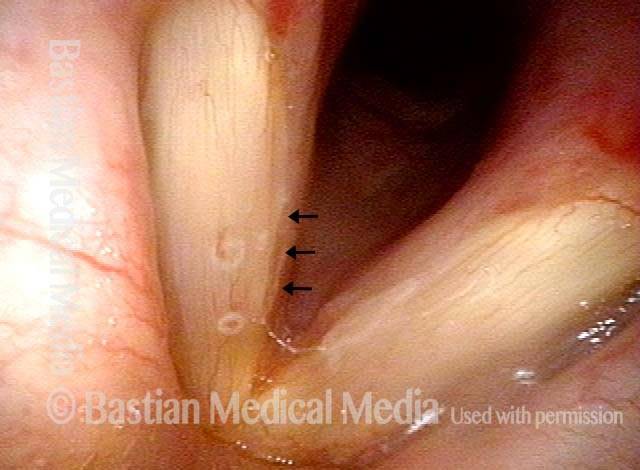
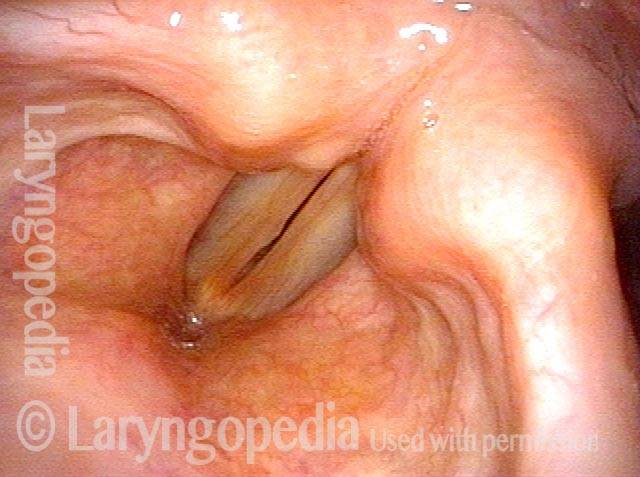
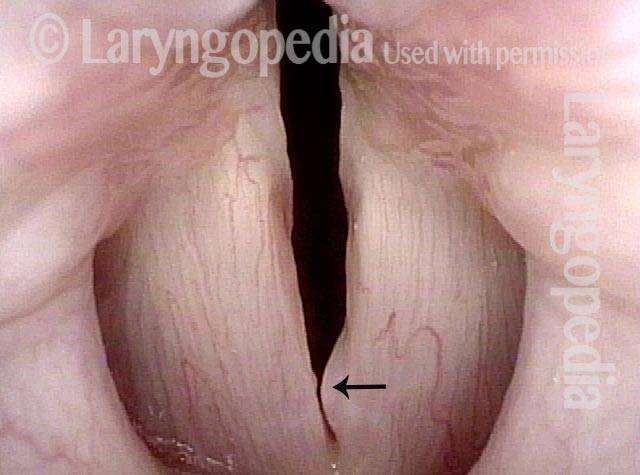
Vocal polyp (2 of 4)
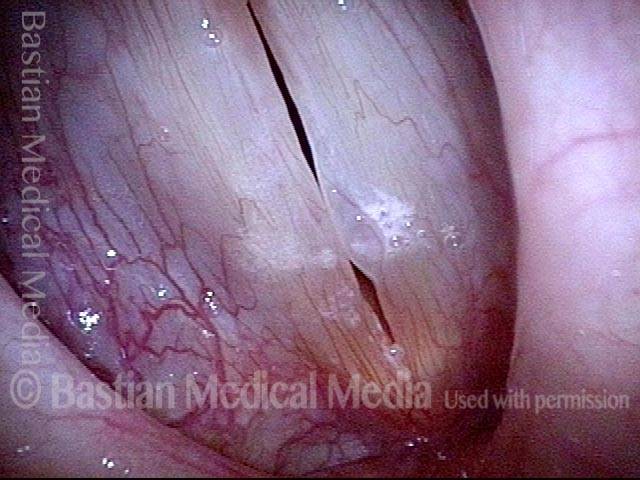
