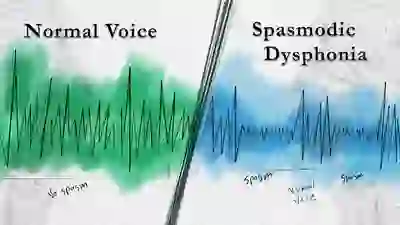
Adductor vs. Abductor SD
There are two main variants of SD. In the first variant, adductor SD (AD-SD), the vocal cords are pressed together excessively, intermittently cutting off words or giving the voice a constant strangled quality; this variant comprises 90% of the cases of SD.
In the second variant, abductor SD (AB-SD), the vocal cords are abruptly and momentarily pulled apart while talking, causing the voice to drop out completely or down to a whispery, breathy sound. There are some cases in which a person has both of these variants: this is called mixed AB-AD SD.
Classic vs. Tonic SD
Another distinction that can be made within adductor and abductor, is between classic variant and tonic variant cases of SD. In classic variant SD, the spasms cause phonatory arrests—that is, while the person is speaking, intermittent words or syllables are choked off (with AD-SD) or drop out (with AB-SD).
In tonic variant SD, the spasms are more continuously sustained, so that the voice continuously sounds either strained (with AD-SD) or breathy (with AB-SD), but without any actual phonatory arrests. Because the presence of phonatory arrests is the symptom most often associated with SD, tonic variant SD goes undiagnosed or misdiagnosed far more frequently than does classic variant SD.
See also: Dystonic Tremor
Treatments for Spasmodic Dysphonia
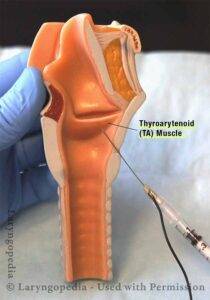
Botox Injections
There is no definitive “cure” for SD, but for most patients, periodic injections of Botox™ into the muscles of the larynx help a great deal, if there is optimal dosage and placement. These injections relax the malfunctioning muscles of the larynx, thereby minimizing the spasms and their impact on the voice.
The effect of an injection typically lasts a few months, and then another injection is needed. For those having difficulty getting good results with Botox™ therapy, see our video below “Spasmodic Dysphonia: When Botox Disappoints.”
What can I expect from Botox injections?
- The initial two or three injections may be needed to establish optimal dose, since there is no way to predict the best dose; instead, these initial injections provide that understanding.
- After each injection, it takes between one and five days, typically, for the Botox effect to be complete.
- If you have AD-SD, we expect transient initial weakness to be a side effect, but your voice should still be functional other than in noisy environments during these initial days. If you have AB-SD, the initial side effect might be mild breathing noises when you exert yourself.
- The golden period of voice quality should last between 8 and 16 weeks on average before another injection is needed. Most people, therefore, receive between 3 and 5 injections per year, and the interval is determined not only by dose, but by individual “biology.”
SLAD-R Surgery
The leading surgical treatment currently offered for SD, Selective Laryngeal Adductor Denervation-Reinnervation (SLAD-R), can be an option for individuals with the AD-SD variant. However, no treatment for SD works satisfactorily for all. The history of each of the several surgical treatments for SD always includes some failures.
Speech Therapy
Speech therapy is another treatment sometimes suggested for SD. While there are strong and even passionate individual proponents of speech therapy, the consensus view is that speech therapy is not expected to substantially improve the voice’s capabilities or reduce spasms other than perhaps in the therapy room1.
A brief course of speech therapy can be very helpful for patient education and perhaps a search for sensory tricks. Much confusion surrounds this subject, because individuals who have a nonorganic voice disorder can be mistakenly diagnosed with SD, and nonorganic voice disorders are routinely “cured” with speech therapy alone.
Frequently Asked Questions

