Vocal cord microsurgery (microlaryngoscopy) is an endoscopic procedure focused upon the larynx, performed under general anesthesia. A hollow lighted tube rests on the upper teeth and the base of the tongue and allows the physician to see the vocal cords. An operating microscope is used to brightly illuminate and highly magnify the vocal cords. Then, tiny instruments and/or a laser are used to remove the abnormality from the vocal cord or cords.
Who Needs Microlaryngoscopy?
The commonest reason is that there is a visible lesion such as nodules, polyps, capillary ectasia (dilated capillaries), epidermoid or mucus retention cyst, glottic sulcus, papilloma, or a known vocal fold cancer. The point is to remove the lesion to improve the sound or capabilities of the voice.
Of course, if a tumor is involved, voice takes second place to removal of the lesion. Removed tissue is always examined by the pathologist, but for most individuals, the need for biopsy is much less than the need for a better voice.
How Is the Procedure Accomplished?
The procedure, aka Microlaryngoscopy, is typically performed in an outpatient operating room during relatively brief general anesthesia. After you are completely asleep, a hollow, lighted “tube”—called a laryngoscope—is placed on the back of the tongue and against the sidewall of the throat, where it rests during the procedure. A microscope is brought into position, aligned with the laryngoscope, and the vocal cords are highly magnified and brightly illuminated.
 Then, the surgeon uses tiny instruments and / or the carbon dioxide laser, to remove or ablate the problem. Both laser and non-laser tools / methodologies are available for every case, but which tools are used depend upon the nature of the problem. There is nothing innately superior about either method; it is the surgeon and not the tools that matter most. Nevertheless, one tends to use instruments for nodules, polyps, cysts, while the laser is more likely to be used for vascular abnormalities or removal of a vocal fold carcinoma.
Then, the surgeon uses tiny instruments and / or the carbon dioxide laser, to remove or ablate the problem. Both laser and non-laser tools / methodologies are available for every case, but which tools are used depend upon the nature of the problem. There is nothing innately superior about either method; it is the surgeon and not the tools that matter most. Nevertheless, one tends to use instruments for nodules, polyps, cysts, while the laser is more likely to be used for vascular abnormalities or removal of a vocal fold carcinoma.
Time required for the procedure is usually short—10 to 45 minutes of operating time.
Potential Risks
Unless you have significant health issues, risks added together are very small indeed. The three main risks include:
- A truly remote possibility of drug reaction, heart problem, etc., during general anesthesia.
- A very small chance of dental trauma—e.g., chipped, scratched, broken, or dislodged tooth. We have a few instances per year of roughened enamel that doesn’t need a dentist’s attention, but only to be smoothed off in the O.R. Beyond this, about once every 3 years something more significant, such as a broken or dislodged crown or tooth happens.
- We cannot guarantee the precise degree of improvement—whether the result will be “good,” “very good,” or “spectacular.” That depends to large degree on the difficulty of the original problem. And when a known tumor is being removed, we may expect possible worsening of voice quality, as compared to “normal.”
Common Questions about Microlaryngoscopy