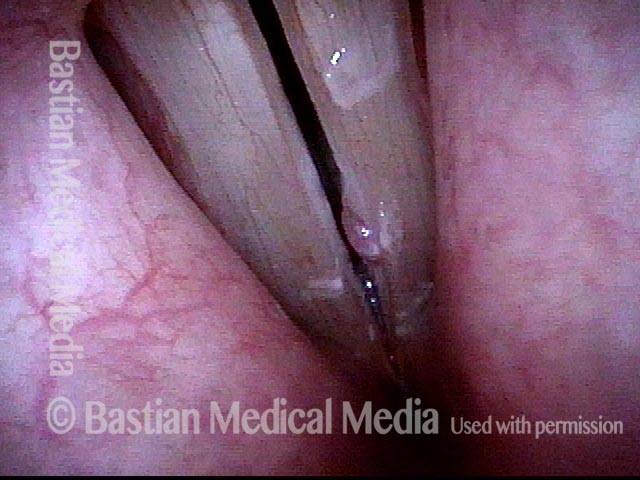
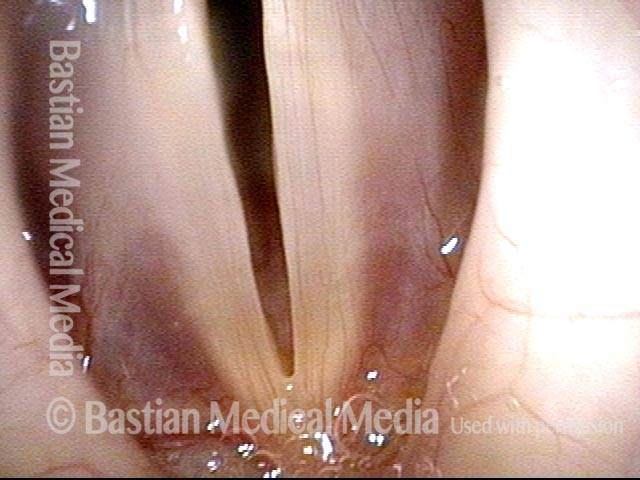
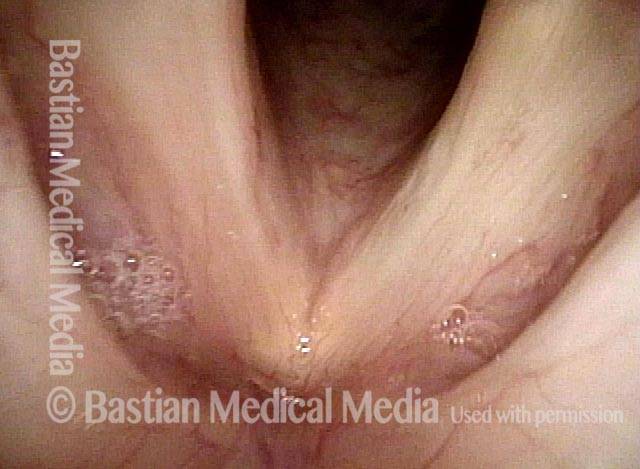
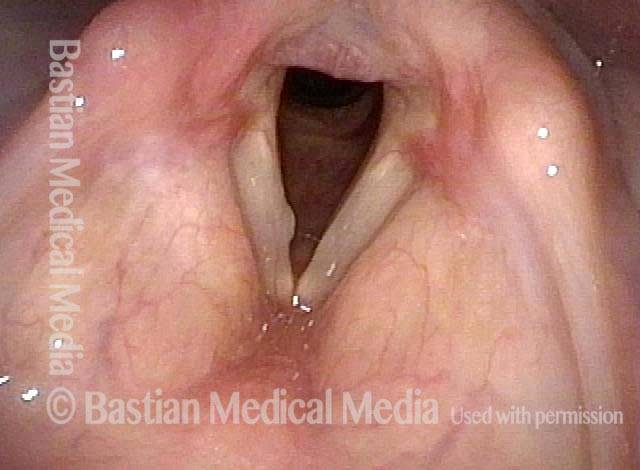
