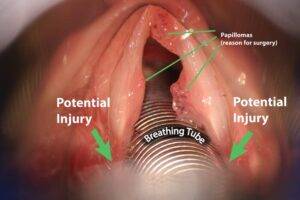
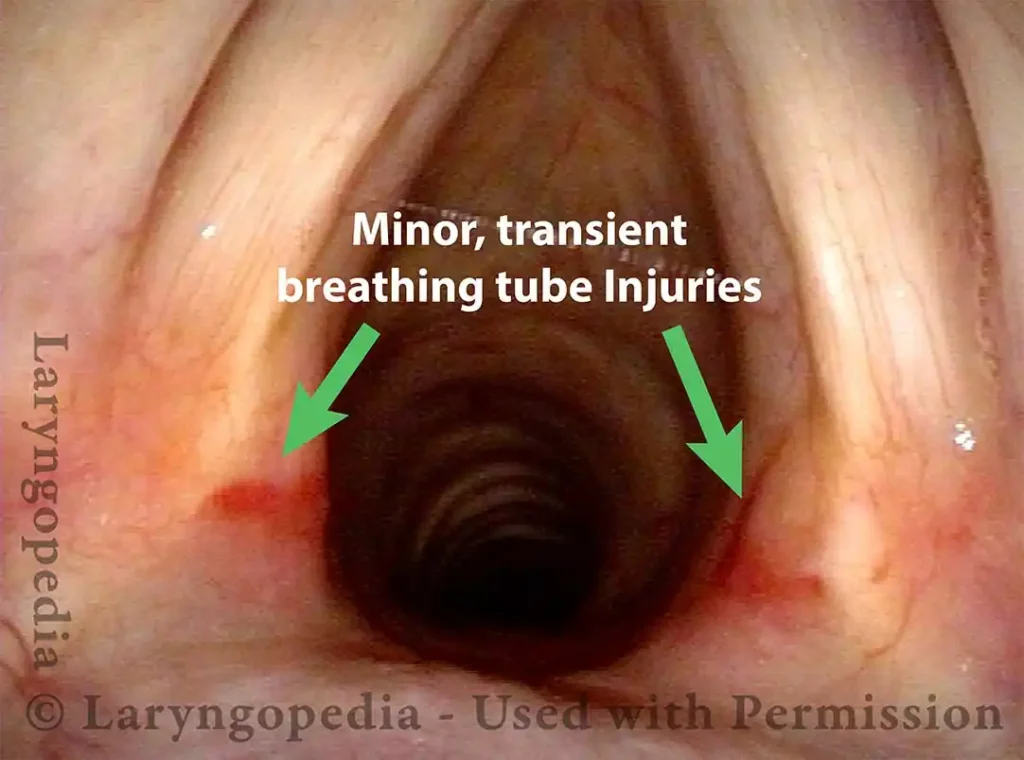
 Injury, typically to the posterior part of both vocal cords, caused by an endotracheal tube1. An endotracheal tube may be used briefly during general anesthesia for surgery, but may be in place for much longer in persons suffering respiratory failure or neurological injury. When severe, the hallmark vocal phenomenology of intubation injury is breathy-pressed phonation.
Injury, typically to the posterior part of both vocal cords, caused by an endotracheal tube1. An endotracheal tube may be used briefly during general anesthesia for surgery, but may be in place for much longer in persons suffering respiratory failure or neurological injury. When severe, the hallmark vocal phenomenology of intubation injury is breathy-pressed phonation.
Breathing Tube Injury may Correlate with Side of Mouth
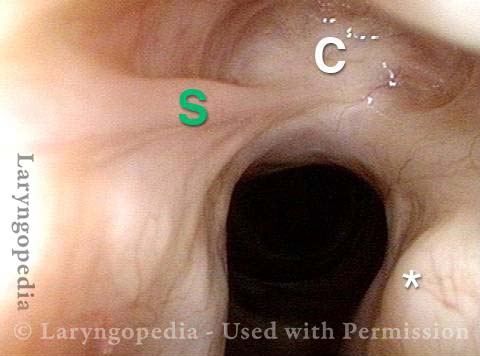
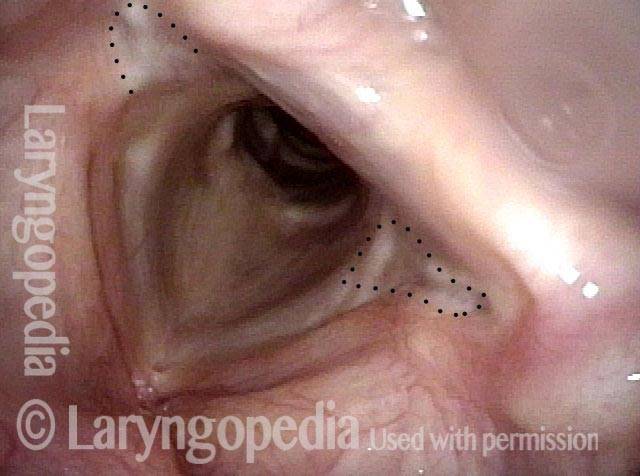
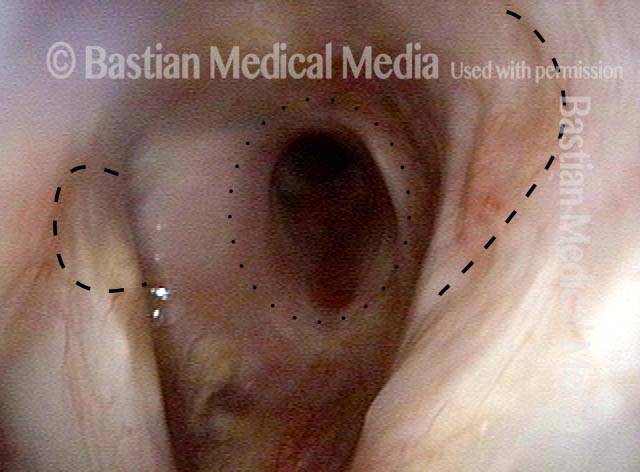
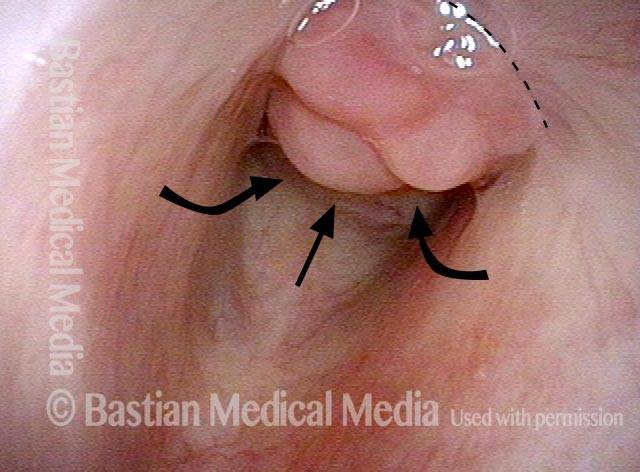
This person was intubated for 2 weeks due to complications after major surgery. He was sent for evaluation due to hoarseness, with a diagnosis from elsewhere of vocal cord paralysis.
During the consultation, he described himself as a very quiet person (a “2” on the 7-point talkativeness scale), and living a quiet life. After the examination below his wife was asked “Was the tube taped to the left corner of his mouth? Or do you not remember?” She replied, “Definitely, the left corner.”
This history raises the question: “Is the diagnosis of paralysis from elsewhere correct, or is the actual diagnosis vocal cord fixation from intubation injury?”
Vocal cord fixation (1 of 4)
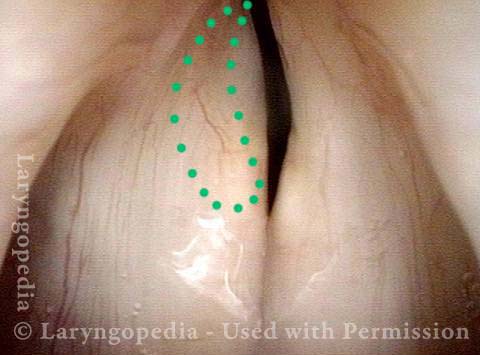
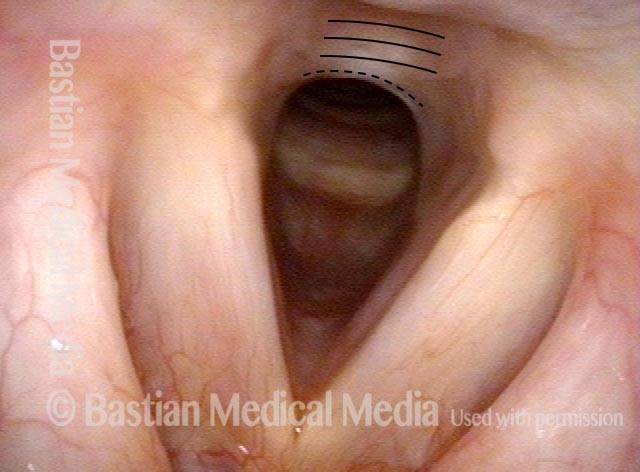
Paralysis (2 of 4)