Surgical Removal of a Mucus Retention Cyst
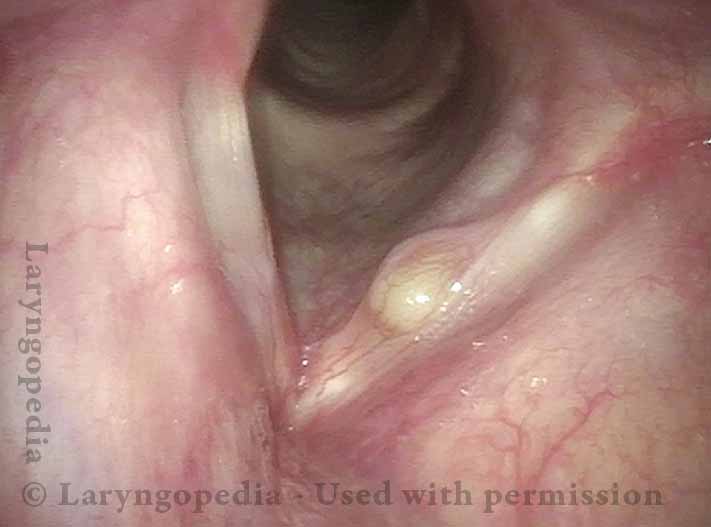
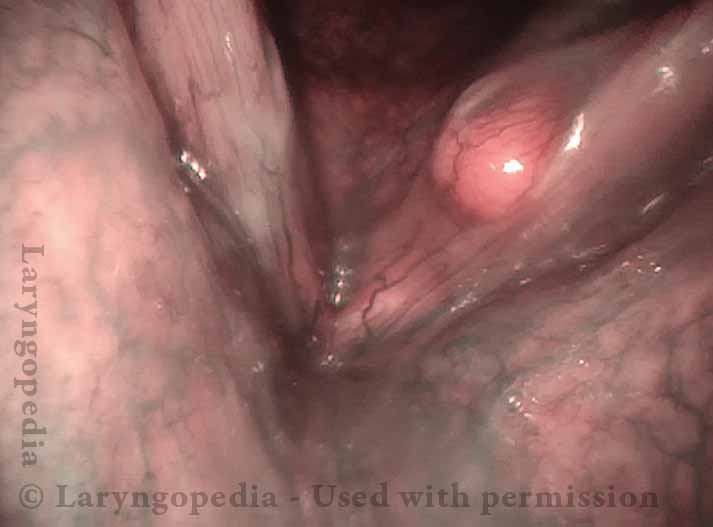
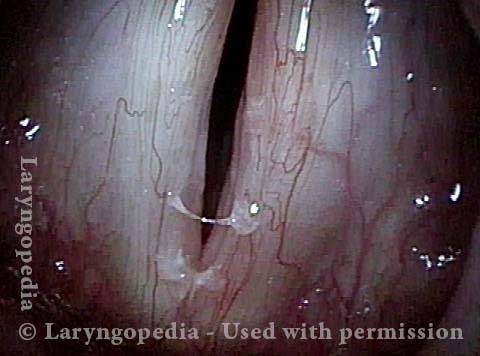
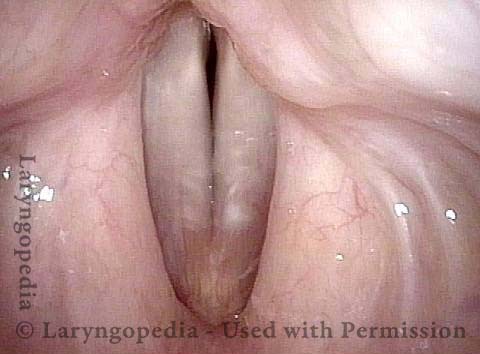
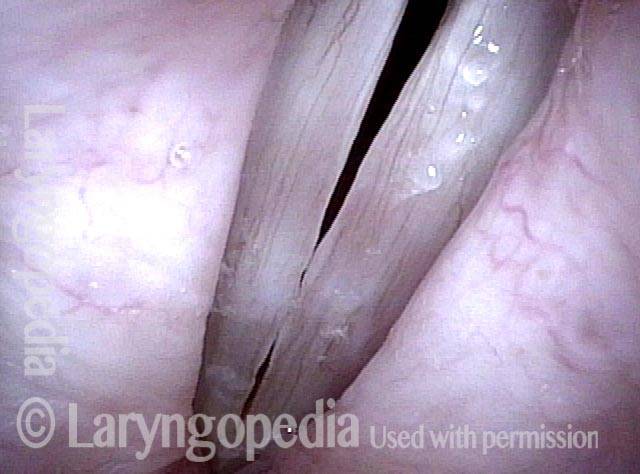
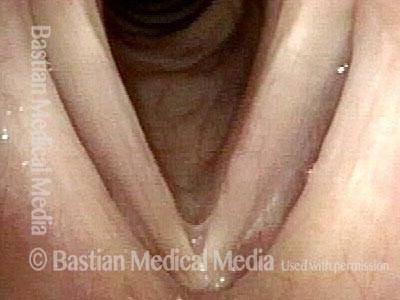
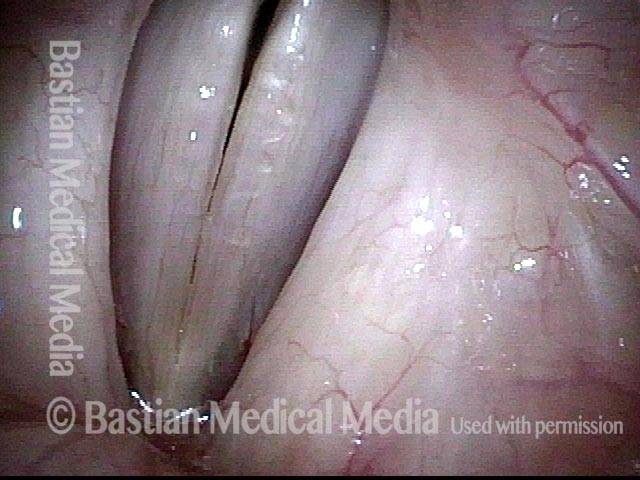
A mucus retention cyst occurs when a small mucus gland becomes plugged and its secretions accumulate, progressively swelling into a cyst. It isn’t known why this happens. There does not seem to be a correlation with vocal overuse, in contrast to vocal nodules, polyps and even