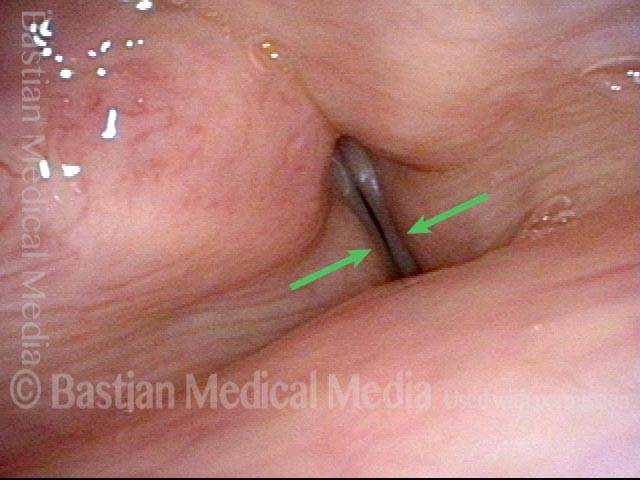
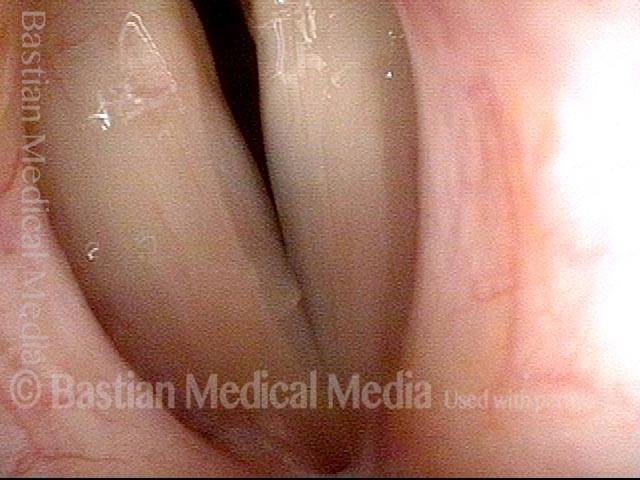
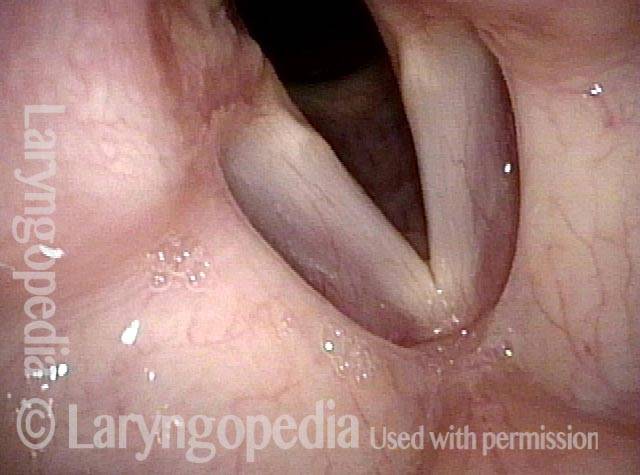
Photo Example of AD-SD
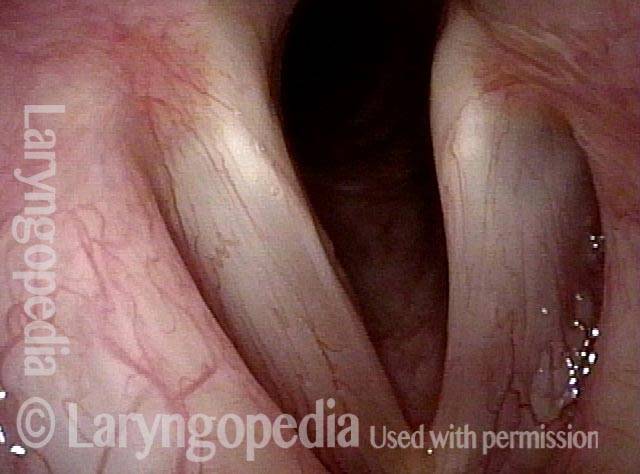
AD-SD (1 of 2)