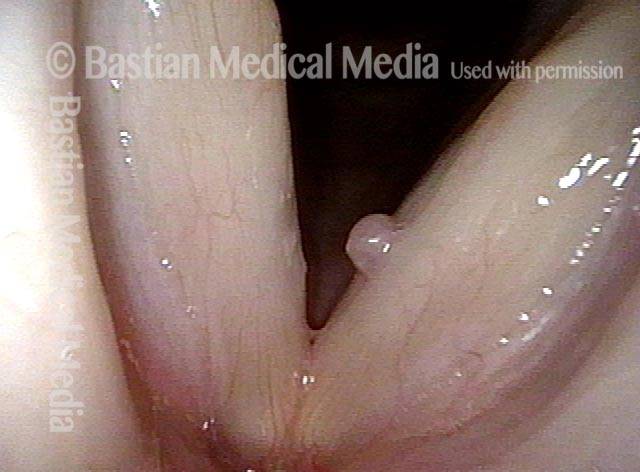
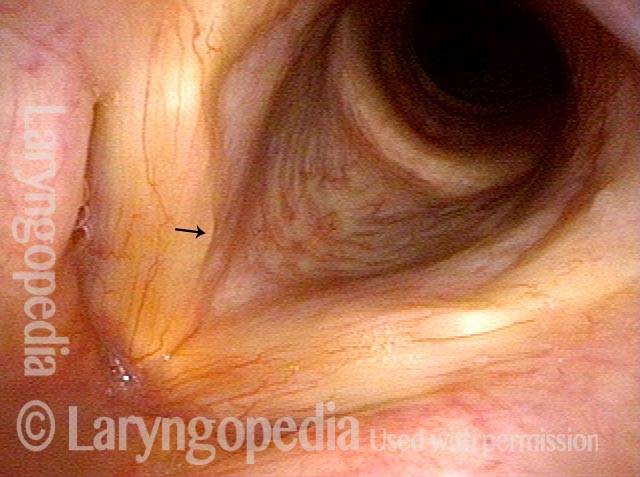
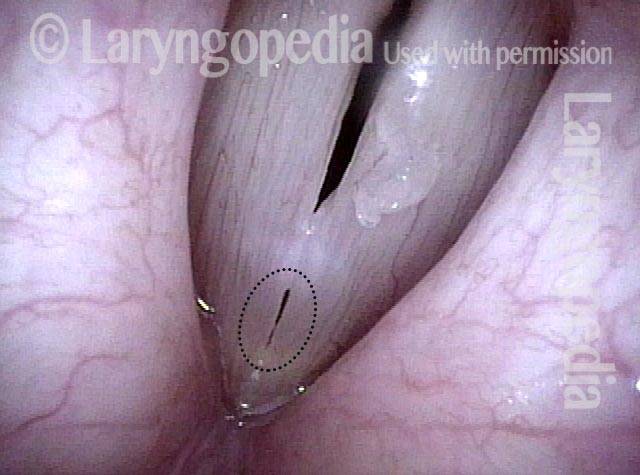
Vocal polyp, one week after surgical removal (3 of 4)

