{kind=link}
{kind=link}
Tracheal Deformity After Tracheotomy
This man had a grave and life-threatening illness that required mechanical ventilation in an ICU for about 3 months. The initial weeks were through an oro-tracheal tube (a tube placed through the mouth, between the vocal cords, and into the trachea); the remaining 2 ½ months were via a tracheotomy (breathing tube inserted through the base of the neck directly into the trachea).
Now out of hospital for many months, he has a barking cough, and occasionally mild harsh inspiratory noise.
No breathing tube damage on the vocal cords (1 of 5)
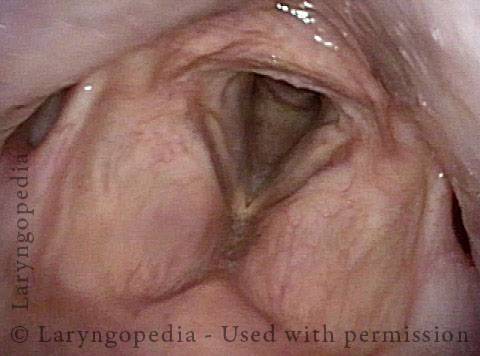
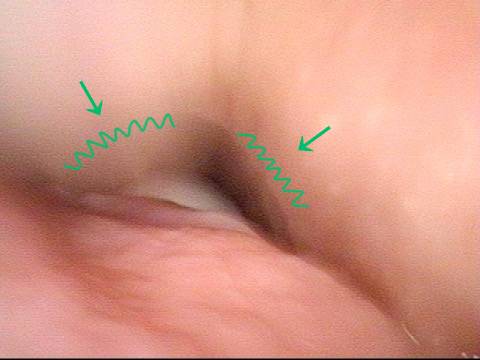
Airway is narrowed below vocal cords (2 of 5)
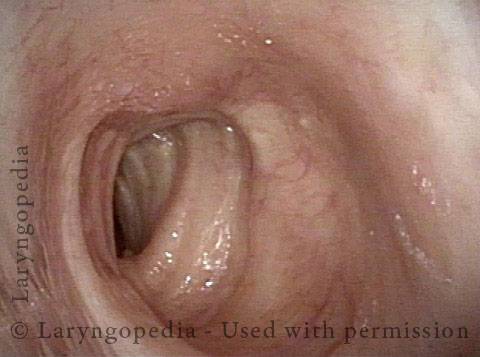
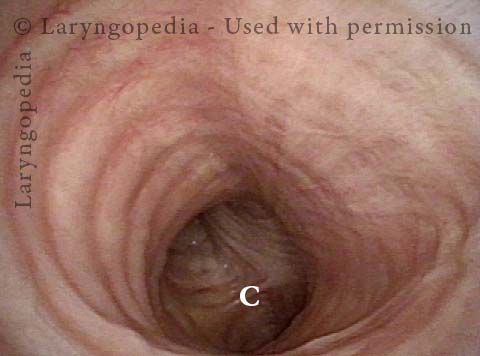
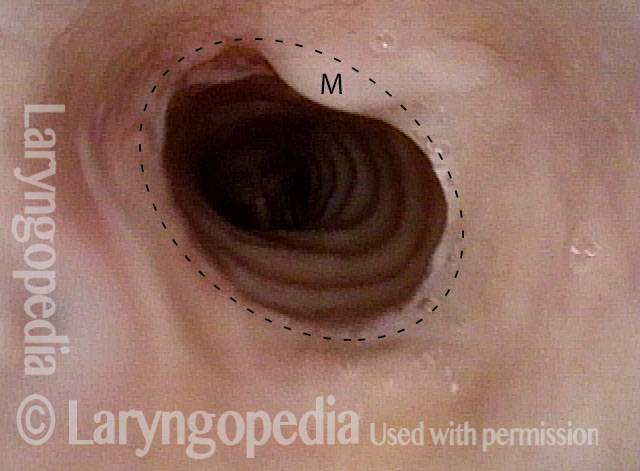
Deformed airway (3 of 5)

