A Key Visual Finding of Vocal Cord Flaccidity
This seventy-something woman has noted a weak voice for at least a decade. She came for evaluation due to what seemed like further reduction of strength following a bout of laryngitis.
At her evaluation, her faintly fuzzy speaking voice can “pass for normal for age” but when asked to project, her voice manifests a lack of edge and power. At low pitch there is one moment of “luffing.” From her history and vocal phenomenology, vocal cord bowing is suspected.
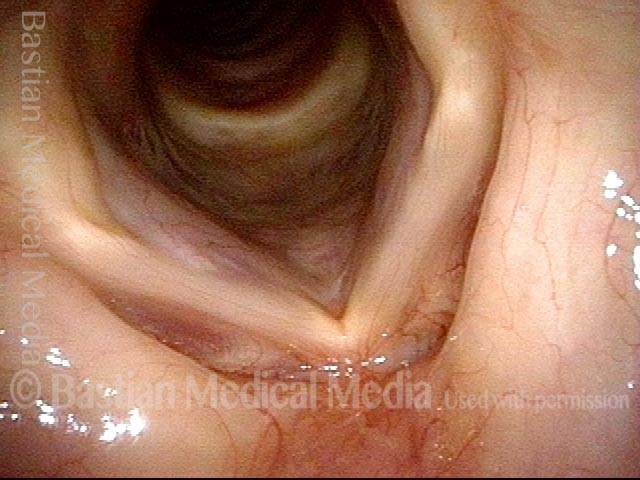
Vocal cords (1 of 4)
Distant view, while breathing. No abnormality is seen.
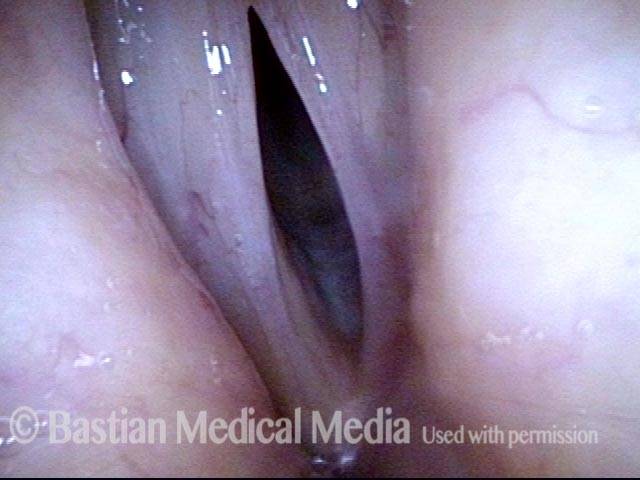
Vocal cords phonating (2 of 4)
Distant view, phonating. Again, nothing unusual is seen.
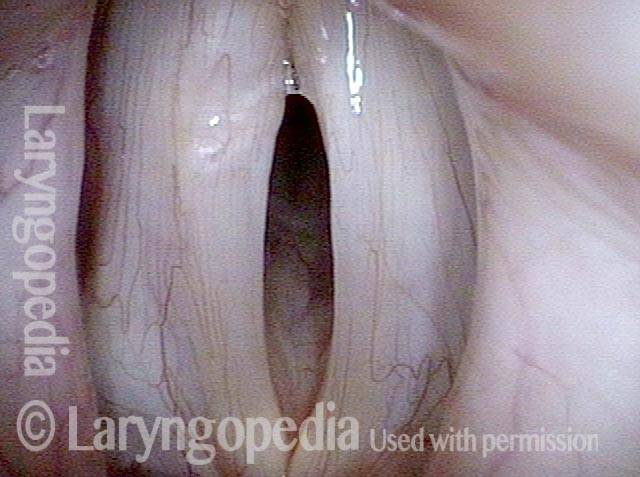
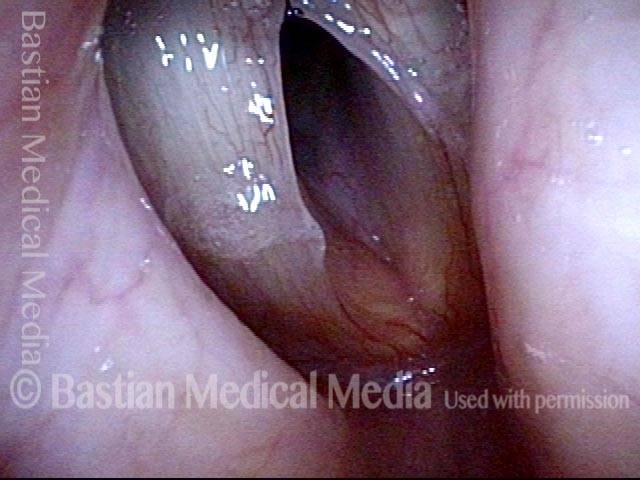
Large amplitude of vibration (3 of 4)