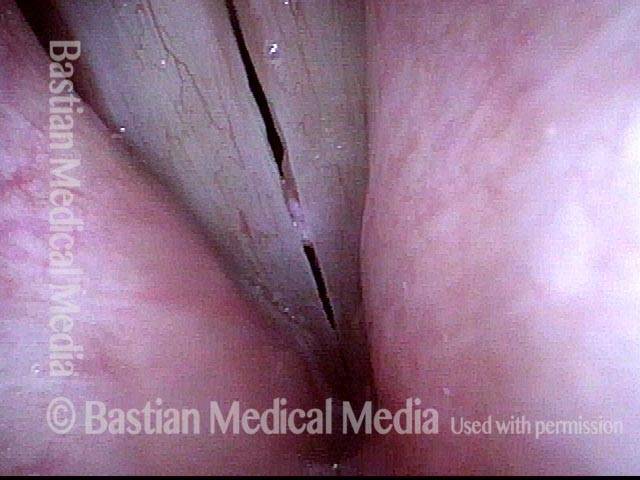
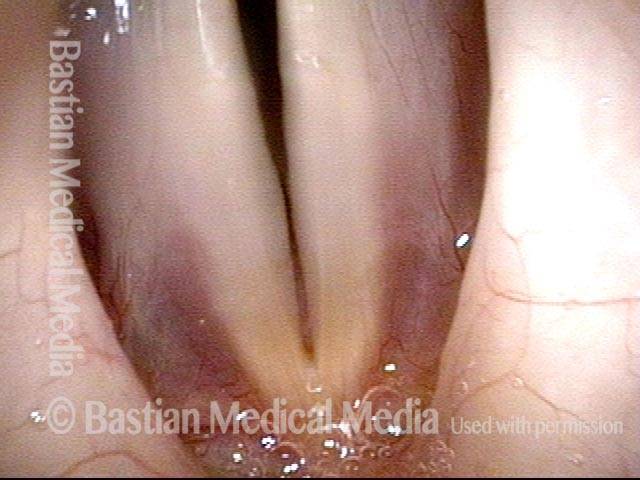
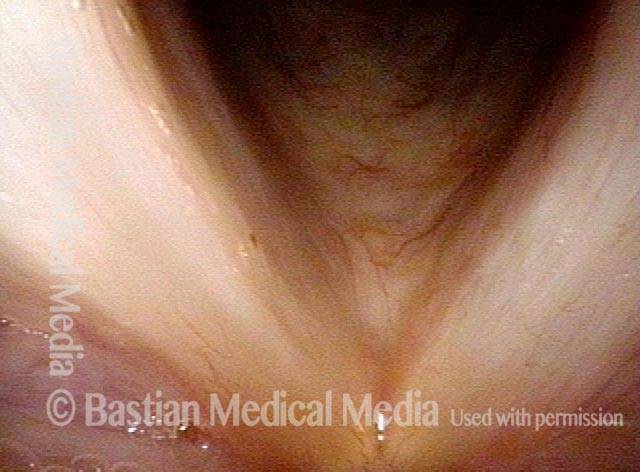
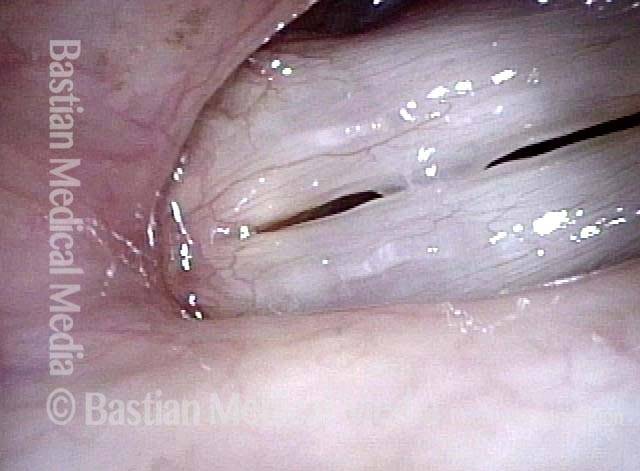
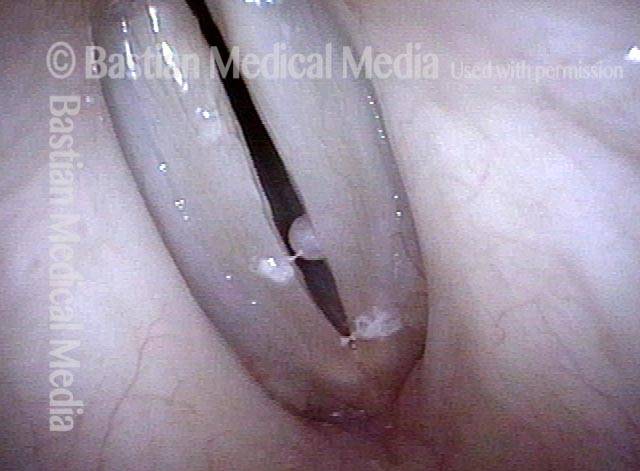
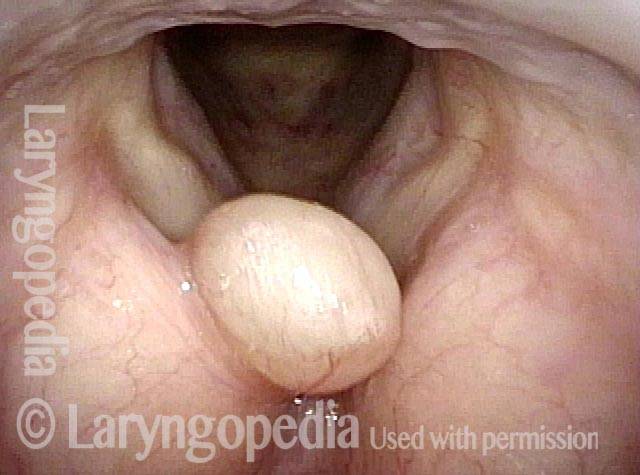
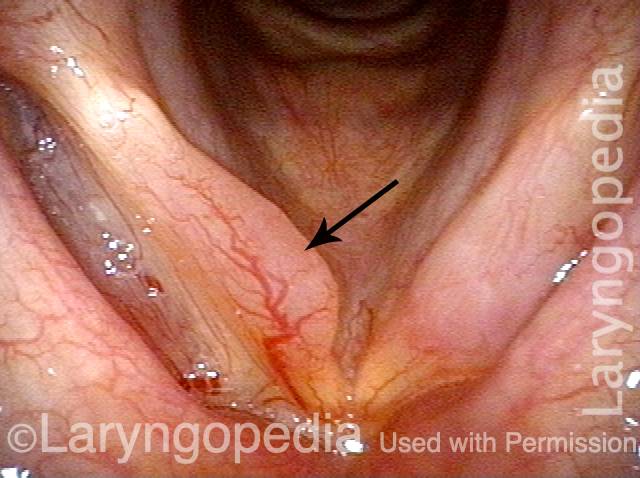