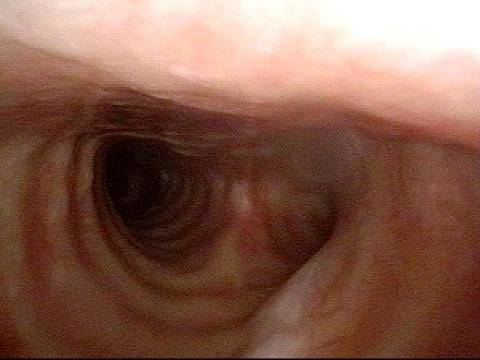
distinctly narrowed but not marginal airway (4 of 5)
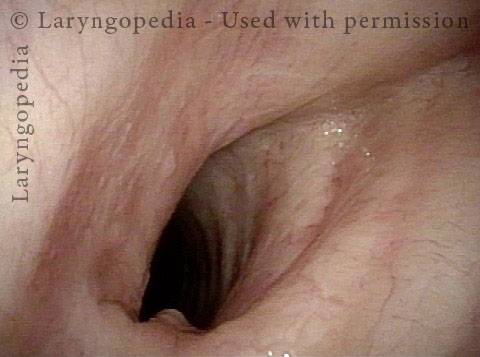
Carina is normal (5 of 5)
Nuances of Endotracheal Tube Injury
This woman with high-risk comorbidities of diabetes and obesity, was in ventilated in ICU more than a month for pulmonary complications of Covid-19 infection. She had an orotracheal tube in place for 3.5 weeks, and then a tracheotomy tube was placed.
Now at her first visit a year later, she remains tracheotomy-dependent, and is told she has bilateral vocal cord paralysis (disproven in the following photo series).
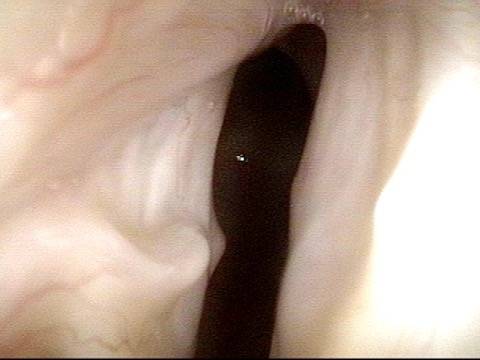
Maximum glottic opening (1 of 8)

Undersurface mucosa indraws (2 of 8)

Phonation (3 of 8)