At close range and under strobe light: At estimated A3 (220 Hz), open phase of vibration. An unusually large amplitude of vibration (lateral excursion of the folds) is seen. This is a typical finding suggesting flaccidity.
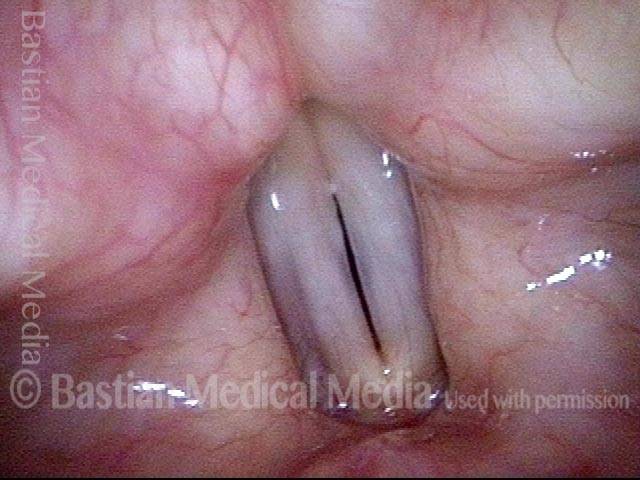
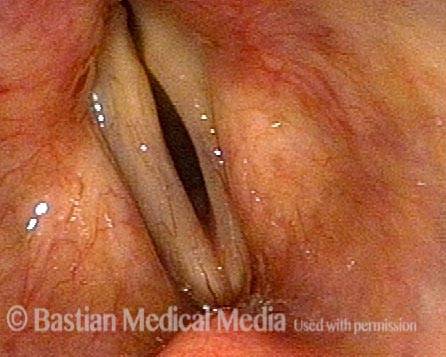
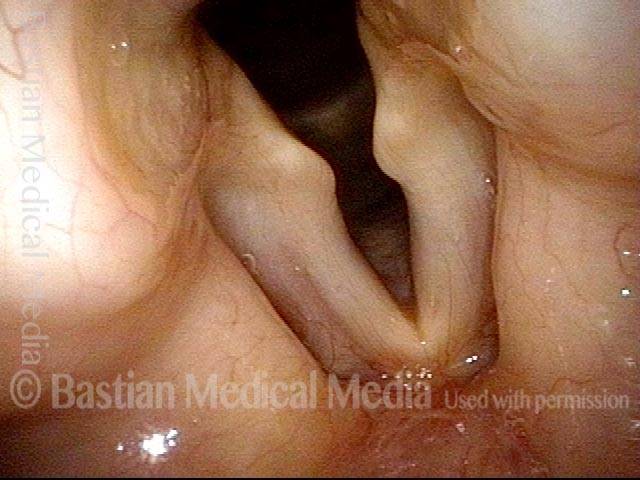
Vocal cord flaccidity (4 of 4)
“Closed phase” of vibration is not fully closed and a highly specific finding of flaccidity is the anterior vocal cords’ failure to close seen here.
Four Views of Vocal Cord Bowing in the Same Person
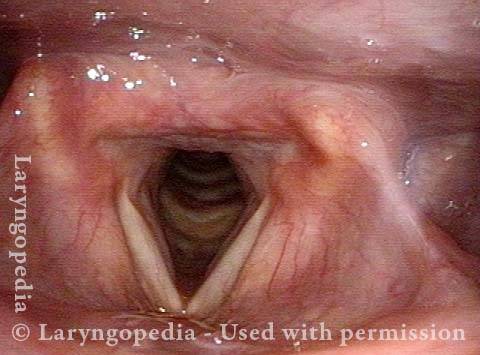
Bowed vocal cords (1 of 8)
An older man has a foggy voice, worsening with use. At medium range in partial abduction, note the bowed vocal cord margins.
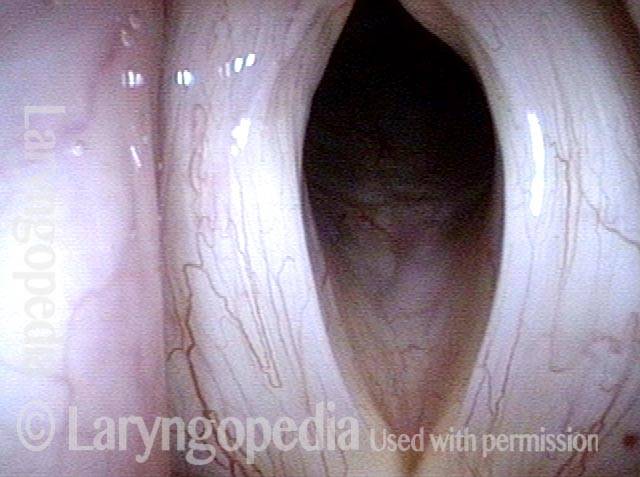
Prephonatory view (2 of 8)
At a greater distance but at the prephonatory instant, there is a large oval gap between the cords.