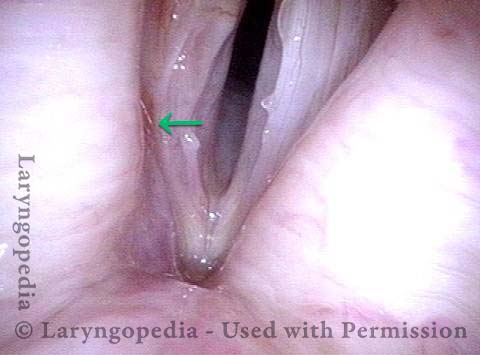
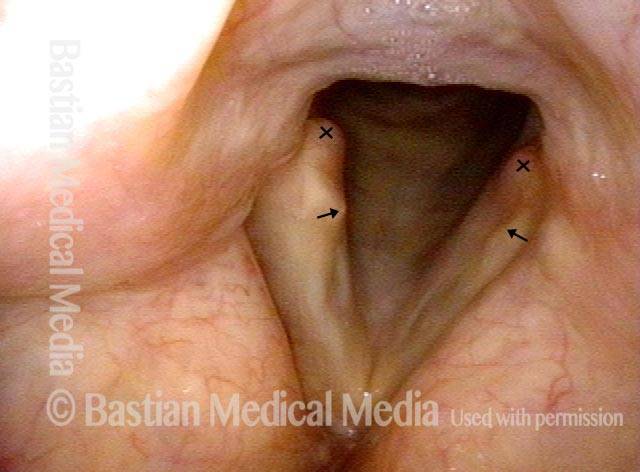
Injury from intubation tube (3 of 4)
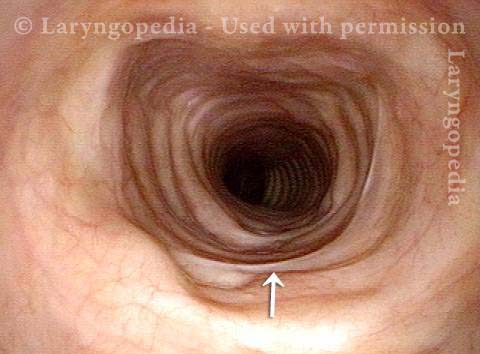
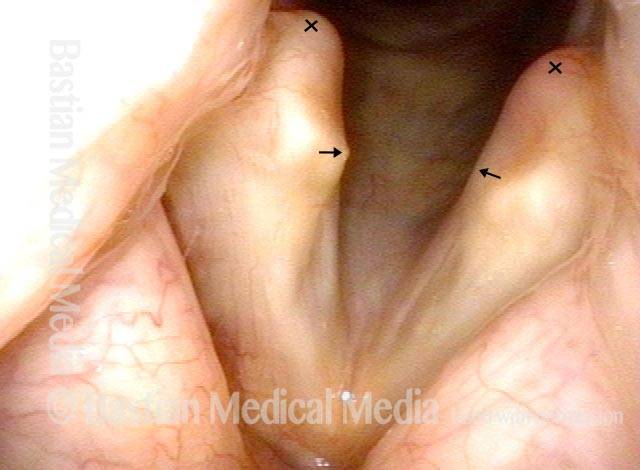
Mismatch of levels (4 of 4)

Breathing Tube Injury, not Vocal Cord Paralysis
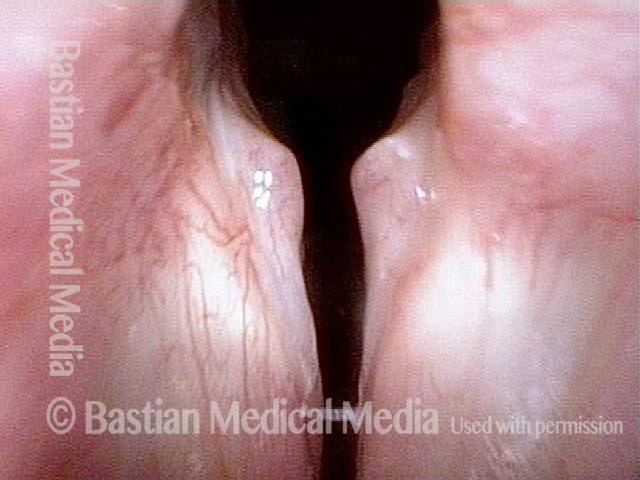
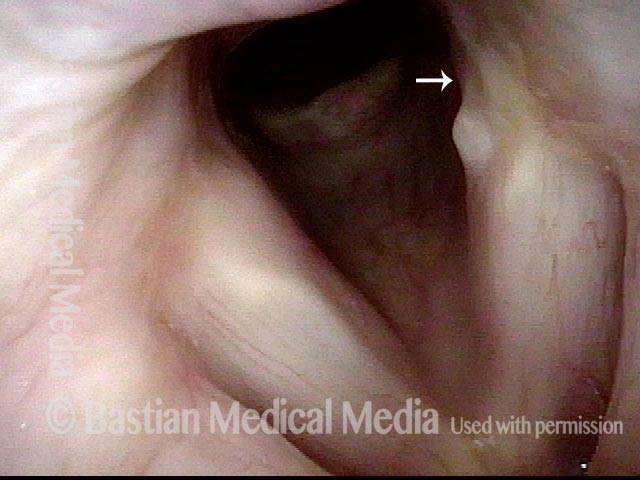
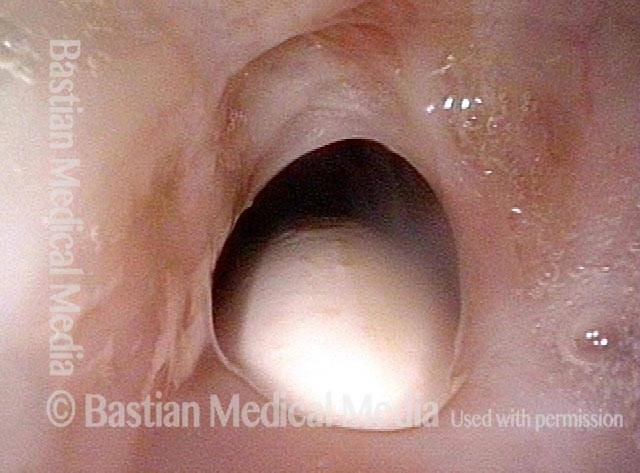
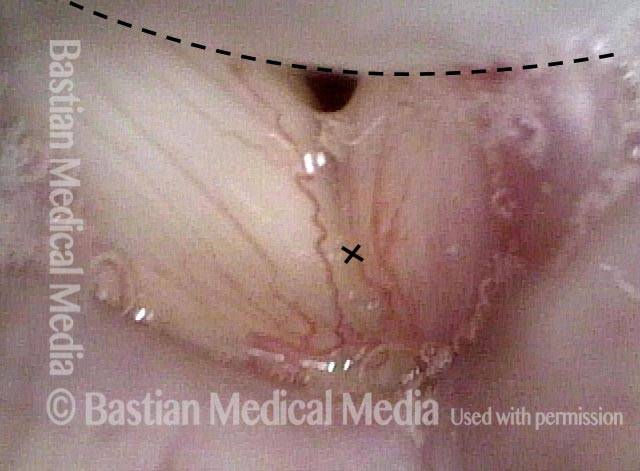
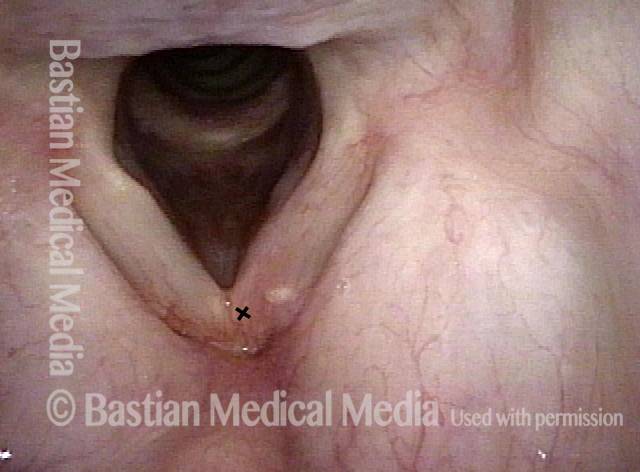
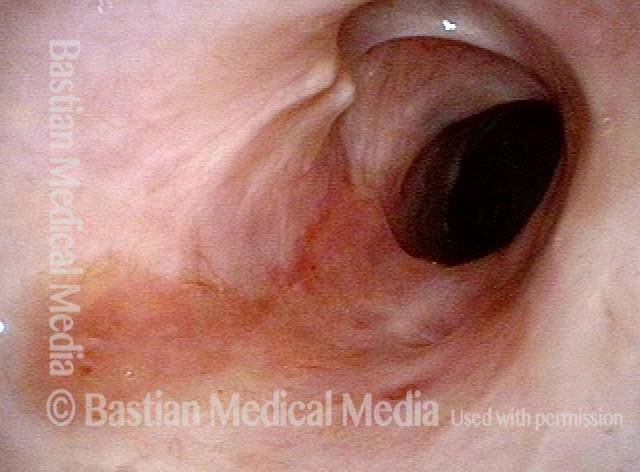
This middle-aged woman was injured severely in an auto accident as a teenager. Recovery involved a long stay in ICU, and ventilation via a breathing (endotracheal) tube for a few weeks prior to tracheotomy. Fifteen years earlier, a posterior commissuroplasty was done by me on the left side. Severely short of breath before that procedure, she said the improvement was such that she was able to do most activities of daily living remarkably well for many years. While still much better than prior to the posterior commissuroplasty, she has felt a little more limited in the past few years and wants now another similar airway-widening procedure. Speaking voice can easily pass for normal, though she thinks it is occasionally a little rough.
Aperture is very narrow (1 of 6)

