Phonatory insufficiency refers to when the vocal cords cannot close sufficiently or vibrate adequately to produce a serviceable voice. An inability to close is usually evidenced by air-wasting phenomenology.
This phonatory insufficiency could have one of several causes. It could be due to the loss of part or all of one or both vocal cords, such as after removal of a vocal cord cancer. Or it could follow prolonged intubation and resulting pressure necrosis of the posterior ends of the vocal cords 1. Another possibility might be scarring of the anterior joint capsule of the cricoarytenoid joints, also as a complication of prolonged endotracheal intubation due to grave illness. Yet another cause might be vocal cord paralysis or paresis. The latter problems not only interfere with the cords’ ability to close, but also make the affected cord flaccid, so that it blows out of the way too easily, further wasting the air stream.
When a person with any of these causes of poor vocal cord closure tries to produce voice, maximum phonation time is typically reduced, because only a fraction of the air pushed up from the lungs is converted to sound, with the remainder of the air quickly “wasted.”
The second main category of phonatory insufficiency, in which the vocal cords cannot vibrate adequately, is seen in a person with stiff or scarred vocal cords. Such a person may not waste air, but just be unable to produce other than a harsh whispery sound, because the stiffened vocal cords (now more like thick leather rather than like, as is normal, plastic wrap overlying a thin layer of jello) cannot vibrate as freely or at all.
Photos:
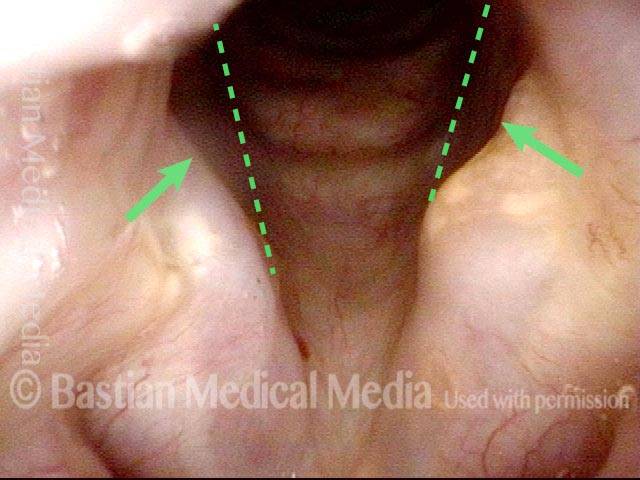
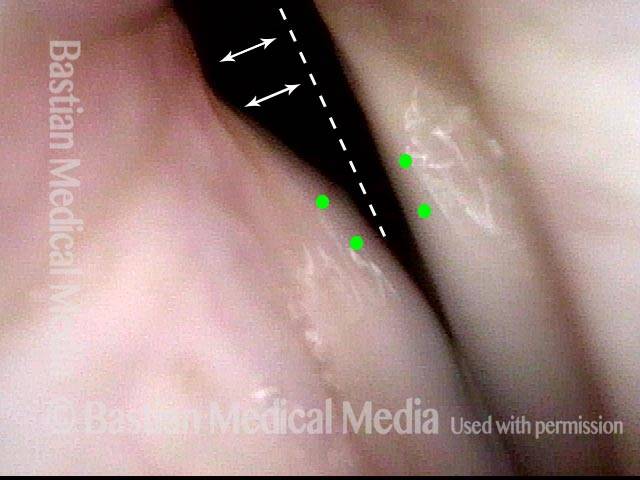
Phonatory insufficiency (1 of 3)
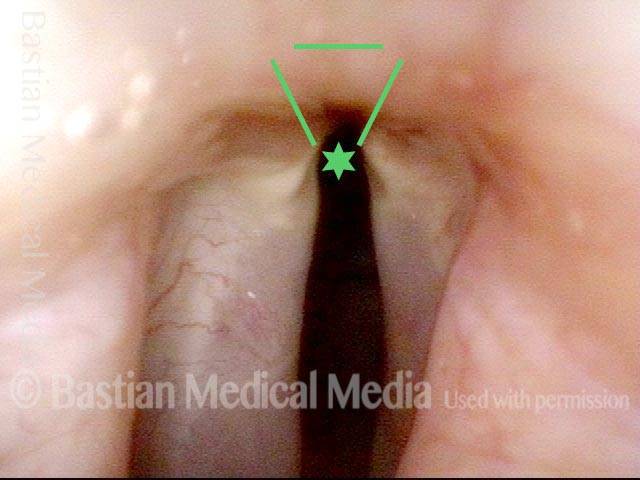
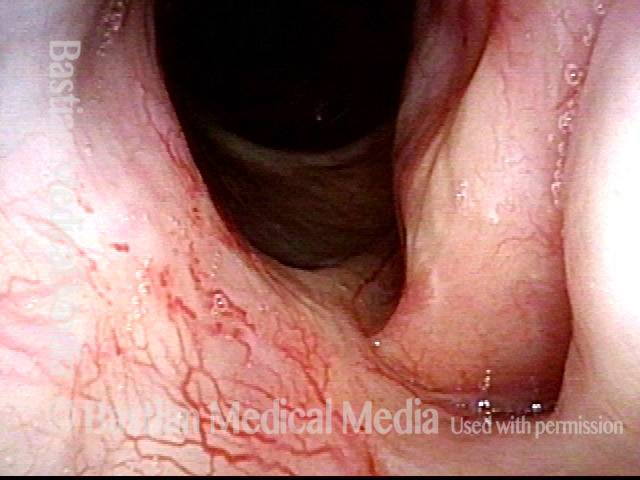
Phonatory insufficiency (2 of 3)