Open phase (3 of 8)
Now under strobe light, at C3 (131 Hz). The lateral excursions of the cords are huge due to the flaccidity of the cords. Compare with photos 5 and 7.

Gravel voice (4 of 8)
At the same pitch, the closed phase of vibration is not fully closed, and the anterior segment that remains open is often unstable and flutters or vibrates as an independent segment, causing ‘gravel.’

Reduced flaccidity (5 of 8)
The vocal cords must lengthen to produce this higher pitch of F#3 (185 Hz). Lengthening also reduces flaccidity, explaining reduced amplitude (lateral travel) of vibration. Compare with photo 3 and 7.
Closed phase (6 of 8)
The closed phase of vibration, also at F#3, is completely closed, and the voice is more stable at this pitch. Compare with photo 4 and 8.

Falsetto, open phase (7 of 8)
Now at B-flat 5 (932 Hz), the cords are stretched and thinned. Amplitude is quite large, because falsetto tends to de-activate tension within the thyroarytenoid muscles. Compare with photos 3 and 5.

Falsetto, closed phase (8 of 8)
Closed phase of vibration at the same pitch in falsetto is not closed at all for the same reasons described in the caption for photo 7. Compare with photos 4 and 6.

Bowing of Vocal Cords and Effect of Pitch
Weak voice (1 of 8)
This patient has a weak, air-wasting, and gravelly voice. In this distant view, prephonatory instant at a low pitch, D3 (147 Hz), severe bowing can be seen.

Phonatory view (2 of 8)
Also at D3 (147 Hz), but while producing voice. Note that the vibratory blur occurs only in the posterior membranous vocal cord.

“Closed” phase (4 of 8)
At D3 again, now closed phase, which is not closed except posteriorly, explaining the lack of vibratory blur anteriorly in photo 2. Some vibratory cycles are chaotic, too, explaining the gravelly, rough quality of the voice.
B3, open phase (5 of 8)
At B3 (247 Hz), open phase of vibration, the anteroposterior stretch required to produce higher pitch, also somewhat reduces the tissue flaccidity. Vibratory amplitude (lateral excursion) is diminished as well.
D3, open phase (3 of 8)
Under strobe light, open phase of vibration at D3 (147 Hz), note that the amplitude of vibration is enormous, as the air stream easily throws flaccid vocal cords very far laterally.
B3, closed phase (6 of 8)
At B3 again, closed phase of vibration is not really closed, yet is more successful than at the lower pitch in photos 3 and 4. Reduced closure anteriorly is typical for flaccid vocal cords.
Bb4, open phase (7 of 8)
Open phase of vibration at B-flat 4 (466 Hz). Added antero-posterior stretch subtly reduces vibratory amplitude further, especially anteriorly.