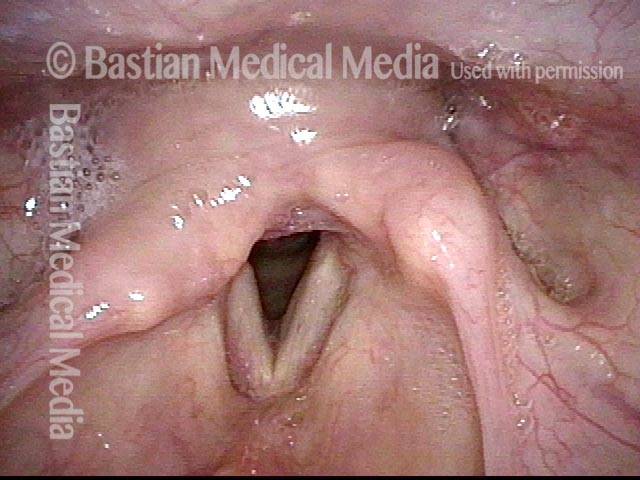
Involuntary inspiratory phonation (2 of 6)
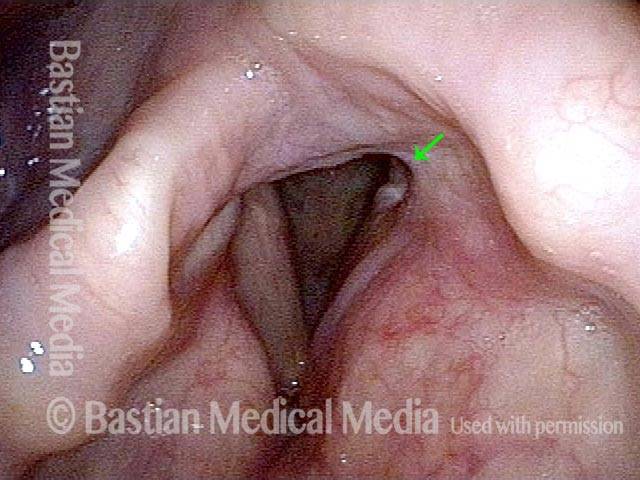
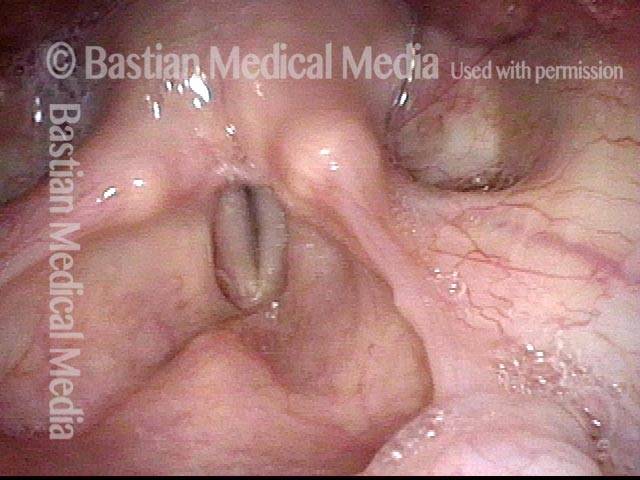
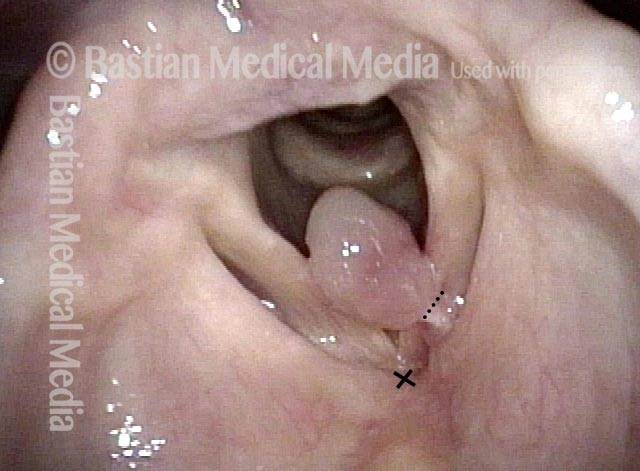
Divot on left vocal cord (3 of 6)

