Mucosal Indrawing with Inspiration
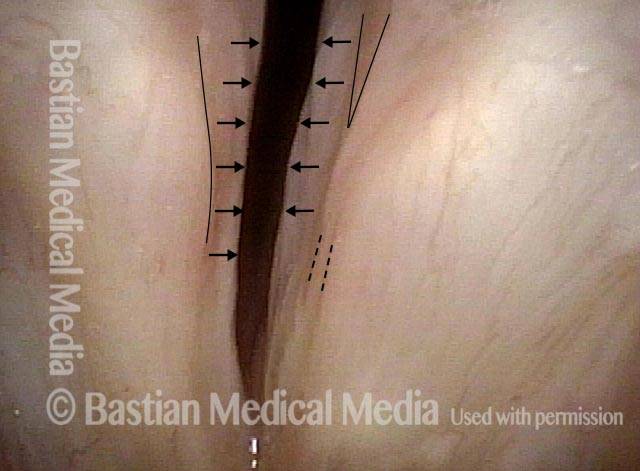
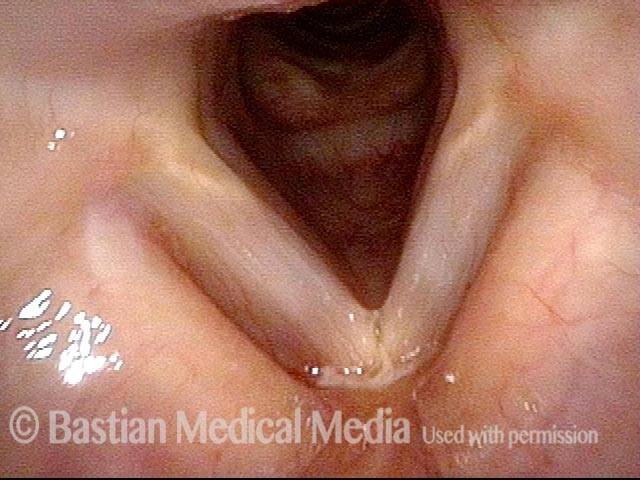
Paralyzed vocal cord (1 of 2)
Paralyzed right vocal cord, with bowing and atrophy. Here, the left vocal cord is maximally but incompletely abducted. Subtle markings are for reference with photo 2.

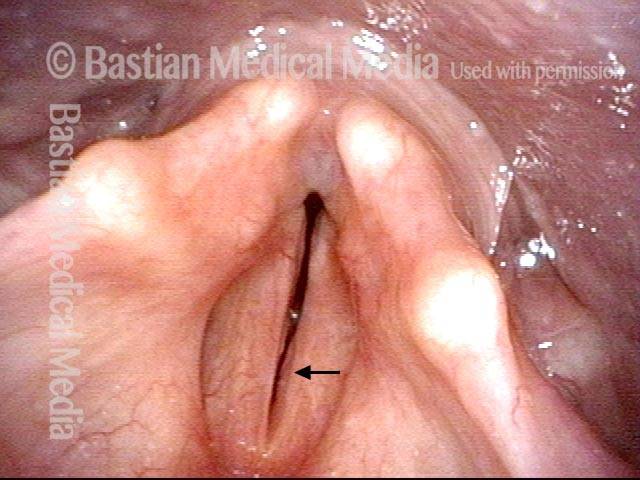
Indrawing with inspiration (2 of 2)
With elicited inspiration, the mucosa of the undersurface of both vocal cords indraws due to Bernouilli effect/ micro-vortices and further narrows the airway. At the same time, the patient involuntarily makes inspiratory voice.
Breathing Tube Injury, not Vocal Cord Paralysis
This middle-aged woman was injured severely in an auto accident as a teenager. Recovery involved a long stay in ICU, and ventilation via a breathing (endotracheal) tube for a few weeks prior to tracheotomy.
Fifteen years earlier, a posterior commissuroplasty was done by me on the left side. Severely short of breath before that procedure, she said the improvement was such that she was able to do most activities of daily living remarkably well for many years. While still much better than prior to the posterior commissuroplasty, she has felt a little more limited in the past few years and wants now another similar airway-widening procedure. Speaking voice can easily pass for normal, though she thinks it is occasionally a little rough.
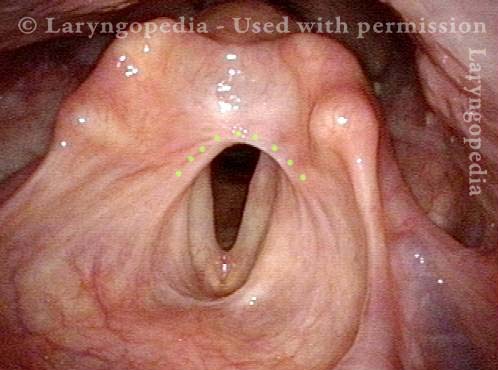
Aperture is very narrow (1 of 6)
Seen from a distance, during exhalation, the vocal cord aperture is perhaps 30% of normal.