Bb4, closed phase (8 of 8)
Closed phase at same pitch as photo 7, is not closed, but the excess lateral amplitude anteriorly is no longer seen.

Red Herring Capillary Ectasia & Mucosal Injuries
Ectatic capillary (1 of 4)
This young performer has a sense of a weakened voice and loss of vocal stamina. Here, we see an ectatic capillary of the left vocal cord (right of photo). Is the problem intermittent vocal hemorrhage from this vulnerable capillary? Is there increased susceptibility to edema due to this margin capillary?
Ectatic capillary, narrow band light (2 of 4)
Under narrow band light, the capillary is even more evident. The additional network of prominent capillaries prompt the same questions as in caption 1.

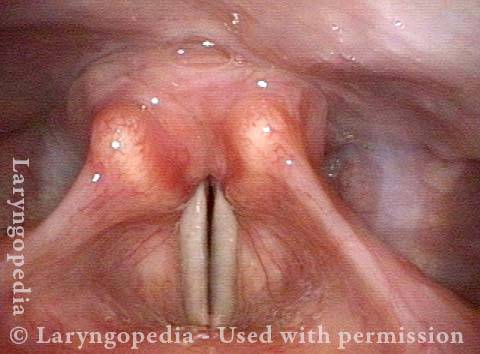
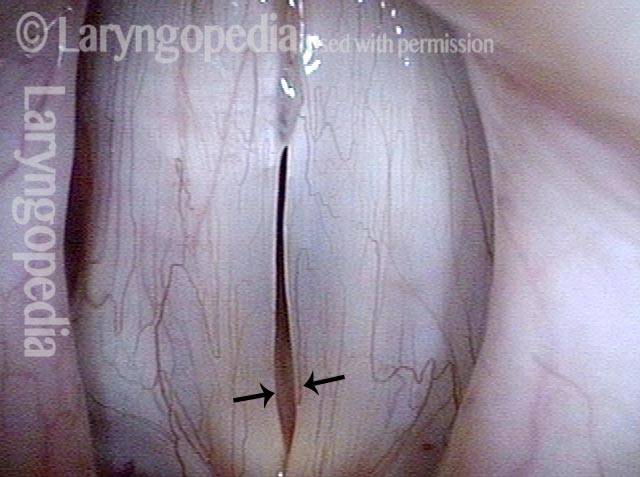
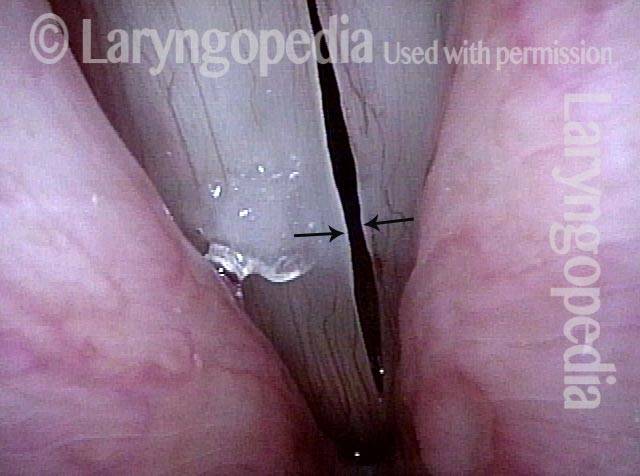
Margin swelling (3 of 4)
Under strobe light at B-flat 4 (494 Hz), we see subtle margin swelling (arrows), here of only “indicator lesion” magnitude.