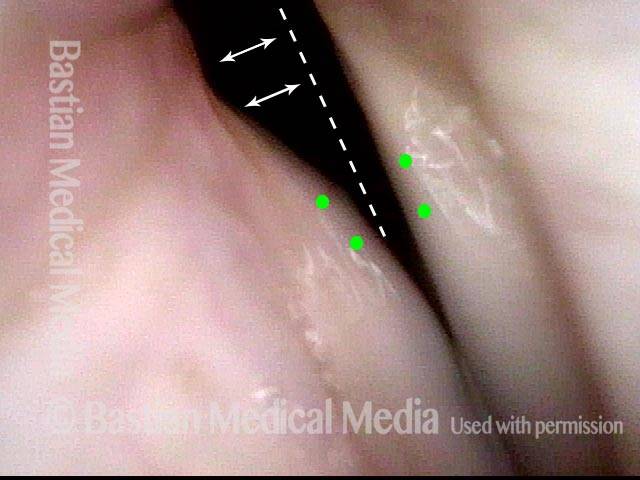
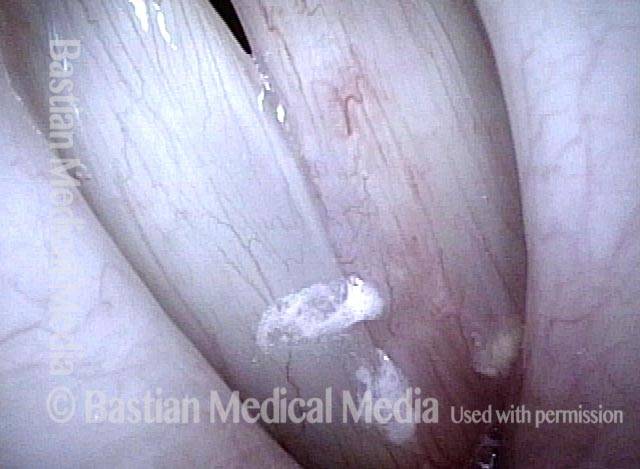
Endotracheal tube injury (4 of 6)
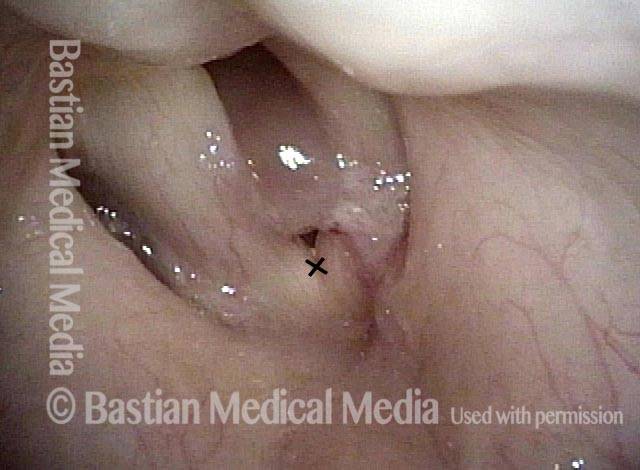
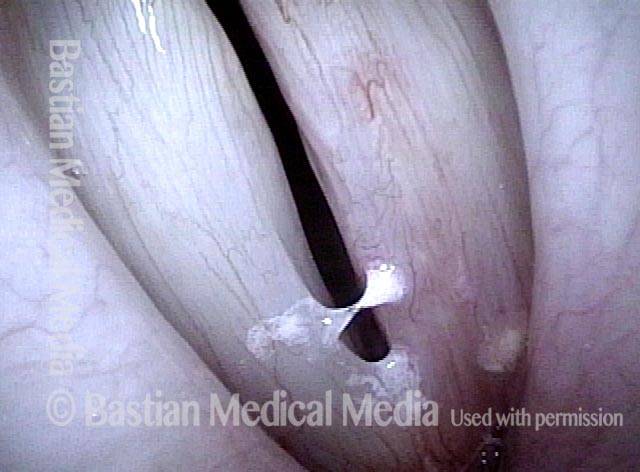
Laser cookie bite (5 of 6)
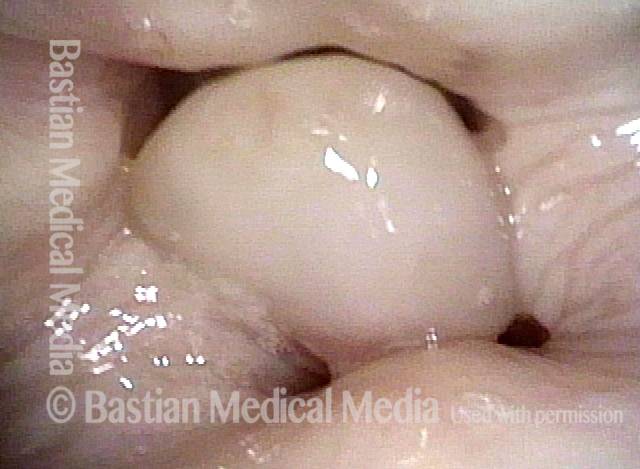
Surface scarring in the tracheotomy (6 of 6)
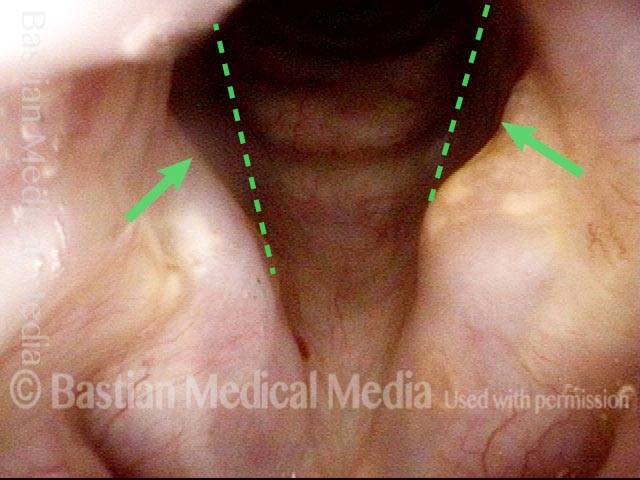
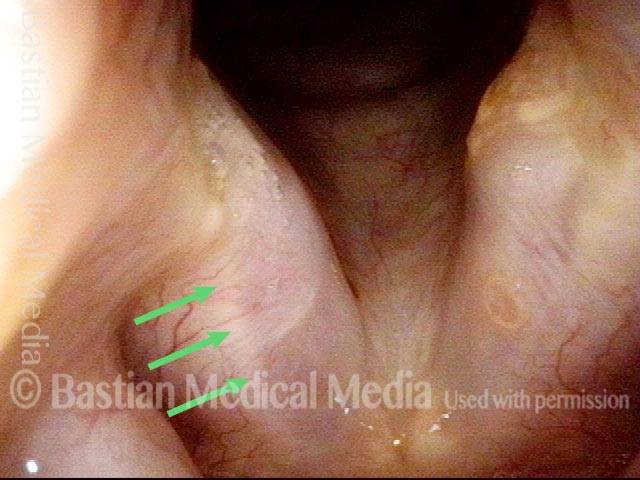
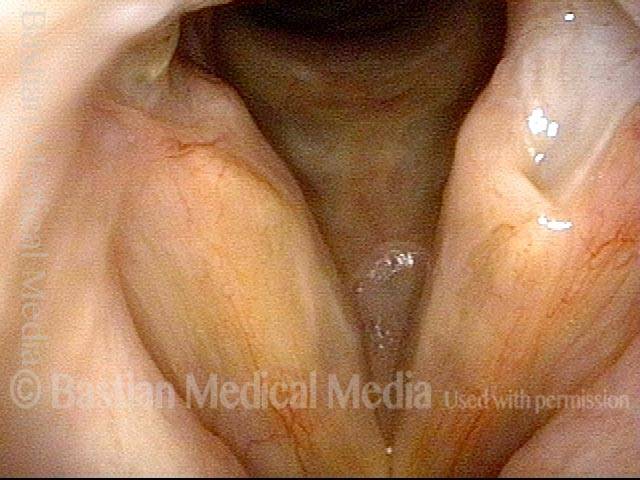
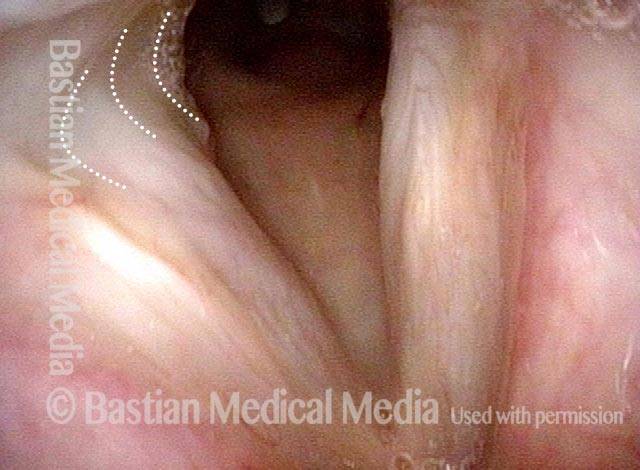
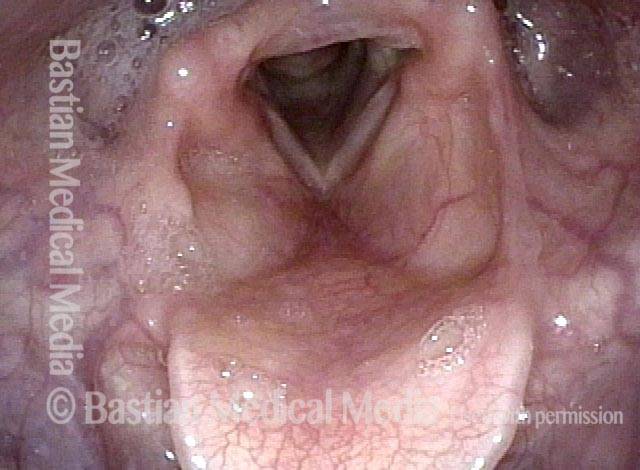
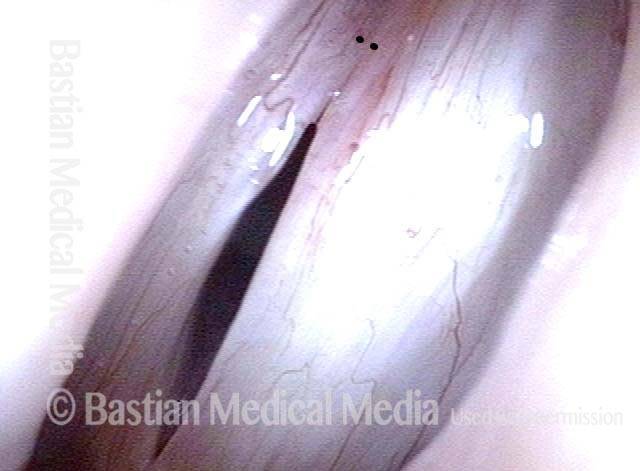
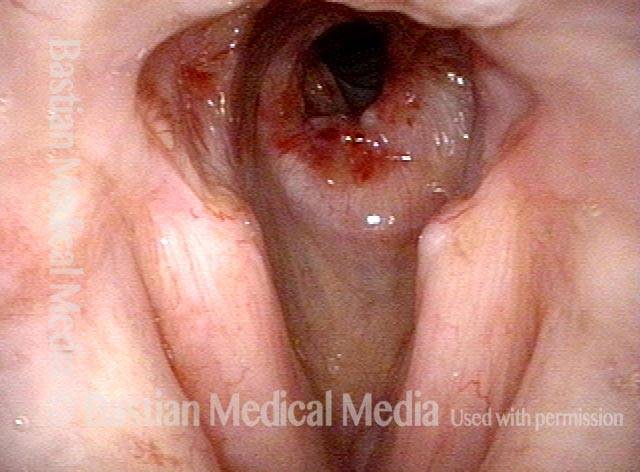
Breathing Tube Injury—A Rare Complication of Intubation for General Anesthesia
Inflamed vocal cord (1 of 5)

