Introduction
Patients who are diagnosed with early vocal cord cancer have two main treatment options to consider: laser surgery or radiation. There are quite a few factors to consider when weighing these two options, which can be confusing for the patient and challenging for the clinician to explain.
After 15 years of laryngology practice, I decided to create a single, codified overview on this subject, to help me teach more clearly and comprehensively when consulting with patients about this decision. Since creating that overview (which I also send home with patients as a handout), I’ve found it much easier to explain to patients the factors to consider when deciding between laser surgery and radiation to treat early vocal cord cancer. Below is that overview I created, in case it could help others who are consulting on or making this decision.
Background
Vocal cord cancer is classified according to size, location, and whether or not there is spread beyond the larynx. To simplify, the classification system for the primary tumor (site of origin) is:
- T1—very superficial, with normal mobility of the vocal cord
- T2—tumor has spread a little deeper and wider and this reduces movement of the vocal cord
- T3—the tumor replaces much of the vocal cord, and the vocal cord is fixed (immobile)
- T4—the vocal cord is not only fixed, but there is evidence of cartilage framework (voice box) invasion
This article focuses on the early vocal cord cancers, T1 and T2. The vocal cord is fairly “isolated” immunologically, so spread to lymph nodes, or to distant organs, is rare with early tumors, and the “N” (nodal) and “M” (distant metastasis) status will therefore not be included in this discussion.
The cell type of cancer in this location is virtually always squamous cell carcinoma. An alternate term, epidermoid carcinoma, is used interchangeably. These terms signify that the tumor originates from the mucosa, or surface layer of the vocal cord. The most common cause of this tumor is tobacco use. Another known cause is HPV (human papillomavirus) infection. Though controversial, some believe that chronic acid reflux from stomach up the esophagus and into the throat—outside of conscious awareness, during sleep—can be a cause as well.
Diagnosis and Workup
An extremely clear view of the tumor in a videoendoscopy room (after general head and neck examination) is usually sufficient to classify the primary tumor (see above). Given that spread outside the larynx is so rare, we in our laryngology practice do not routinely do CT or other scanning for a T1 and even T2 lesion (radiation doctors virtually always do). Biopsy to prove the diagnosis is accomplished either in the videoendoscopy procedure room using topical anesthesia, or in the operating room under general anesthesia.
Treating Cancer in General
The theoretical options for the treatment of cancer include chemotherapy, radiation therapy, and surgery. The obvious general principle when treating cancer of any organ is to match best treatment to each cancer, according to its type and whether it is early or advanced.
For example, leukemia is cancer of the blood cell-forming elements in bone marrow, but the cancerous cells circulate throughout the bloodstream as well. For this reason, neither surgery (a local and regional treatment) nor radiation (also a local and regional treatment) plays a significant role as compared with chemotherapy, which also circulates in the blood and therefore treats the entire body.
Note that some tumors are treated with a combination of surgery + radiation, or chemotherapy + radiation, etc.