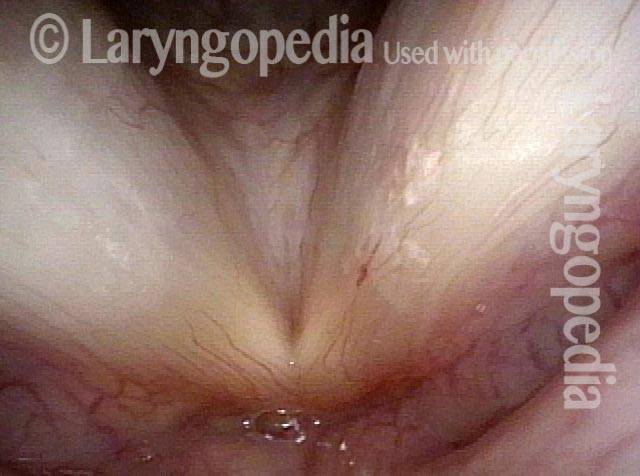
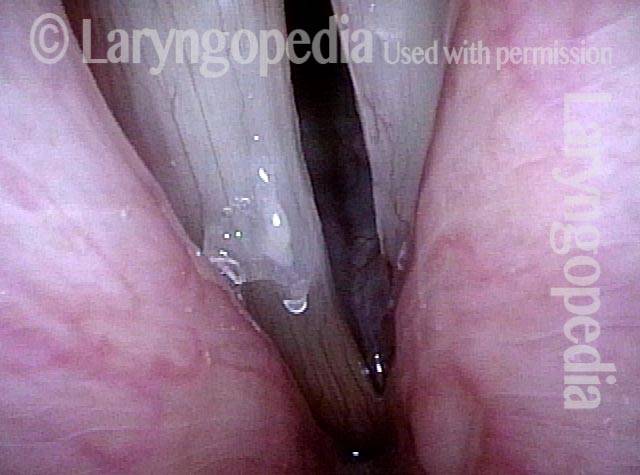
Bowing, atrophy, and flaccidity (4 of 4)
The large amplitude of the open phase of vibration at the same pitch, along with the lack of closure in photo 3, reveals the actual problem to be bowing, atrophy, and flaccidity. These findings fit with the “bowing” symptom complex: loss of edge to voice quality and the tendency of voice quality and strength to “fade” as the day progresses.
Glottic Furrow—Not Just Bowing and Not Glottic Sulcus
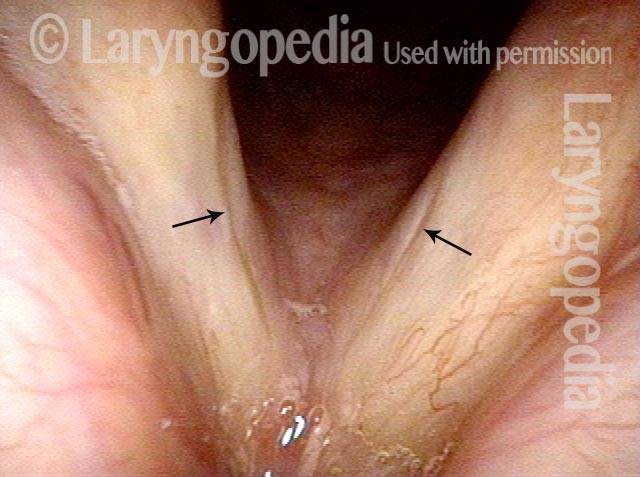
Bowing vocal cords with furrows (1 of 4)
This middle-aged man’s voice has become increasingly husky and weak across many years. In retrospect, it was never a “strong” voice. The cords are bowed, and the furrows seen here (arrows) become more visible in subsequent photos.
Closed phase (2 of 4)
Under strobe light at B-flat 2 (117 Hz), this is the “closed” phase of vibration, perhaps better defined in this instance as the “most closed” phase.