Involuntary inspiratory phonation (2 of 6)
When asked to inspire rapidly, even in this distant view, the vocal cords can be seen to in-draw and vibrate (see blur), creating involuntary inspiratory phonation. Inspiratory phonation time is estimated at 2.5 seconds, rather than the normal 1 second or less.
Divot on left vocal cord (3 of 6)
The shallow “divot” of the left cord (right of photo) is all that remains of what would have been a much deeper divot created at the time of posterior commissuroplasty, 15 years earlier. The dashed line indicates the likely magnitude of laser excision.

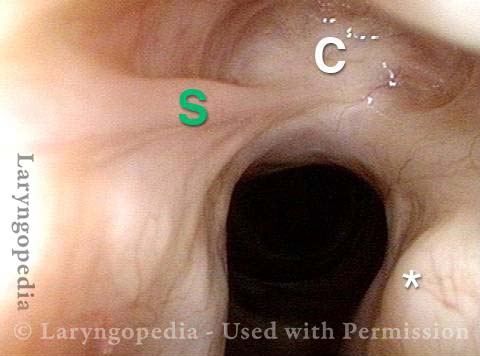
Endotracheal tube injury (4 of 6)
The full extent of the original endotracheal tube injury is seen best in this view of the extreme posterior commissure. One can almost see the upper surface of the cricoid cartilage marked with “C” showing also a scar band between arytenoid and cricoid cartilages, especially on the right (at S).
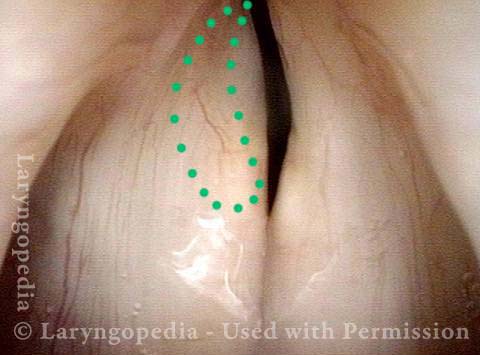
Laser cookie bite (5 of 6)
The posterior commissure during phonation shows the divot on the left cord (right of photo). The dashed line shows the approximate magnitude of the laser “cookie bite” to be created at the time of surgery. But the lighter dotted line is a typical remaining divot after full healing. Interestingly, (as explained by Charles’ Law) if even this small area is added to the size of the glottic aperture while breathing, the patient will notice a significant improvement of exercise tolerance.
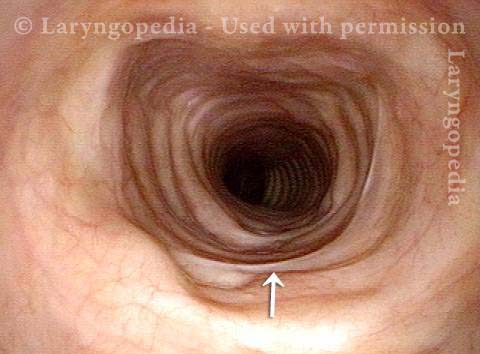
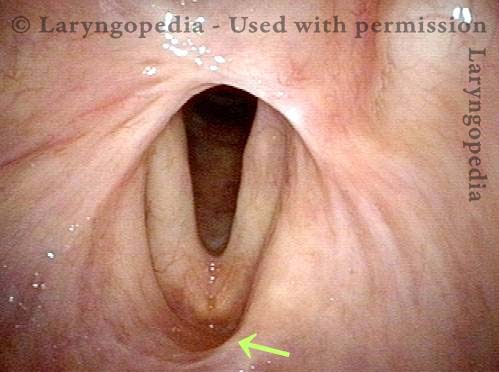
Surface scarring in the tracheotomy (6 of 6)
When there is a scar anywhere in the airway, the clinician must make sure there isn’t another causing narrowing. In this case there is no narrowing, but the tracheotomy site shows surface scarring at the arrow.