Closer view (2 of 5)

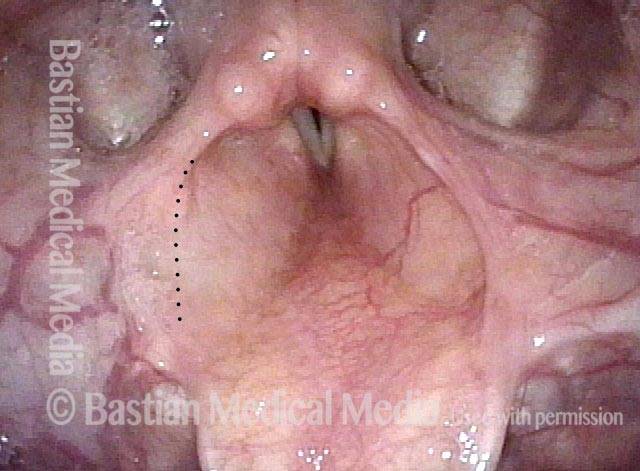
Scarring from intubation tube (3 of 5)

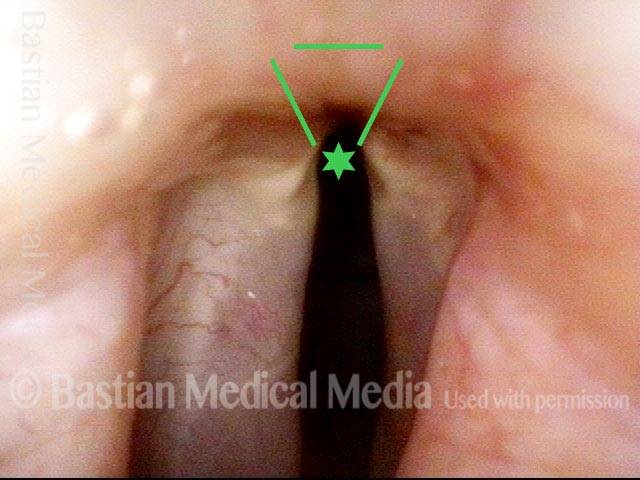
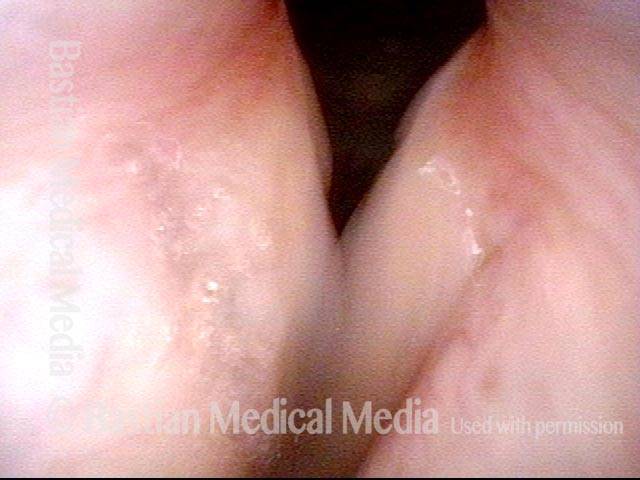
Mucosal Injury (4 of 5)

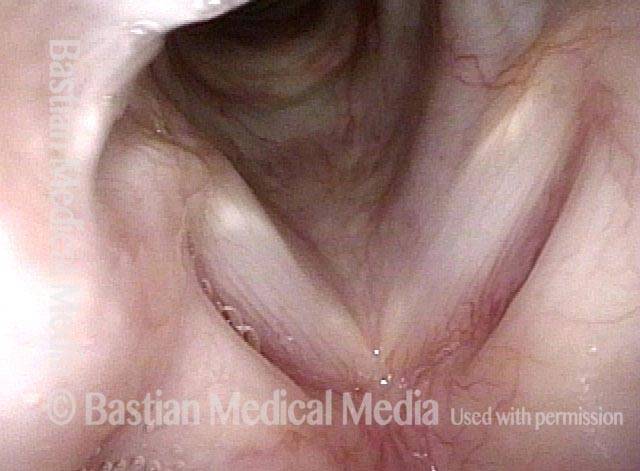
Flaccidity of right vocal cord (5 of 5)
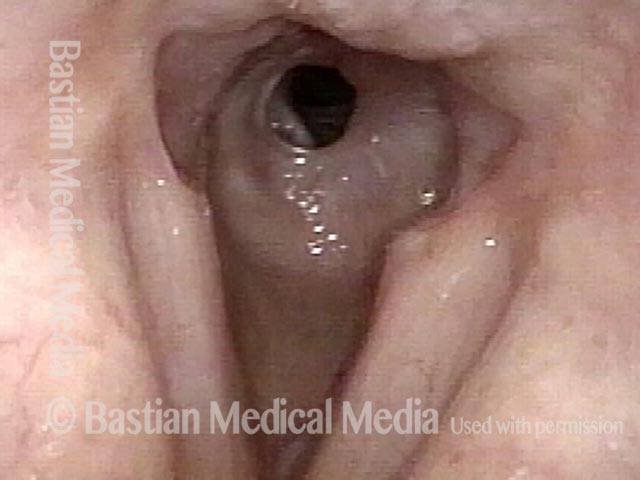
Conclusion
While we try to explain abnormality due to one cause, here, the patient has a mucosal injury and paresis of right TA and LCA muscles, which can also follow intubation. This explains why the initial postop voice was so weak and whispery, and also the rapid partial improvement. This voice will likely continue to improve and be very functional as a speaking voice. Fortunately, this person is not a singer, as clarity especially in upper notes, will likely be remain impaired even after full recovery.
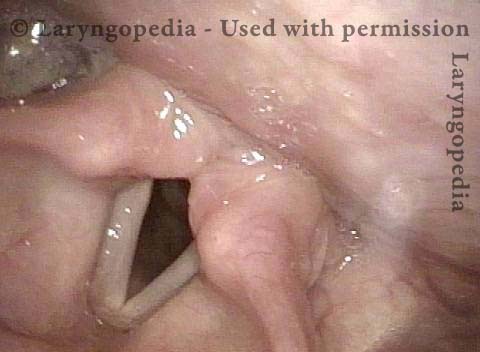
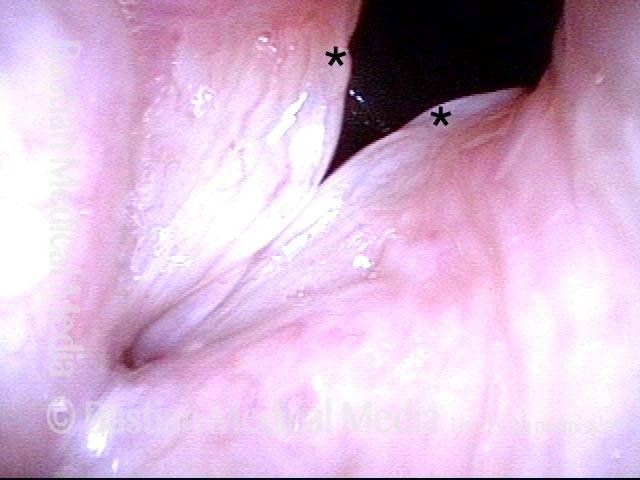
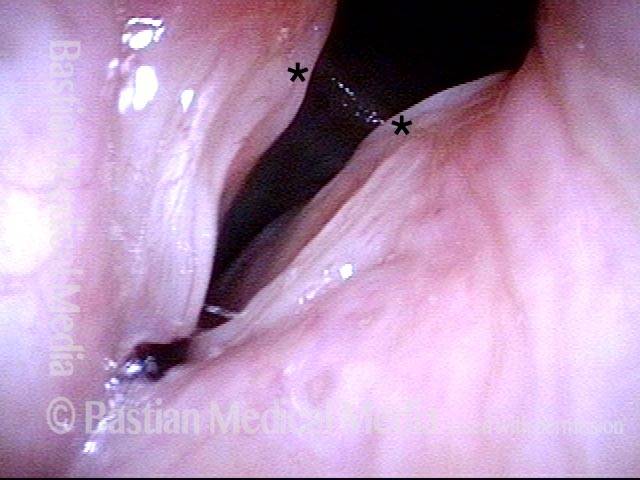
Breathing Tube Injury: Synechiae
Breathing Tube Injury (1 of 4)