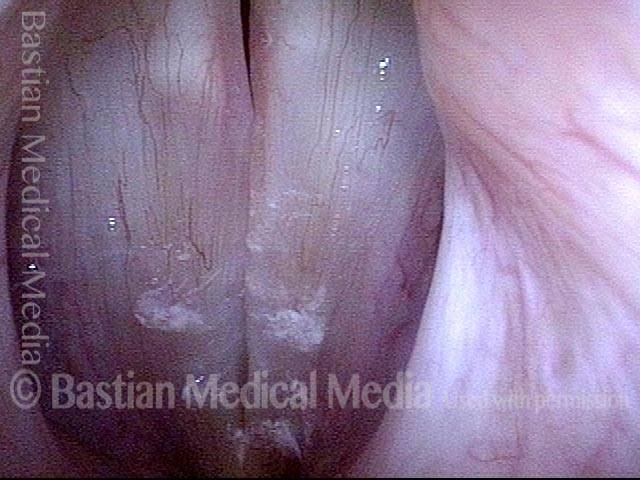
AD-SD (2 of 2)
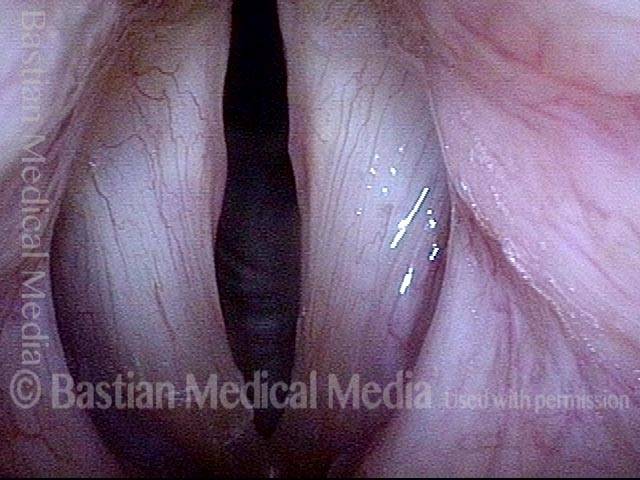
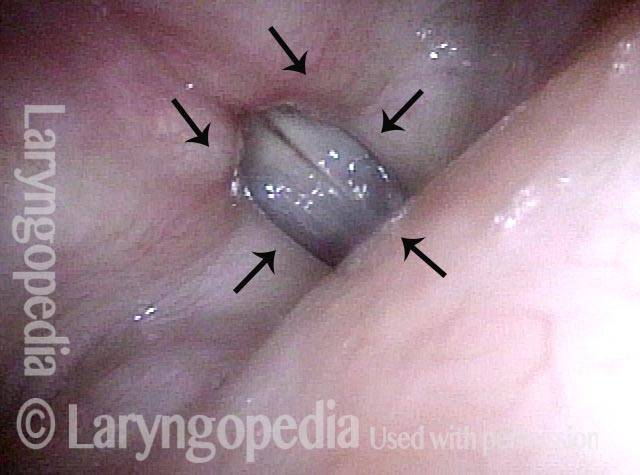
Example 2
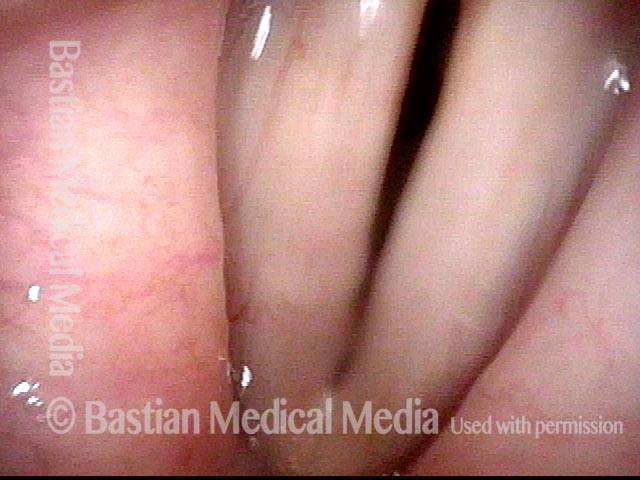
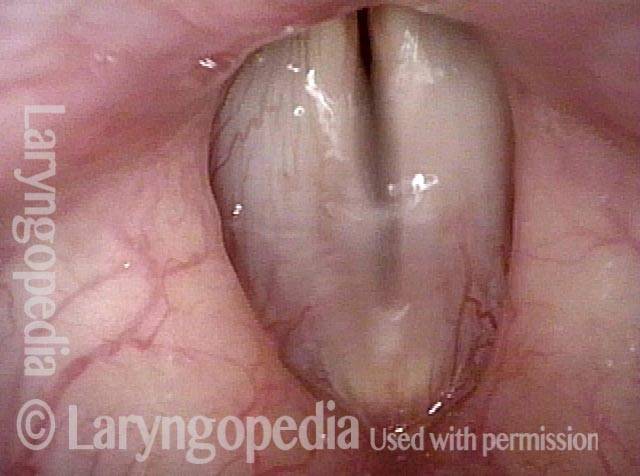
Adductory spasm (1 of 2)
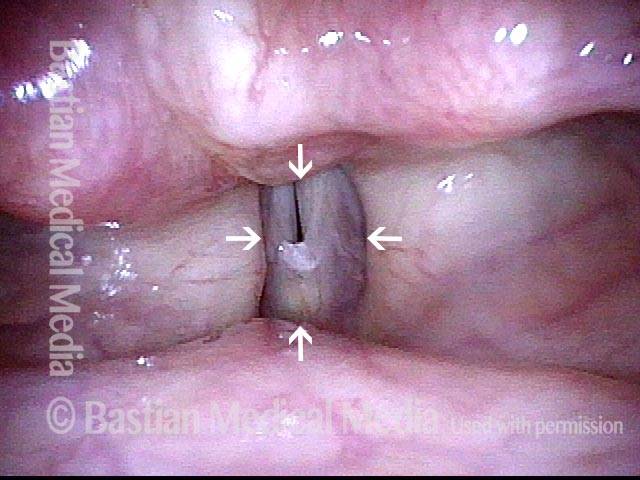
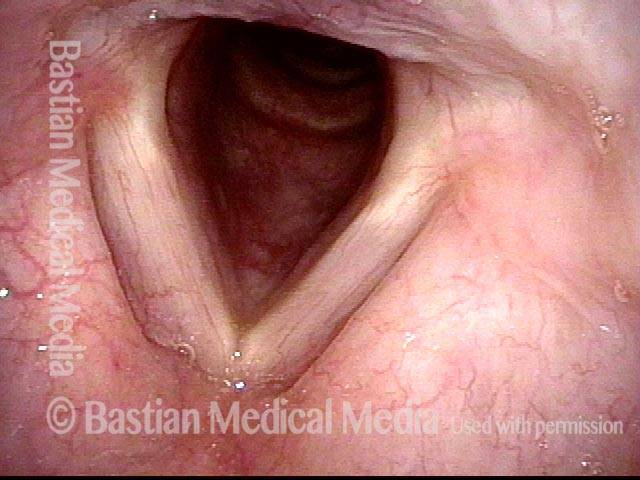
Adductory spasm (2 of 2)