Treatment of Early Vocal Cord Cancer
For early squamous cell carcinoma of the vocal cords, specifically T1 and T2 tumors, we use single modality treatment (i.e., only one mode of treatment is used rather than two or three in combination). There are two perfectly valid modes of treatment which are highly competitive options: endoscopic laser surgery, accomplished through the mouth during general anesthesia, or radiation therapy . A table highlighting each treatment mode’s “points of competition” for early vocal cord cancer—that is, the pros and cons of each—is presented below.
Modes of Treatment for Early Vocal Cord Cancer
| Point of Competition | Radiation | Laser Surgery |
|---|
1. Cure Rate with Initial Single-Modality Treatment
(Failure of first treatment does not imply that the tumor will win, but only that you will need a second treatment modality.) | Approximately 85% “cure.” The remaining 15% need more treatment. See also #7 below. | Approximately 85% “cure.” The remaining 15% need more treatment. See also #7 below. |
| 2. Convenience | Approximately 30 visits to the radiation therapy facility | One outpatient surgical procedure under general anesthesia, or, uncommonly, two |
| 3. Early Side Effects | Little to none for two weeks, then skin of neck goes from pink to red to somewhat tanned; the inside of the throat becomes sore. There may be a period of radiation laryngitis lasting a month or so, as well as a sore throat when swallowing. You may lose some weight due to swallowing discomfort. | Sore throat from the laser surgery, typically for a few days following the procedure. Voice may be quite weak for a few weeks until healing is established. Approximately one in ten patients develop exuberant “proud flesh” healing response, which delays voice recovery, but does not change final result. |
| 4. Later Untoward Consequences, Potentially Permanent | 1) Persistent throat dryness. 2) A rare progressive fibrosis—what we call a “leatherization” process that makes tissues stiff, and voice progressively harder to produce, usually starting several years after radiotherapy was completed. 3) A rare stenosis where raw surfaces—either vocal cords, or upper esophagus—stick together, causing poor voice or swallowing difficulty. May be treated successfully, however. 4) A radiation-induced malignancy called sarcoma. It occurs rarely, many years after treatment is complete. | None, other than (for some, not all) persistent huskiness that is usually less than that caused by the tumor itself. |
| 5. Cost | An estimated five times the cost of surgery | An estimated one-fifth the cost of radiation |
| 6. Voice Result | Usually quite good after recovery from radiotherapy. Most voices a little deeper in pitch, and “drier.” | After healing, the typical voice result rivals that achieved with radiotherapy, provided not more than one-third of the bulk of the cord is removed. In those with larger resections, an implant can be placed to improve voice. |
| 7. Implications of Treatment Failure | Since radiation therapy cannot be repeated, the second treatment is necessarily some form of surgery: endoscopic laser or partial laryngectomy, or, rarely, even total laryngectomy. | All surgery options, including a second laser excision, remain. So does radiation therapy. |
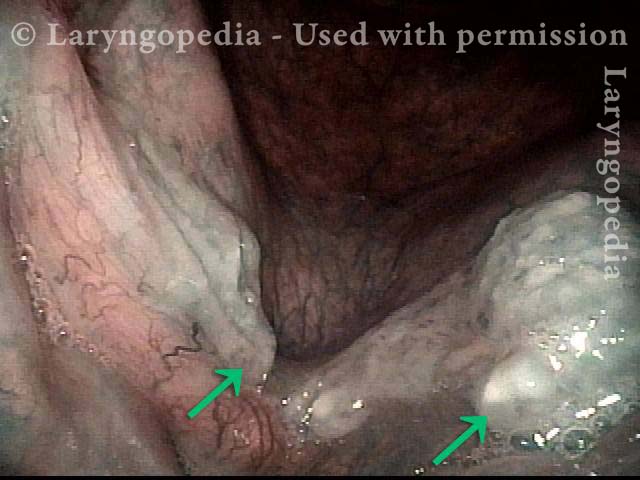
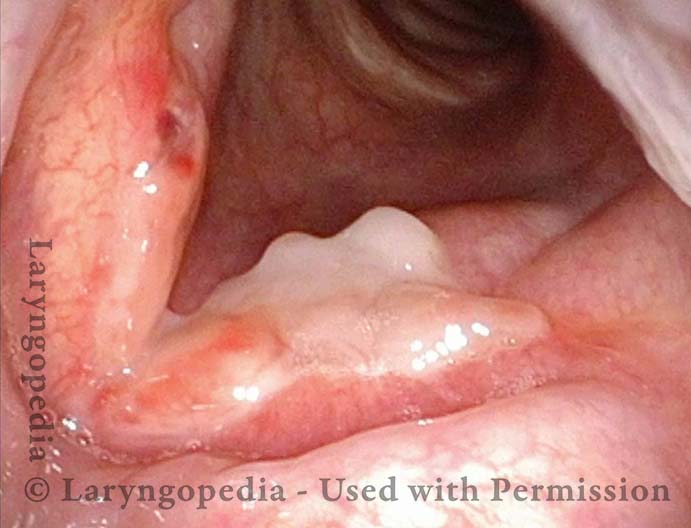
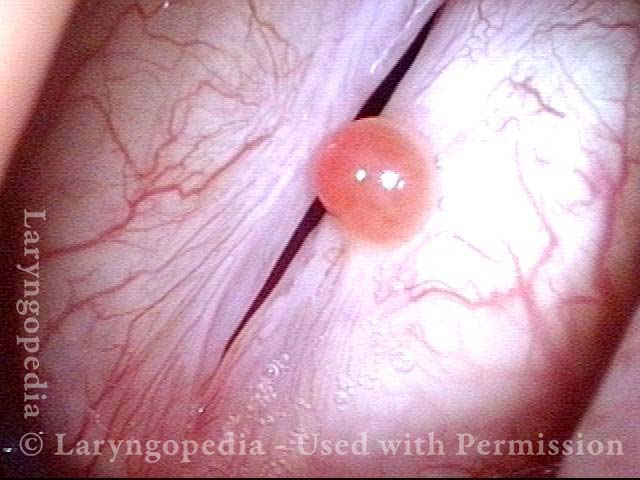
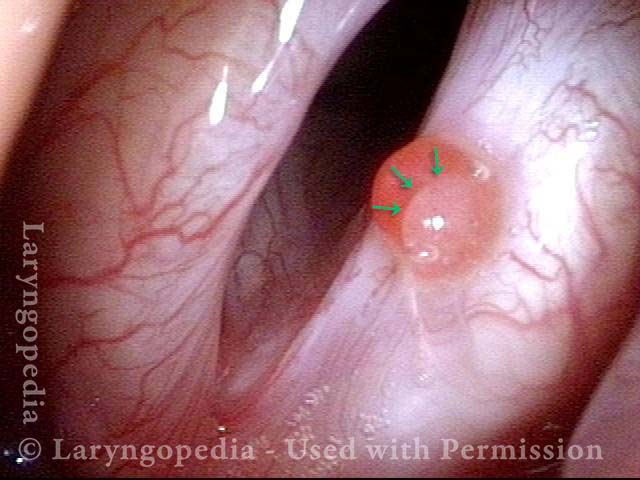
Before and After Images of Surgical Treatment







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
 Early Vocal Cord Cancer Overview
Early Vocal Cord Cancer Overview