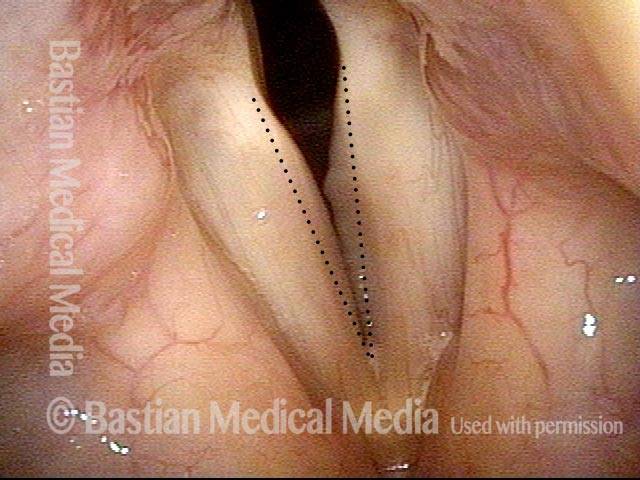
Smoker’s Polyps with Two Explanations for Bruising
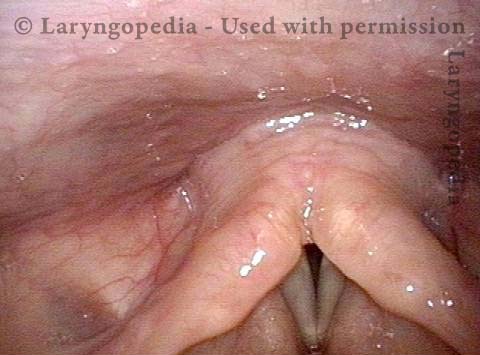
Convexed vocal cords (1 of 4)
Abducted, breathing position. Note that the margin of both vocal cords is slightly convex. See dotted line for normal, perfectly straight margin.
Inspiratory phonation (2 of 4)
Inspiratory phonation in-draws the mild Reinke’s edema (smoker’s type polyp formation).
Open phase, faint translucency (3 of 4)
Strobe illumination, at E4 (approximately 330 Hz), mostly open phase.
Closed phase, faint translucency (4 of 4)
Note again in closed phase.
Nonorganic Breathing Disorder, Laryngeal
Nonorganic breathing disorder, laryngeal (1 of 3)
Nonorganic breathing disorder in a patient who makes loud inspiratory noise with athletic exertion. Images shows functional partial closure during inspiration as a nonorganic phenomenon.
Nonorganic breathing disorder, laryngeal (2 of 3)
Normal abduction of vocal cords with elicited sniffing.
Nonorganic breathing disorder, laryngeal (3 of 3)
Note the convexity and vibratory blurring of the free margins, correlating with inspiratory phonation.

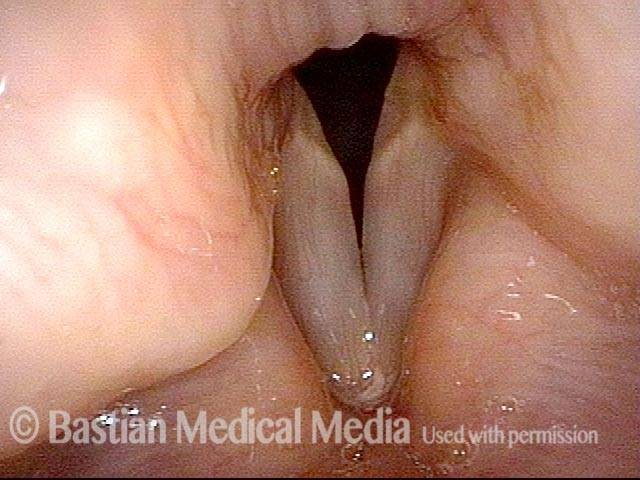
Bilateral Vocal Cord Paralysis
Maximum space between cords (1 of 2)
After thyroidectomy many years earlier, the patient’s exercise tolerance became minimal without becoming short of breath and making loud inspiratory vocal sounds. Eventually, she underwent tracheotomy, which she has continued to wear for more than ten years. This view shows the maximum space between her vocal cords, which paradoxically occurs when she exhales.

View during inhalation (2 of 2)
When asked to inhale with tracheotomy tube momentarily plugged, the passing air causes the vocal cords to indraw slightly and come into vibration, creating “involuntary inspiratory phonation.” Note the faint convexity and grey blur where the mucosa is vibrating.