Post-intubation synechiae (2 of 4)
Breathing Tube Injury (3 of 4)
Breathing Tube Injury (4 of 4)
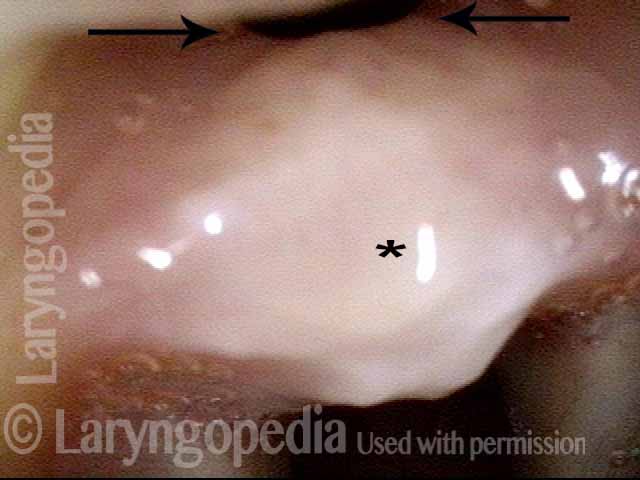
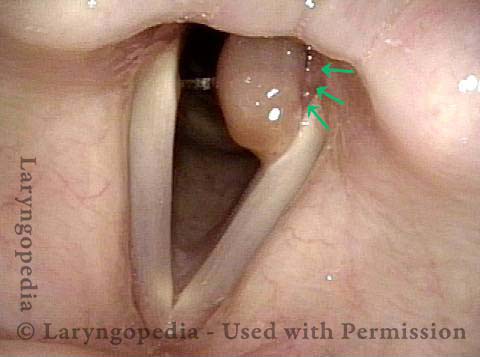
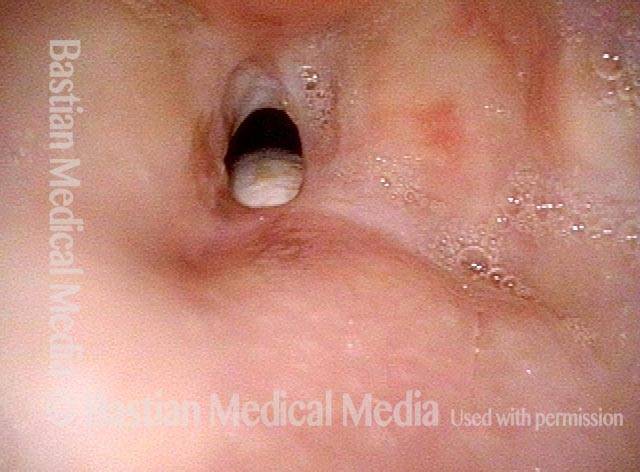
“Tattoo” of blood after detachment of intubation granuloma
Intubation granuloma (1 of 5)
Pedunculation in process (2 of 5)
Granuloma is gone (3 of 5)
Blood tattoo (4 of 5)
Blood Tattoo (5 of 5)
Intubation injury audio with photos:
Voice sample of a patient with a cricoartyenoid joint intubation injury (see this patient’s photos just below):
Intubation injury (1 of 3)
Intubation injury (2 of 3)
Maximum phonatory closure (3 of 3)
Intubation Injury Causing Partially Frozen Cricoarytenoid Joints
Intubation injury (1 of 4)

Intubation injury (2 of 4)
Closed phase of vibration (3 of 4)
Open phase of vibration (4 of 4)
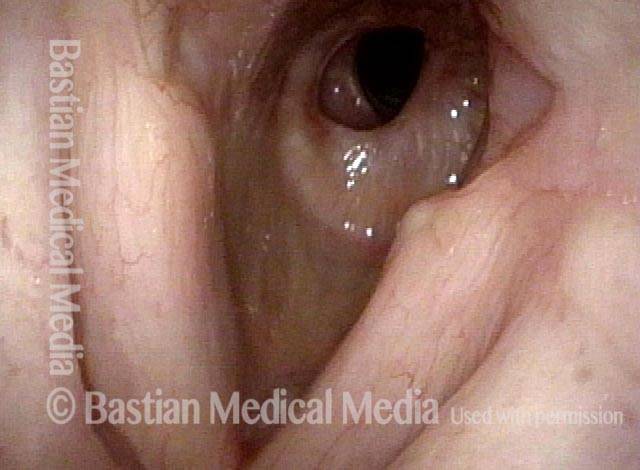
Intubation Injury
Abducted, breathing position (1 of 2)
Intubation injury (2 of 2)

Example 2
Intubation injury (1 of 3)
Posterior commissure divots (2 of 3)
Intubation injury (3 of 3)

Example 3
Intubation injury (1 of 4)
Breathy Voice (2 of 4)
Vocal cord fixation (3 of 4)

During phonation (4 of 4)
Forcing the Larynx to Give Up Its (Paresis and Intubation Injury) Secrets
Intubation injury (1 of 4)
Forceful exhalation (2 of 4)

Phonation begins (3 of 4)

LCA (4 of 4)

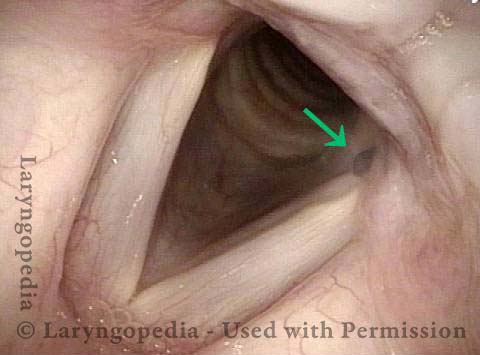
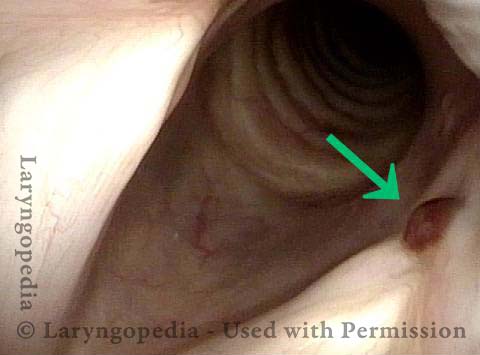
Intubation Injury, Including A Subglottic Synechia
Intubation injury, including a subglottic synechia (1 of 2)
Intubation injury, including a subglottic synechia (2 of 2)