epidermoid cysts. Instead, inflammation (viral, or acid reflux-related, for example) seems to be the culprit that plugs the duct of the mucus gland.
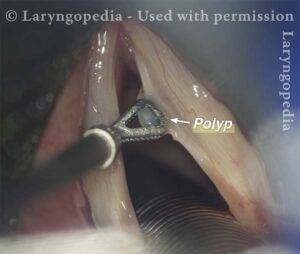
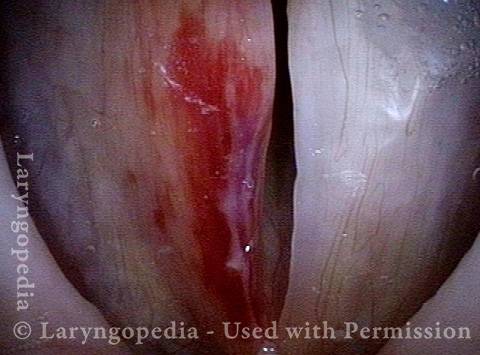
In this long series, an older male public speaker presents with severe hoarseness of many months’ duration. Elsewhere, the swelling of his right cord was described as a polyp, rather than a mucus retention cyst. The only solution is microlaryngoscopy; voice therapy is ineffective for this lesion.
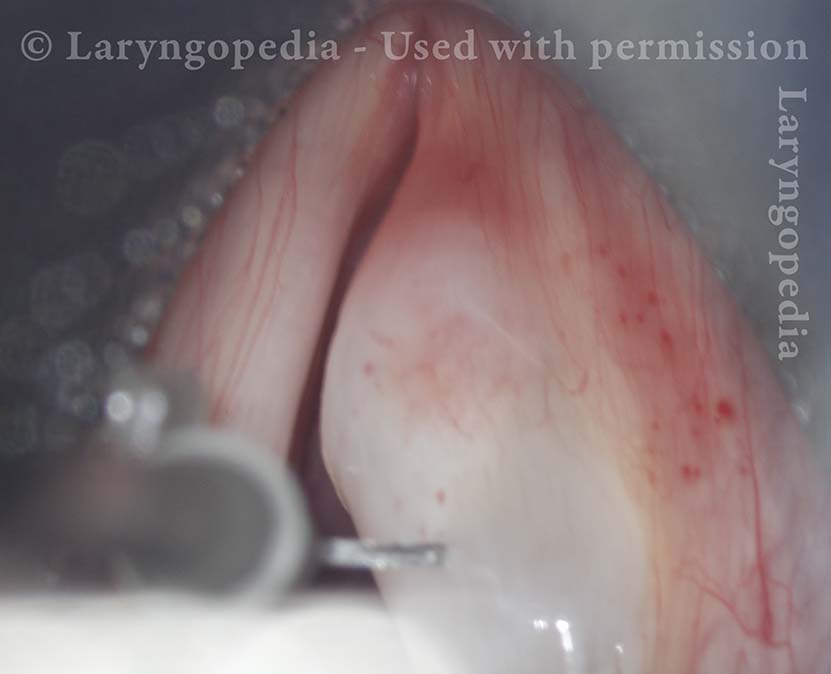
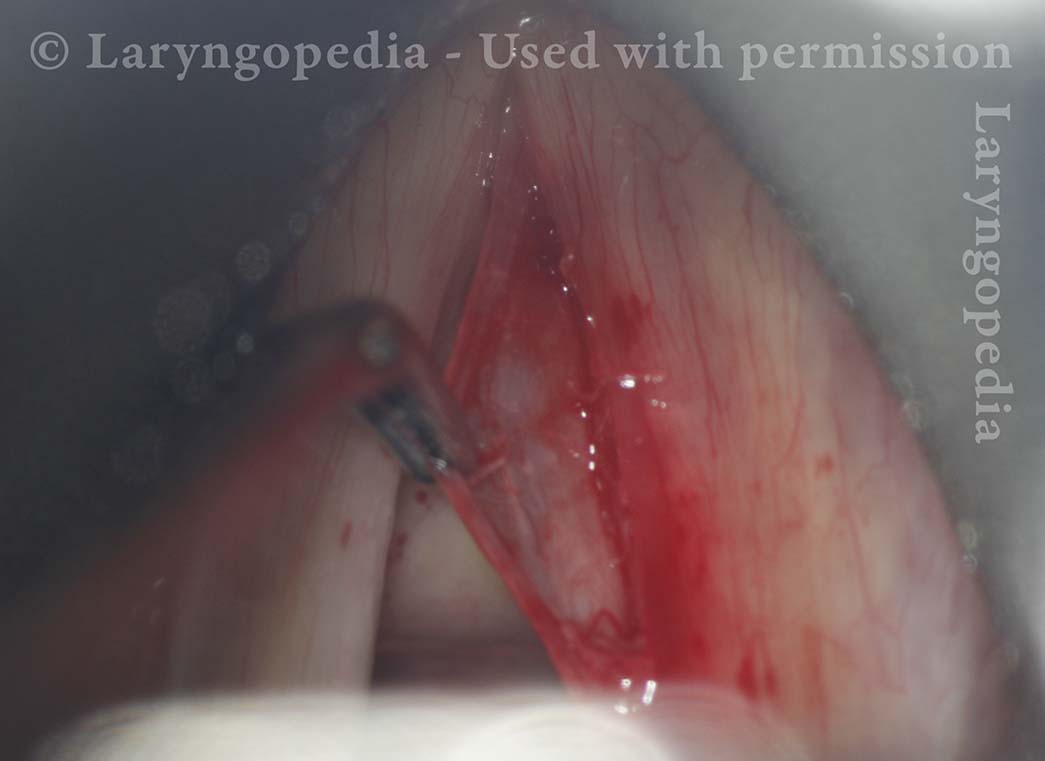
Working with long instruments down a laryngoscope, a very superficial incision is made, the “dragonfly wing” mucosa overlying the cyst is peeled back to expose the cyst. The wall of the cyst itself is also “dragonfly wing” in thickness, making the cyst subject to rupture during removal. Usually if rupture occurs, it is nearing the completion of removal, when most of the dissection has been accomplished and making it possible to remove the entire cyst. In this case, the cyst is delivered intact. Vocal recovery is virtually to normal.
Right vocal cord cyst (1 of 20)
Cyst under strobe illumination (2 of 20)