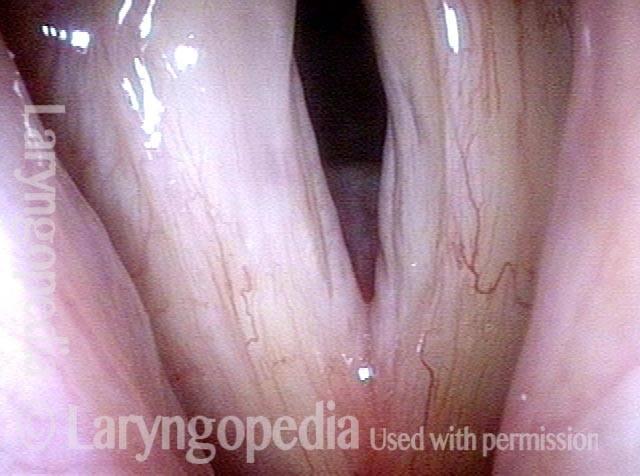
Open phase (3 of 4)
The open phase at the same pitch, shows a linear groove just below the margin of each cord. Some might call these glottic sulci, but “furrow” would be the better definition, as seen in the next photo.
Lower pitch reveals furrow (4 of 4)
At lower pitch, the amplitude of vibration is larger and the right cord (left of photo) reveals more clearly that the the linear depression is a wide furrow, not a slit-like sulcus.

More Photo Examples
No items were found matching your selection.
Example 2
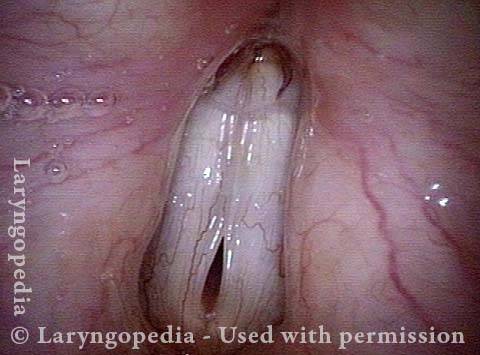
Glottic gap (1 of 3)
Vocal cords at the prephonatory instant under standard light. Note the highly bowed glottic gap.

Vibratory blur (2 of 3)
After vibration begins. Note the very wide “vibratory blur,” consistent with bowing under standard light.

Wide lateral excursion (3 of 3)
Open phase of vibration under strobe light, showing unusually wide lateral excursions of the cords resulting from their flaccidity.
Example 3
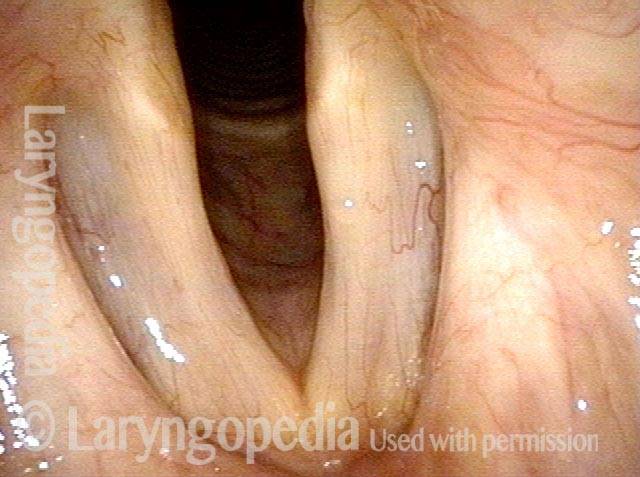
Vocal cord bowing (1 of 2)
Vocal cord bowing, at the prephonatory instant.
Vocal cord bowing (2 of 2)
Immediately after phonation, showing better closure, but only due to vibratory blur.