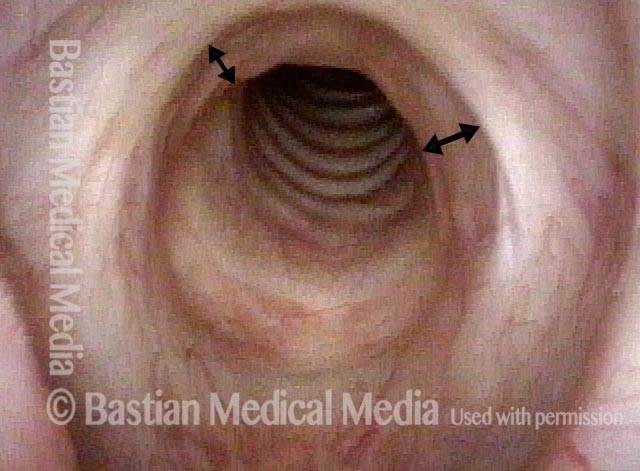
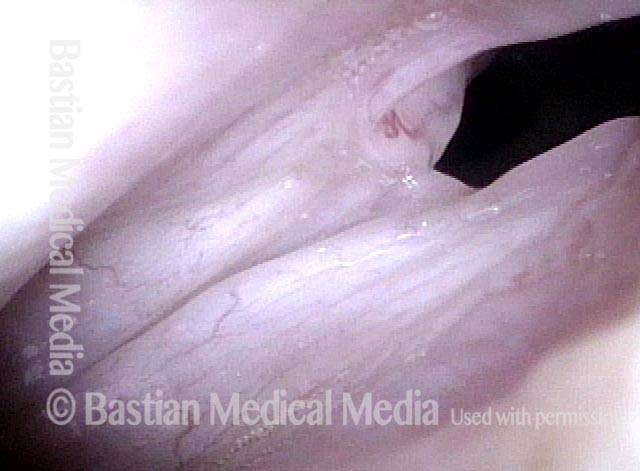
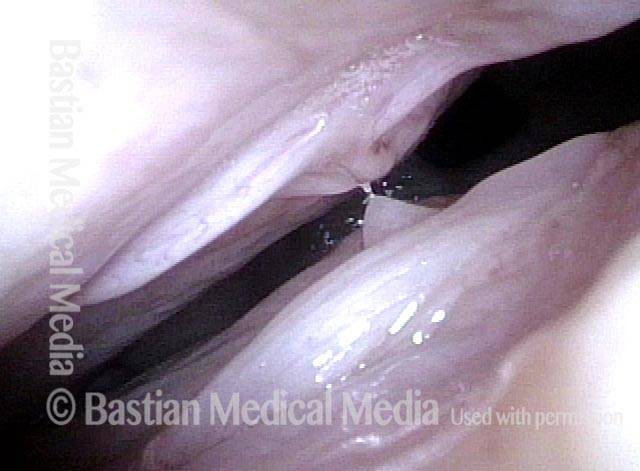
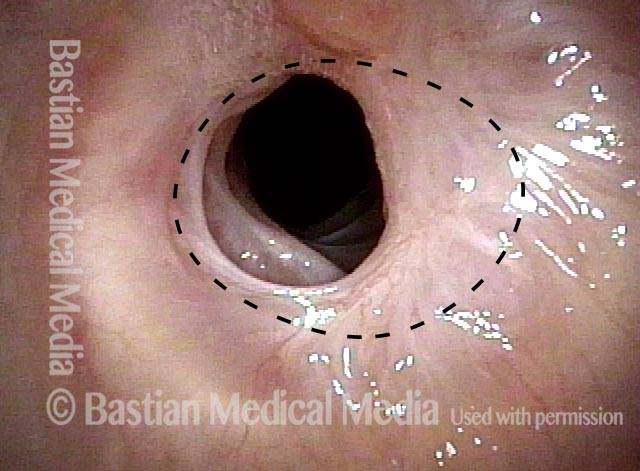
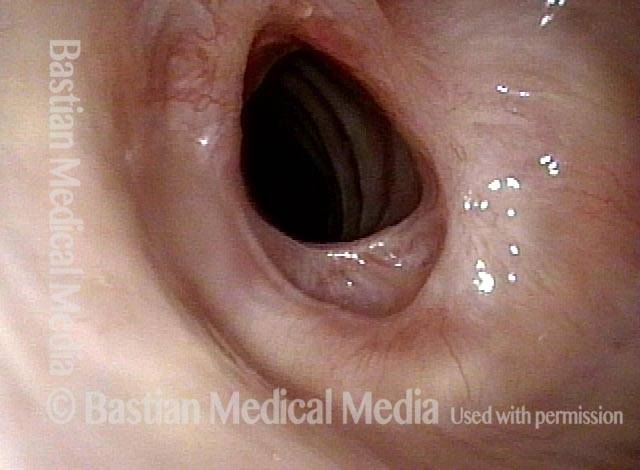
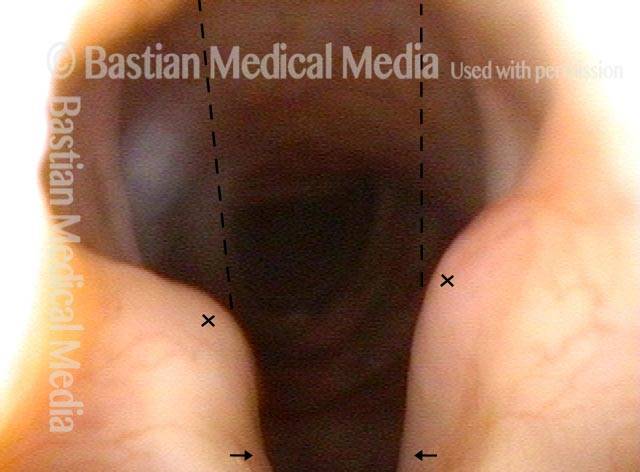
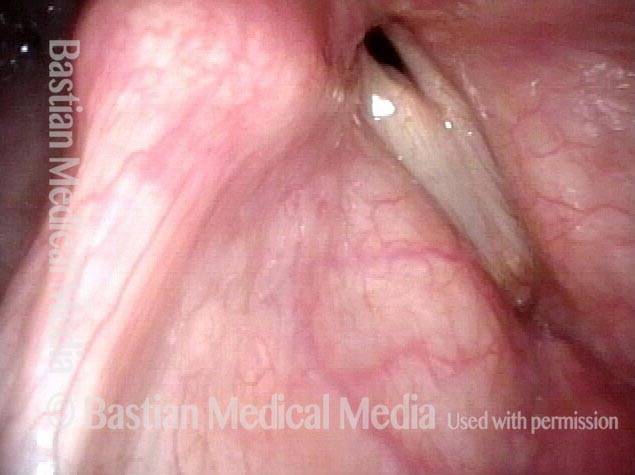
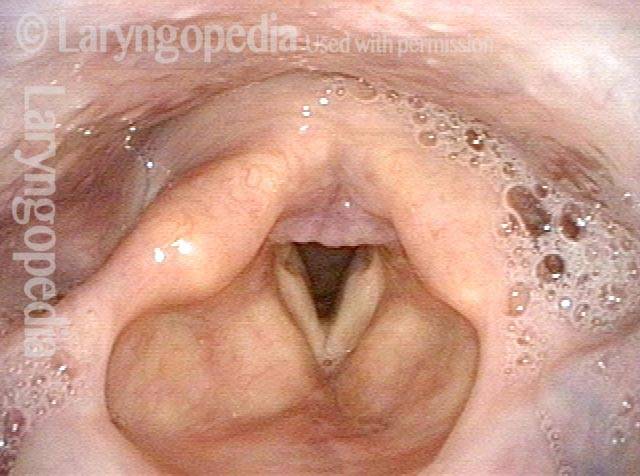
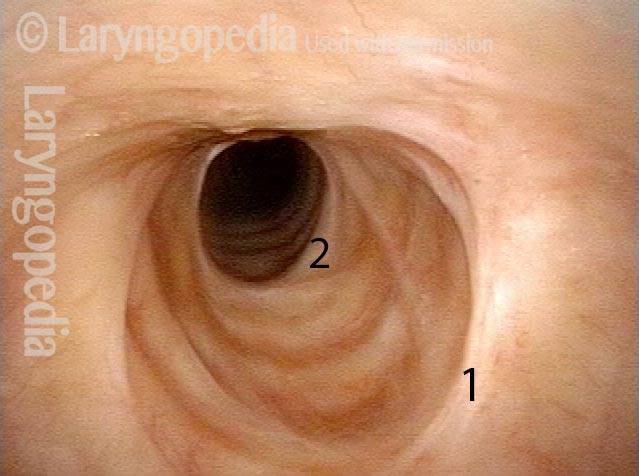
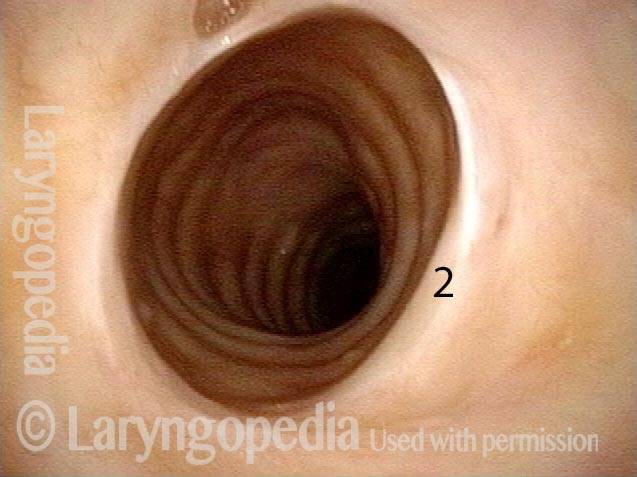
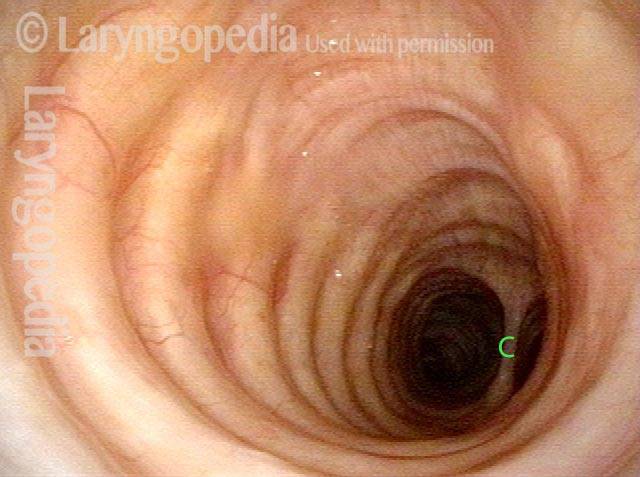
Post-Intubation Stenosis
Endotrachel tube injury (1 of 4)
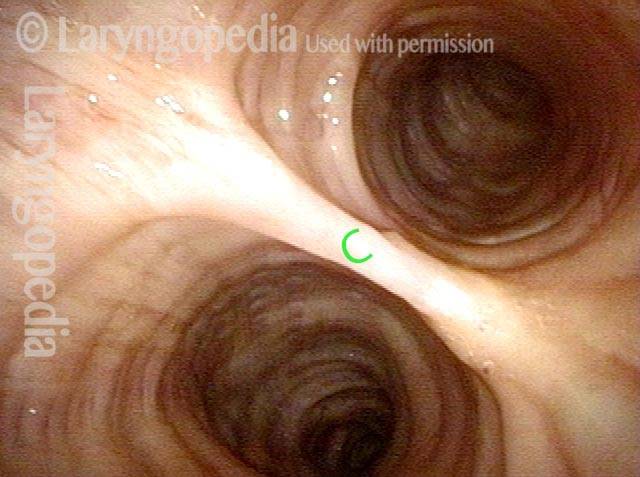
Closer view, between the posterior vocal cords (2 of 4)