Vocal polyp, subsequent new injury (4 of 4)
Polipi vocali, prima e dopo l’intervento chirurgico
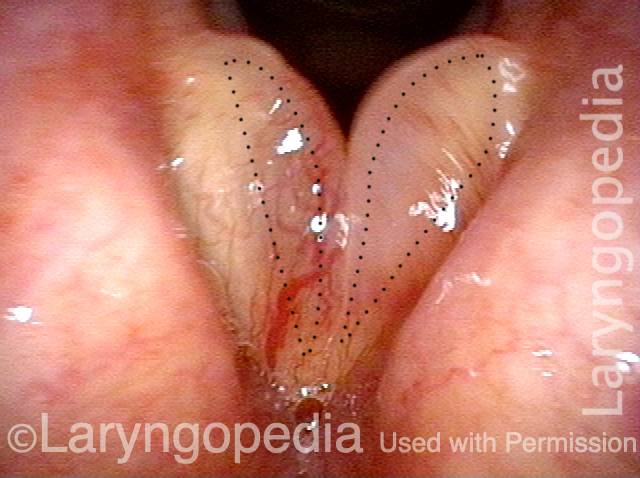
Vocal polyp (1 of 6)
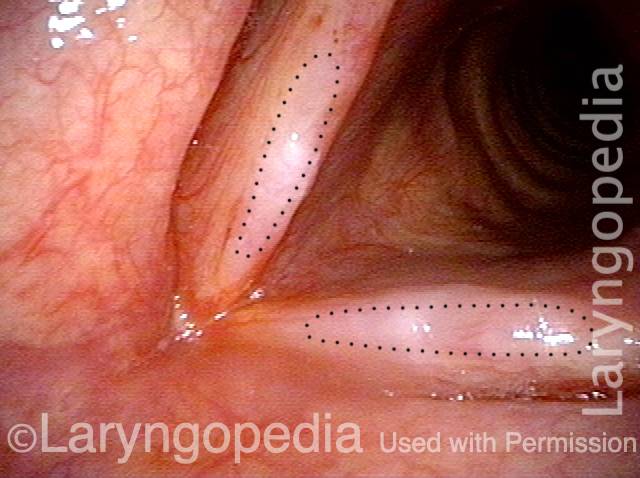
Vocal polyp (2 of 6)
Vocal polyp (3 of 6)
Vocal polyp, surgically removed (4 of 6)
Vocal polyp, surgically removed (5 of 6)