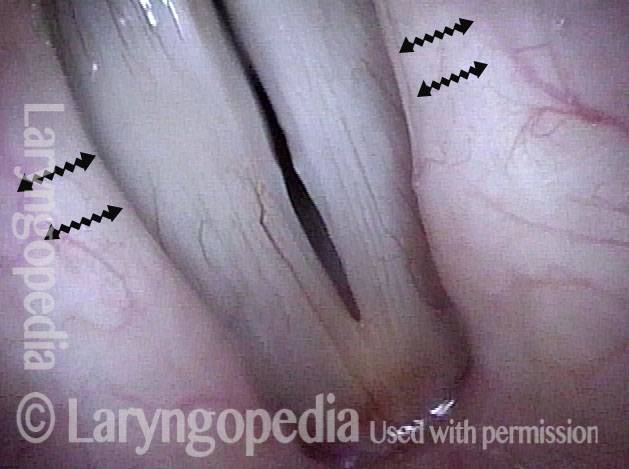
Photo Example of AB-SD
AB-SD (1 of 4)
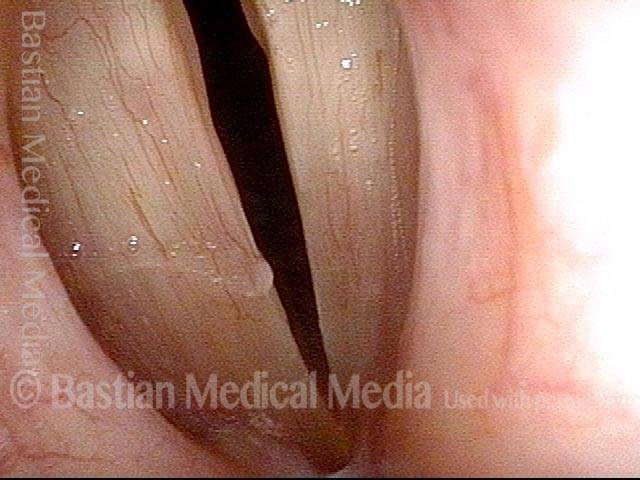
AB-SD (2 of 4)
AB-SD (3 of 4)
AB-SD (4 of 4)
Abductor Spasms, Worsened by Cognitive Loading
Abductor spasmodic dysphonia patient (1 of 4)
Limited abductor spasms (2 of 4)