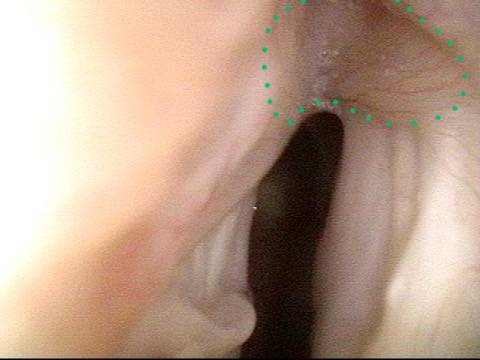
Posterior commissure divot (4 of 8)
Further evidence of scarring (5 of 8)
View into trachea (6 of 8)
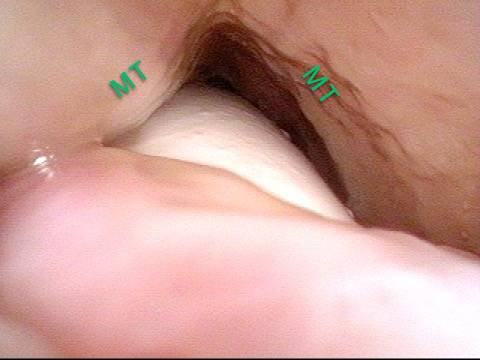
Vibration of trachea (7 of 8)
Open trachea beyond the tube (8 of 8)
The plan here is posterior commissuroplasty, followed by placement of a smaller trach tube and a trial of plugging. If plugging is tolerated during the day, she will need a sleep study with it plugged at night, given the tracheomalacia and her obesity.
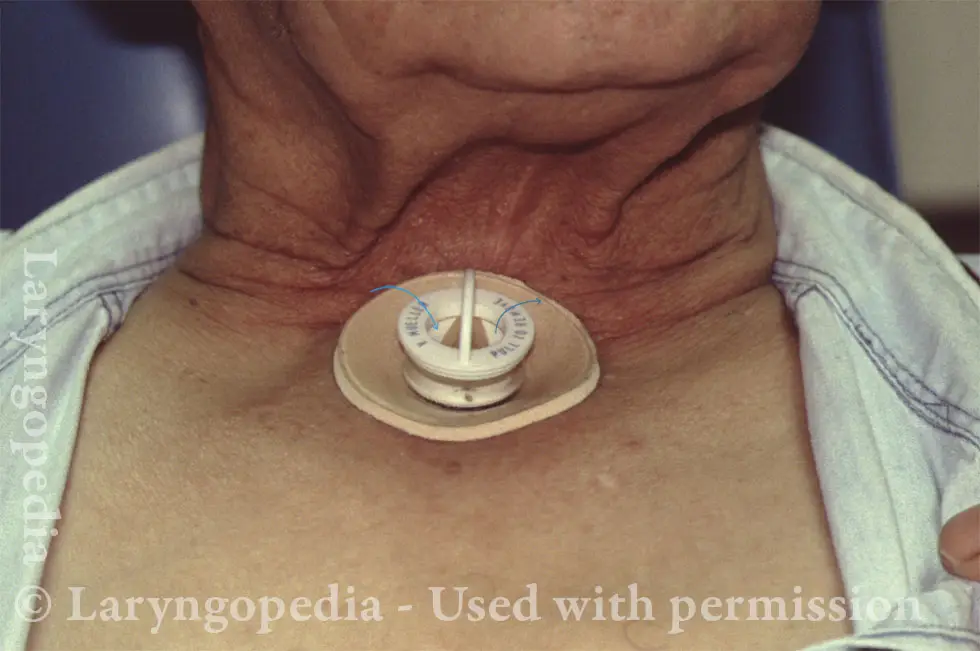
A Fenestrated Tracheotomy Tube allows Voicing when there Is Stenosis
Tracheotomy (1 of 4)

View below vocal cords (2 of 4)
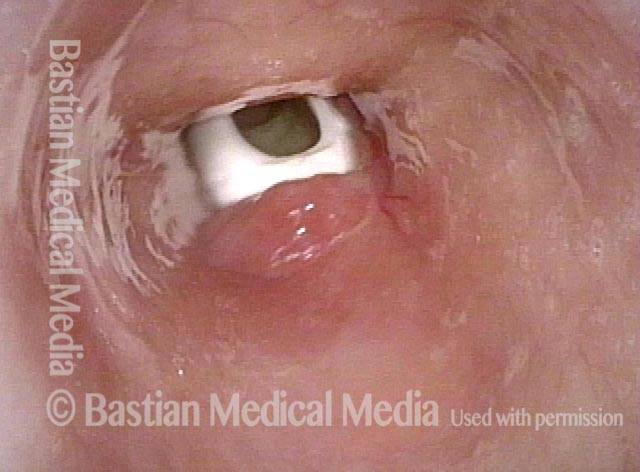
Fenestra (3 of 4)
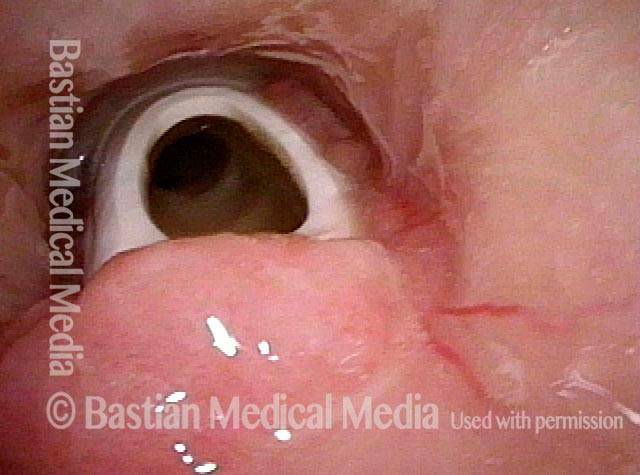
Patient post-trach (4 of 4)
{kind=link}