Vocal polyp, surgically removed (6 of 6)
Esempio 2
Vocal polyp (1 of 2)

Vocal polyp, surgically removed (2 of 2)

Esempio 3
Vocal polyp (1 of 6)

Vocal polyp (2 of 6)

Vocal polyp, surgically removed (3 of 6)
Vocal polyp, surgically removed (4 of 6)
Vocal polyp, surgically removed (5 of 6)
Vocal polyp, surgically removed (6 of 6)
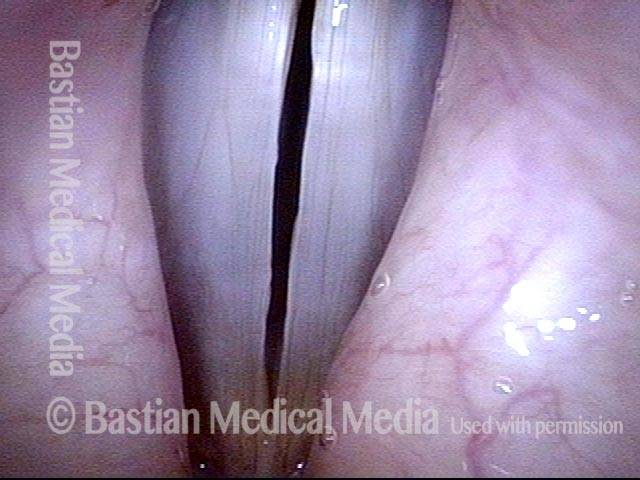
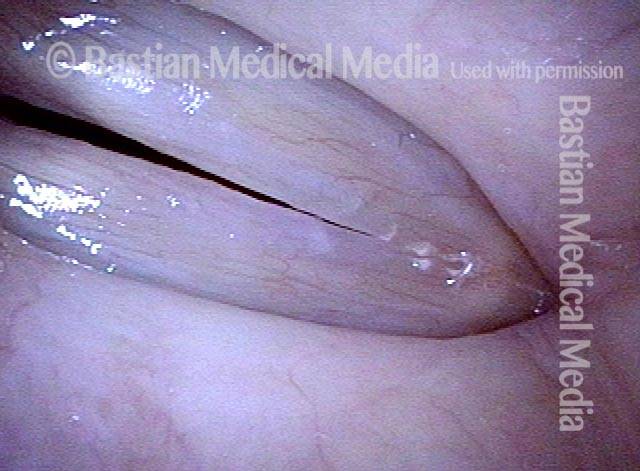
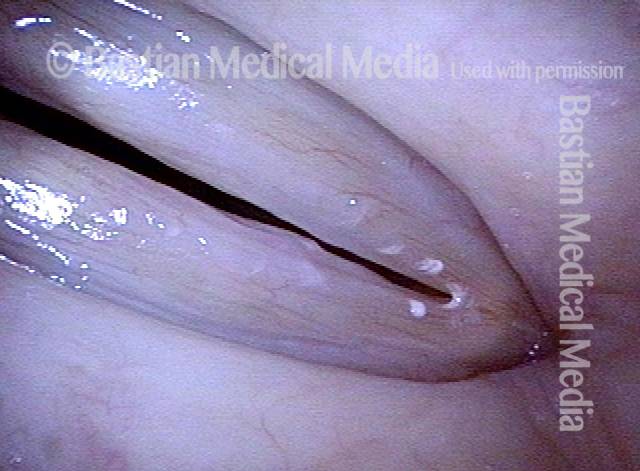
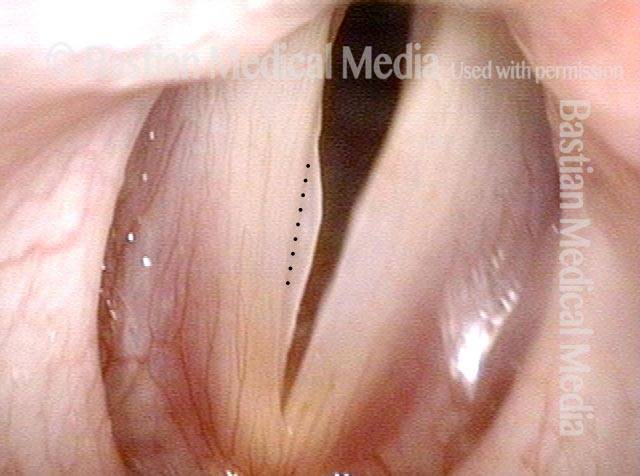
Polipo traslucido
Translucent polyp (1 of 4)