Increased abductor spasms (3 of 4)
Even greater abductor spasms (4 of 4)

Laryngology 401: PCA-only Paresis, but the Actual Voice Problem Is Spasmodic Dysphonia
Sense of instability (1 of 3)
Vibratory amplitude (2 of 3)
Spasm (3 of 3)
Remarkable Task-Specificity of Spasmodic Dysphonia
Young singer (1 of 4)
Phonation (2 of 4)

Closed phase (3 of 4)

Sudden spasm (4 of 4)
Assessment of Vocal Phenomenology Protects from Visual Red Herrings
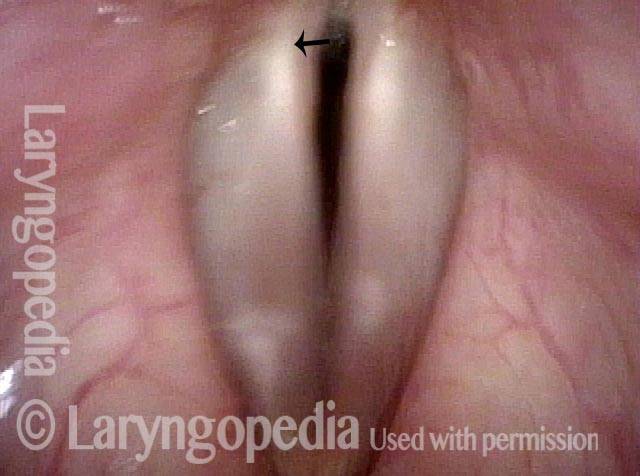
Swelling? (1 of 2)

Spasmodic dysphonia (2 of 2)



- Ludlow CL. Treatment for spasmodic dysphonia: limitations of current approaches. Curr Opin Otolaryngol Head Neck Surg. 2009; 17(3): 160–165. [↩]