Example 4
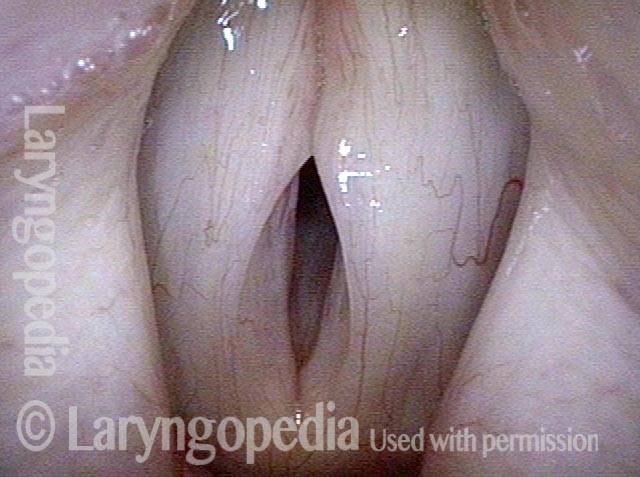
Vocal cord bowing (1 of 4)
Bowing of vocal cords as seen under continuous light, at prephonatory instant, just before vibratory blur.

Vocal cord bowing (2 of 4)
Under strobe illumination, at maximum open phase (greatest lateral excursion).
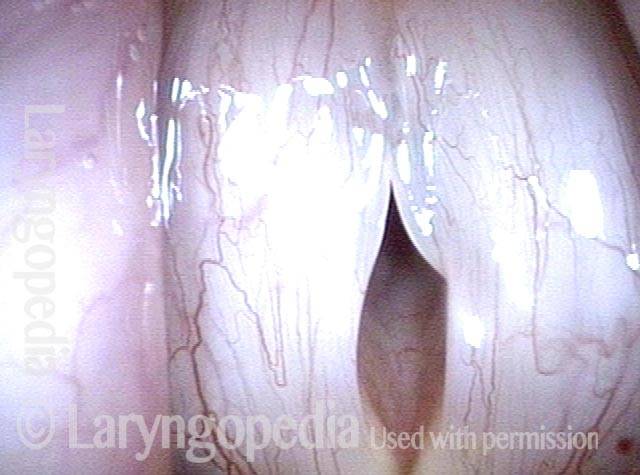
Cords do not close (3 of 4)
Maximum “closed” phase of vibration, which is not fully closed; greatest medial vibratory excursion does not bring the cords into full contact.

Vocal cords only come in near contact (4 of 4)
Due to vocal weakness, when effort is increased the false cords come into near contact, and can even add a rough second sound to the voice.

Example 5
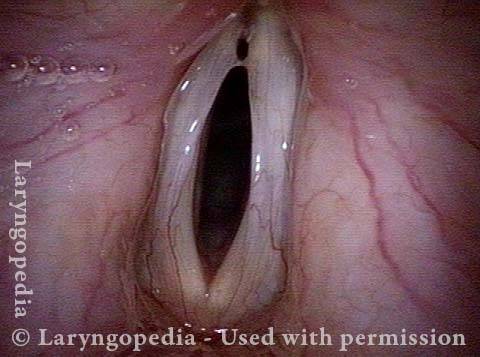
Oval gap during prephonatory instant (1 of 4)
Prephonatory instant shows an oval gap between the cords, rather than a thin line.

Vocal cord bowing (2 of 4)
Bowing, as seen in abducted, breathing position.

Anterior flaccidity (3 of 4)
Strobe light, maximum closed phase, with poor closure especially anteriorly. The greater flaccidity anteriorly may cause an independent vibratory segment and chaotic vibration with rough, gravelly quality.

Vocal cord bowing (4 of 4)
Strobe light, maximum open phase of vibration.

Example 6
Vocal cord bowing (1 of 5)
Bowed vocal cords, abducted breathing position.
Musculomembranous are bowing (2 of 5)
As the cords begin to adduct, medial turning of vocal processes accentuates the bowing of the musculomembranous (anterior 2/3) of the vocal cords.
Elliptical gap (3 of 5)
The prephonatory instant under continuous illumination, showing bowed free margins and an elliptical gap rather than the straight-line match of more normal vocal cords.

Vocal cord bowing (4 of 5)
Under strobe illumination, open phase of vibration.

Vocal cord bowing (5 of 5)
Under strobe illumination, closed phase of vibration. The closure here isn’t complete because the cords’ return to midline is flaccid.