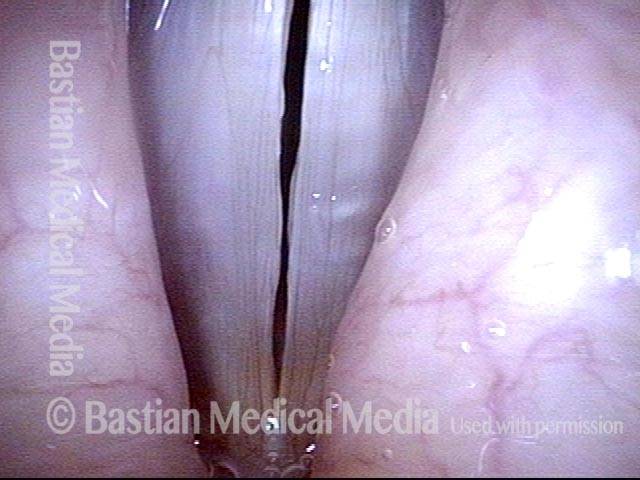
Translucent polyp (2 of 4)
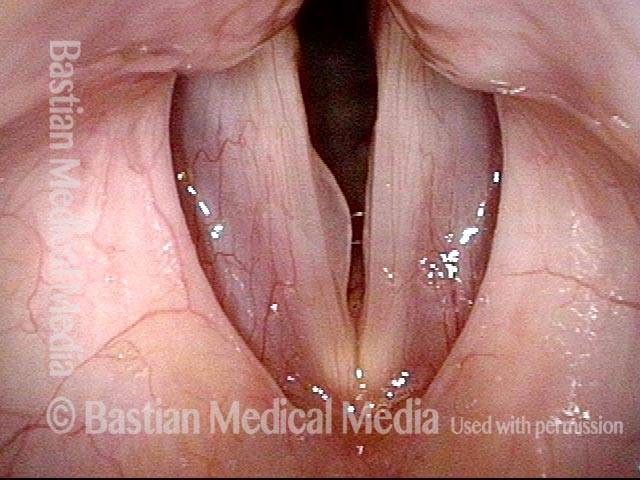
Translucent polyp (3 of 4)
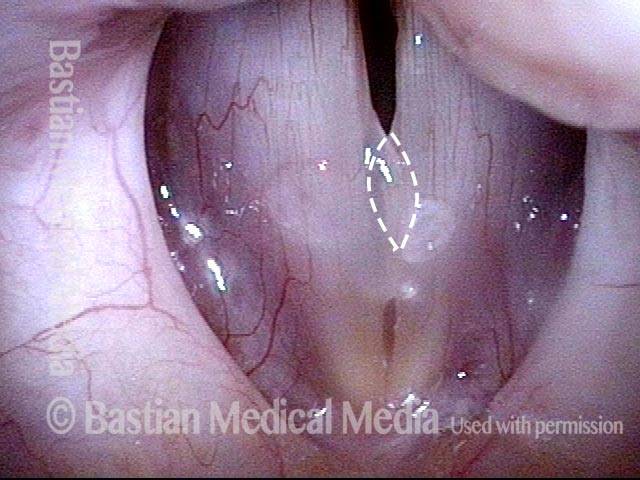
Translucent polyp (4 of 4)
Rimosso polipo di cantante lirico con ripristino delle capacità originarie
Polyp and capillary ectasia (1 of 8)
Prephonatory instant (2 of 8)

One week post-op (3 of 8)
Prephonatory instant (4 of 8)

One month post-op (5 of 8)
Prephonatory instant (6 of 8)
Closed phase (7 of 8)

Open phase (8 of 8)
Polipo di un’attrice prima e ore dopo la rimozione chirurgica
Vocal cord polyp (1 of 8)
Closer view (2 of 8)

Closed phase (3 of 8)
Open phase (4 of 8)
24 hours post surgery (5 of 8)

Primary “wound” (6 of 8)
Closed phase (7 of 8)

Open phase (8 of 8)