Supraglottic (above the vocal cord) Scarring as a Result of Radiotherapy
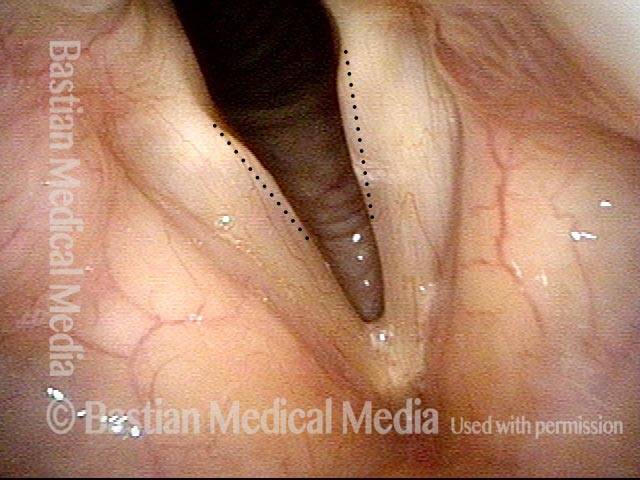
Supraglottic Scarring (1 of 4)
This man was treated with radiotherapy for an early vocal cord cancer, approximately 35 years prior to this examination. For those 35 years, his breathing has been slightly noisy, and he feels mild restriction of exercise tolerance. Here, you see an arch-like scar above the posterior end of the vocal cords (dotted line).
Hoarseness caused by radiation effects (2 of 4)
The vocal cords can come together fully when he makes voice; his mild hoarseness is therefore not due not to the scar band, but instead to reduction of vibratory flexibility of the surface tissue of the vocal cords due to radiation effects.

Cords don’t close completely (3 of 4)
In this closer view, one can also appreciate that the vocal cords do not separate to as wide a “V” as would be normal, and this is the main explanation of the harsh inspiratory noise and slight prolongation of time to fill his lungs with forced inspiration. Note as well additional evidence of radiation damage (scar band) at the arrow.
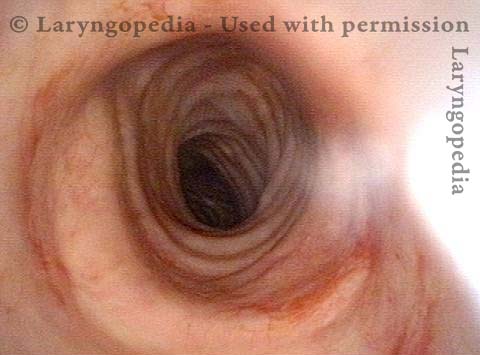
Normal caliber trachea (4 of 4)
A view is obtained of his (normal caliber) trachea, to make certain that there is not an additional reason for his noisy breathing.
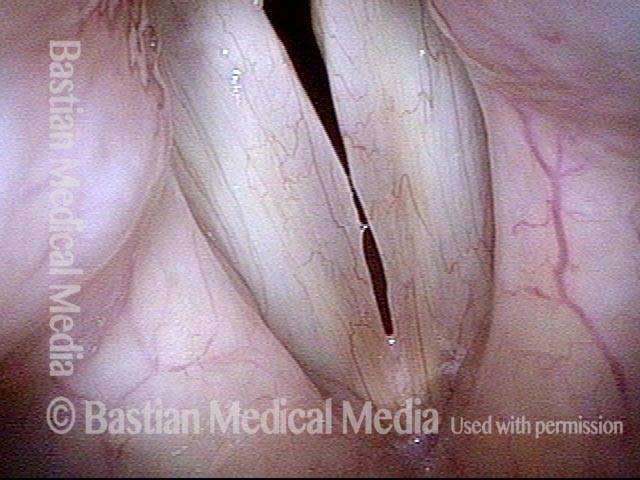
Reinke’s (Smoking-Related) Edema and How to See It
Convexed vocal cords (1 of 4)
Abducted, breathing position. Note that the margin of both vocal cords is slightly convex. See dotted line for normal, perfectly straight margin.
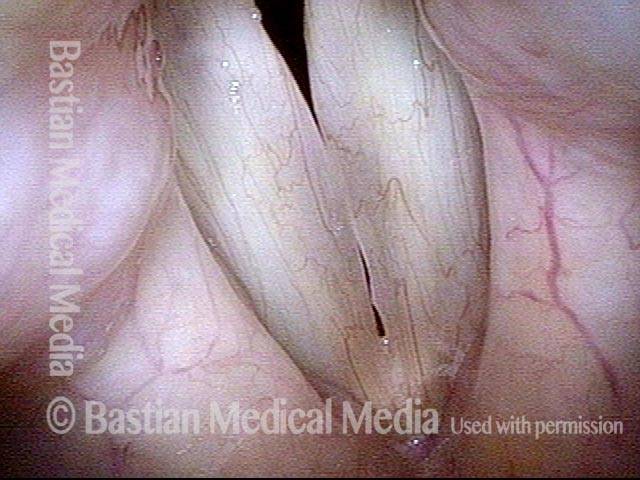
Inspiratory phonation (2 of 4)
Inspiratory phonation in-draws the mild Reinke’s edema (smoker’s type polyp formation).
Open phase, faint translucency (3 of 4)
Strobe illumination, at E4 (approximately 330 Hz), mostly open phase.
Closed phase, faint translucency (4 of 4)
Note again in closed phase.