Cyst margin projection (3 of 20)
Operating view of cyst (4 of 20)

Injecting Lidocaine (5 of 20)
Preparing for Microlaryngoscopy (6 of 20)

Incision of mucosa (7 of 20)

Incision in process (8 of 20)

Dissection of cyst (9 of 20)

Dissection near complete (10 of 20)

Un-ruptured cyst removal! (11 of 20)

7mm intact cyst (12 of 20)

Mucosa flap (13 of 20)
Is the voice affected? (14 of 20)

Voice is much improved! (15 of 20)
Vocal cord vibrates (16 of 20)

Slight bowing (17 of 20)

Equal vibratory blur (18 of 20)

Reasonable closure (19 of 20)

Voice returns to baseline (20 of 20)
Excision of a Mucus Retention Cyst that Decompresses during Dissection
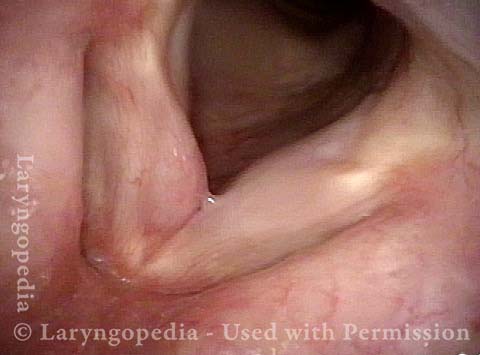
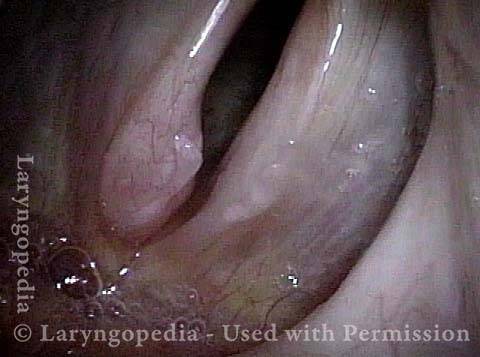
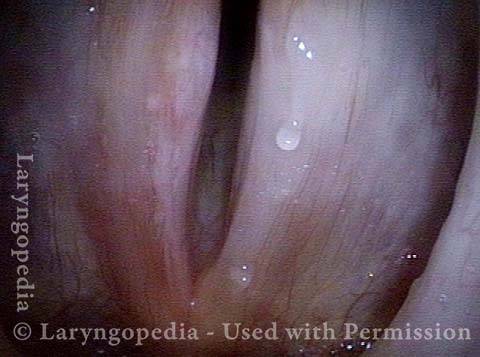
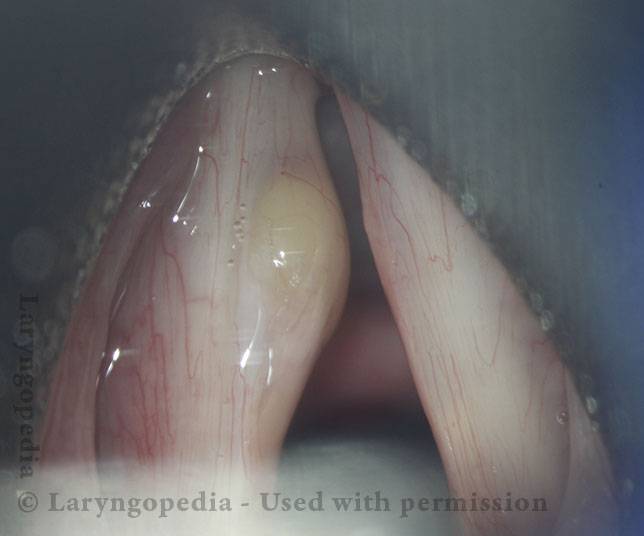
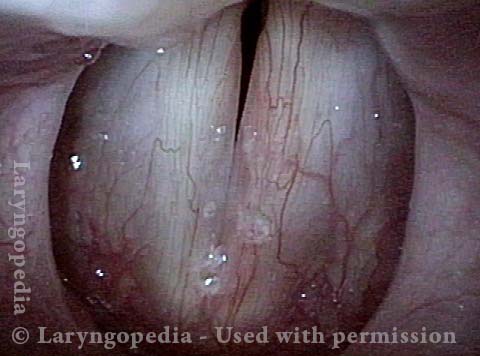
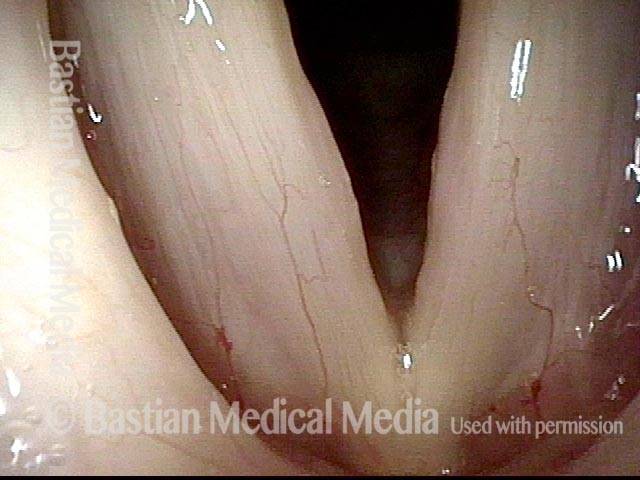
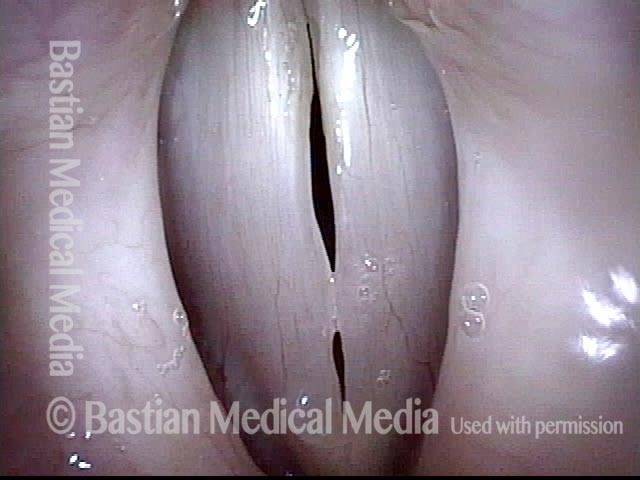
This man has had slight hoarseness for many years, possibly related to his self-described highly talkative and loud-spoken nature. His voice took a significant turn for the worse soon after a bout of mild laryngitis, and had remained extremely hoarse for many months.
An ENT doctor diagnosed a polyp of his left vocal cord. Instead, this represents a mucus retention cyst. Removal provided dramatic return of clear speaking voice. Seen below is preop, intra-operative sequence, and then the result at 3 months after surgery.
Mucus retention cyst (1 of 17)
Closer look (2 of 17)