Il cavo operato ha un aspetto migliore rispetto al cavo non operato
Singer with chronic hoarseness (1 of 4)
Attempting phonation (2 of 4)
One week post surgical removal (3 of 4)
Open phase (4 of 4)
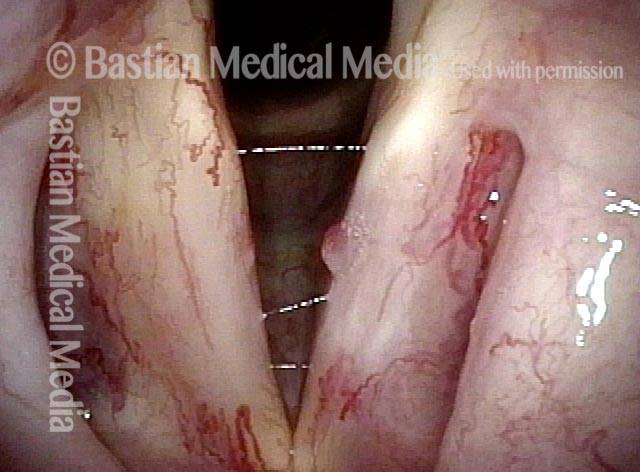
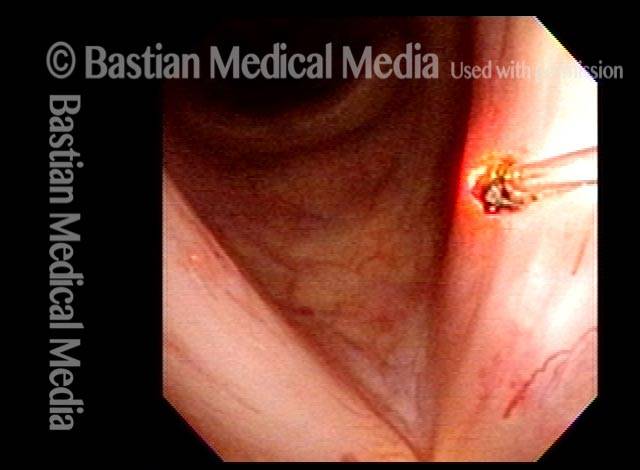
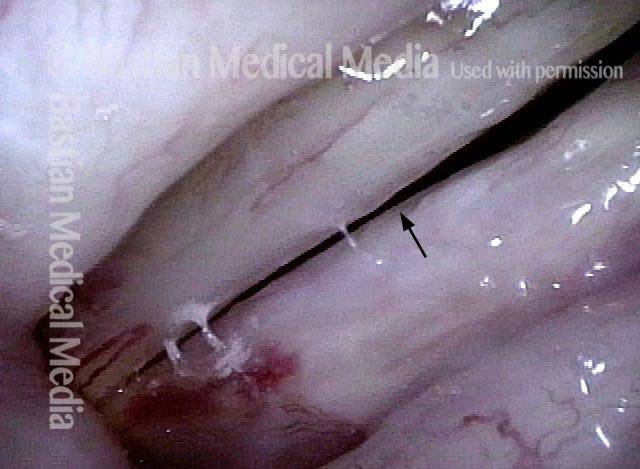
Laser da ufficio del polipo telangiectasico post-radiazione
Post-radiation telangiectasias (1 of 4)
Pulsed-KTP coagulation (2 of 4)
“Polyp” pulled off (3 of 4)

Three weeks later (4 of 4)
Sfumature “raccolte” dagli esami quotidiani
Vocal “overdoer” (1 of 4)
Inspiratory phonation (2 of 4)
Translucent polyp (3 of 4)

Open phase (4 of 4)

L’espressione della lesione nella mucosa varia
Vocal cord injuries (1 of 4)

Narrow band lighting (2 of 4)

Strobe lighting (3 of 4)
Phonation (4 of 4)
Il potere di vedere un polipo “vicino-chiaro” e non “lontano-sfocato”.
Disant view (1 of 4)
Closer view (2 of 4)
Close-clear view (3 of 4)

Open phase (4 of 4)

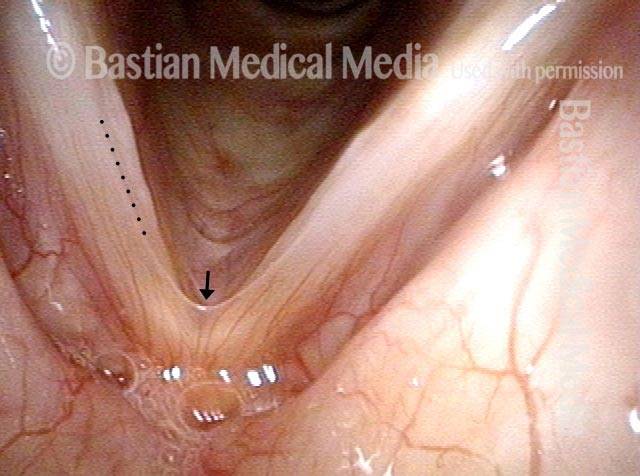
Polipo o cisti?
Hoarseness (1 of 4)

Position of lesion (2 of 4)
Close view (3 of 4)
Anterior saccular cyst (4 of 4)

Il piccolo segmento vibrante dà la voce di un piccolo fischio di latta
Prephonatory instant (1 of 6)
Phonation (2 of 6)

Gaps due to nodules (3 of 6)

Open phase (4 of 6)

“Tin whistle” sound (5 of 6)
“Tin whistle” at open vibration (6 of 6)

La riduzione dei polipi del fumatore migliora la voce anche se il risultato della laringe potrebbe non essere “carino”
Smokers Polyp (1 of 5)
Reine’s edema (2 of 5)
A week after surgery (3 of 5)
Residual Reinke’s edema (4 of 5)

Residual submucosal edema (5 of 5)