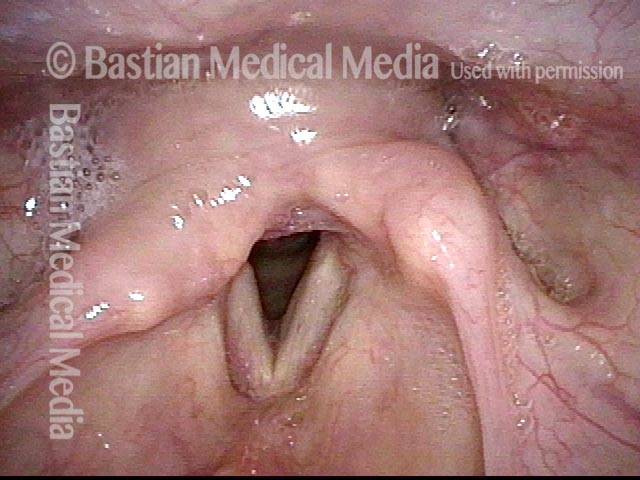
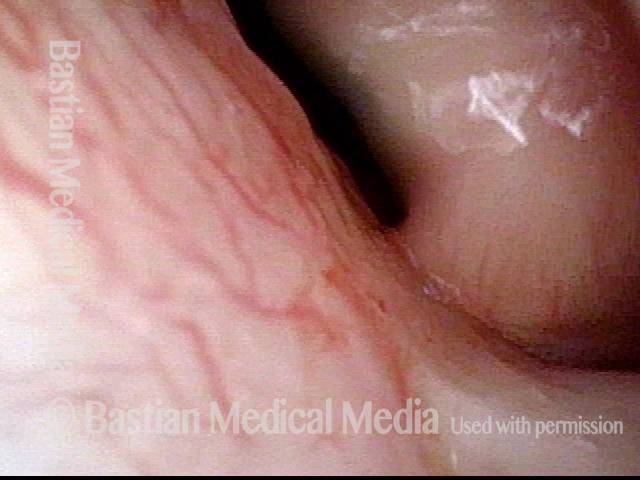
Phonatory insufficiency (3 of 3)
Example 2
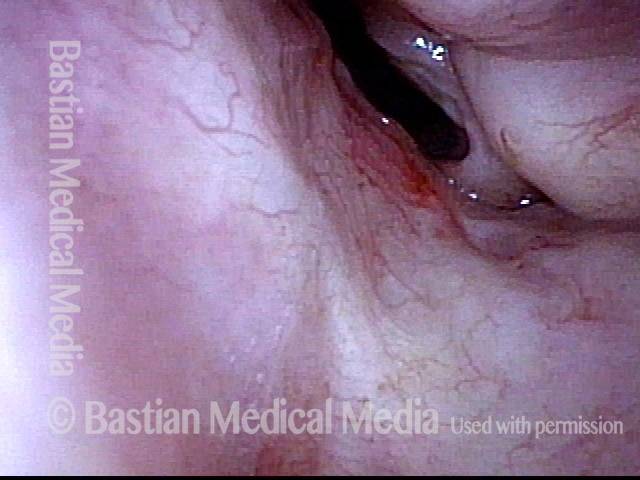
Phonatory insufficiency (1 of 4)
Phonatory insufficiency (2 of 4)
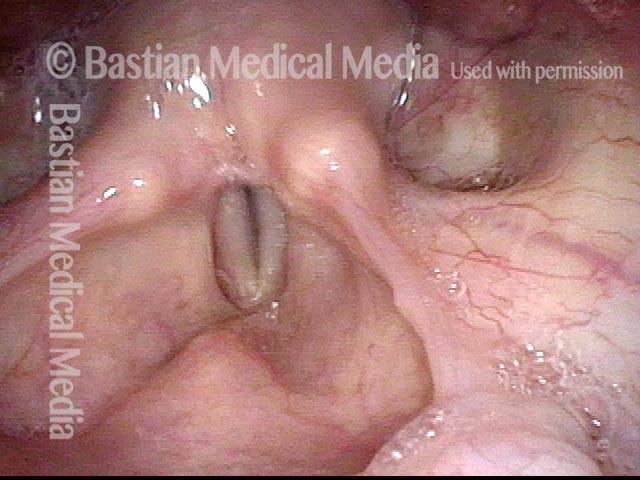
Phonatory insufficiency (3 of 4)

Phonatory insufficiency (4 of 4)
Phonatory Insufficiency Due to Loss of Vibration-capable Tissue
Phonatory insufficiency due to loss of vibration-capable tissue (1 of 4)
Phonatory insufficiency due to loss of vibration-capable tissue (2 of 4)
Phonatory insufficiency due to loss of vibration-capable tissue (3 of 4)

Phonatory insufficiency due to loss of vibration-capable tissue (4 of 4)
- Bastian RW, Richardson BE. Postintubation phonatory insufficiency: an elusive diagnosis. Otolaryngol Head and Neck Surg. 2001; 124(6): 625-33. [↩]