Cyst under narrow band light (3 of 17)
Cyst interferes with phonation (4 of 17)

Surgical view (5 of 17)

After infiltration (6 of 17)
Lifting the mucosa (7 of 17)

Dissecting cyst from deep attachments (8 of 17)

Cyst has ruptured and emptied (9 of 17)

Dissection of empty sac (10 of 17)

Flaps retract (11 of 17)
Voice is virtually normal at 3 months (12 of 17)

Evidence of vibration, standard light (13 of 17)
Open phase at E3 (14 of 17)
Closed phase at E3 (15 of 17)
Open phase at A4 (16 of 17)

Closed phase at A4 (17 of 17)

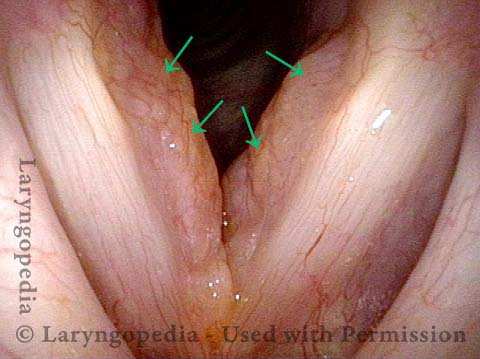
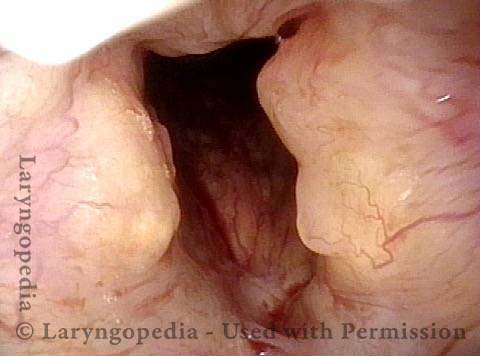
Amyloidosis of the Larynx as Seen Over Time, with Treatment
Primary laryngeal amyloidosis (1 of 7)
Bulky swelling (2 of 7)

Amyloidosis (3 of 7)

Amyloid deposits (4 of 7)
Vocal cords cannot close completely (5 of 7)

Amyloids Remain (6 of 7)

Voice remains clear (7 of 7)
Surgery for Fibrosis, Polyp
Fibrosis + polyp (1 of 4)

Strobe light (2 of 4)

Post microsurgery, open phase (3 of 4)

Post microsurgery, open phase (4 of 4)
Vocal Nodules, Before and After Surgery
Vocal nodules, before surgery (1 of 4)
Before surgery (2 of 4)
After surgery (3 of 4)
Vocal nodules, after surgery (4 of 4)



Vocal Cord Microsurgery in Singers
Dr. Bastian’s original 1996 publication detailing the process for the first time...