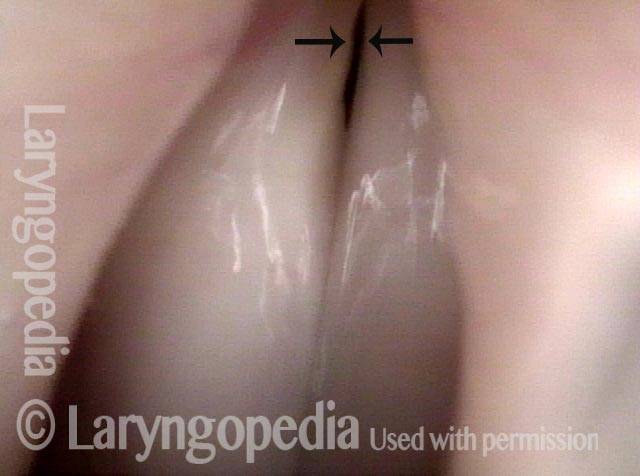
Even closer view, showing upper surface of the tube (3 of 4)
Non-inflammatory stenosis, caused purely by injury (4 of 4)
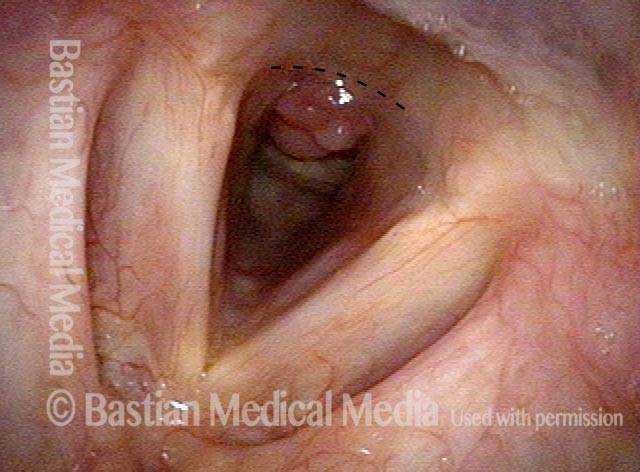
Vocal Cord “Tear” and Granuloma
Intubation injury (1 of 8)
Granuloma drawn into glottis (2 of 8)
Phonation (3 of 8)
Anterior commissure (4 of 8)
Granuloma detached (5 of 8)
Vocal cord blurring (6 of 8)

Closed phase (7 of 8)
Open phase (8 of 8)
Injured Adult Larynx from Intubation In Infancy
Intubation injury (1 of 6)
Phonation (2 of 6)
Breathing position (3 of 6)
Prephonatory instant (4 of 6)

Phonatory blurring (5 of 6)

Scarring in subglottis (6 of 6)
Intubation Injury to Voice, Airway, from Decades Ago
Severe intubation injury (1 of 5)
Subglottic stenosis (2 of 5)
Mid-distal trachea (3 of 5)

Posterior commissure keyhole (4 of 5)

Flaccidity (5 of 5)
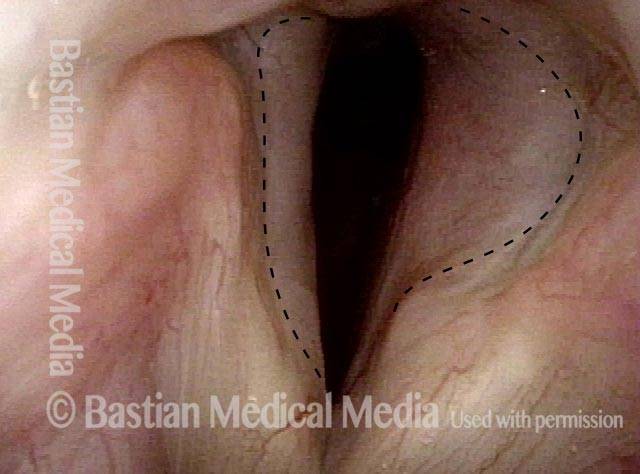
Injury at Two Levels from Breathing Tube-Particularly Clear
Posterior commissure divots (1 of 8)
Closed phase (2 of 8)
Open phase (3 of 8)
Subglottic stenosis (4 of 8)
Post dilation (5 of 8)
Closer view (6 of 8)
Final result (7 of 8)
Closer view (8 of 8)
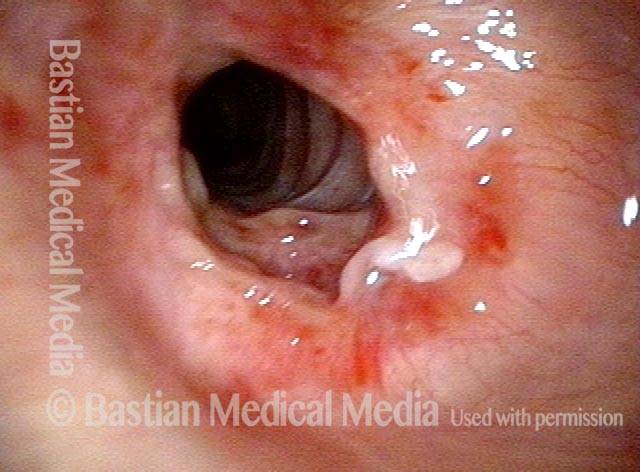
Subglottic Granulation and Curving Airstream
Intubation injury (1 of 4)
Lobules (2 of 4)
2 months later (3 of 4)
Scar band (4 of 4)

Double Whammy: Intubation Injury + Glottic Furrows
Intubation injury + glottic furrows (1 of 4)
Bilateral glottic furrows (2 of 4)
Intubation injury (3 of 4)
Phonatory position (4 of 4)

Sometimes You DO Remove Granulation to Avoid Tracheotomy
Granulation (1 of 8)

Closer view (2 of 8)

Post microlaryngoscopies (3 of 8)

Scarring (4 of 8)
Post posterior commissuroplasty (5 of 8)
Breathing improved (6 of 8)
Closer view (7 of 8)

Phonatory view (8 of 8)
Who Knew…? Many Such Injuries Are Never Found
Coughing evaluation (1 of 6)
Intubation scars (2 of 6)

Stenosis (3 of 6)
Further down trachea (4 of 6)
Below stenosis (5 of 6)
Carina (6 of 6)
A Strapping Young Man Whose Larynx Was Injured As A 1-lb Preemie!
Intubated as preemie (1 of 4)

Left vocal cord (2 of 4)

Vascular pattern (3 of 4)

“Closed” phase (4 of 4)

An “Inner Voice” Problem Viewed As An End-Organ Problem
Atrophied right vocal cord (1 of 4)

Vocal cords at high volume (2 of 4)
Strobe light, closed phase (3 of 4)

Open phase (4 of 4)

Intubation Scar With Pseudo-Polyp
Posterior swelling (1 of 3)

White scar (2 of 3)

Pseudopolyp (3 of 3)

- Bastian RW, Richardson BE. Postintubation phonatory insufficiency: an elusive diagnosis. Otolaryngol Head and Neck Surg. 2001; 124(6): 625-33. [↩]