![]()

Smoker’s Polyps, before and after Surgery (audio with photos)
Voice sample of a patient with smoker’s polyps, BEFORE surgery (see this patient’s photos just below):
Same patient, two months AFTER surgery (the occasional syllable dropouts are due to the recentness of surgery):
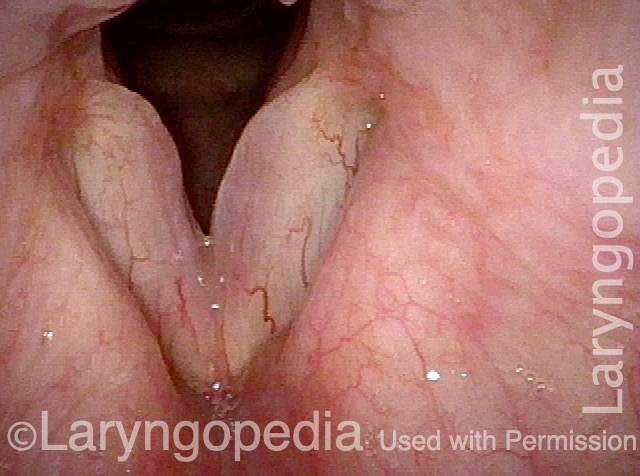
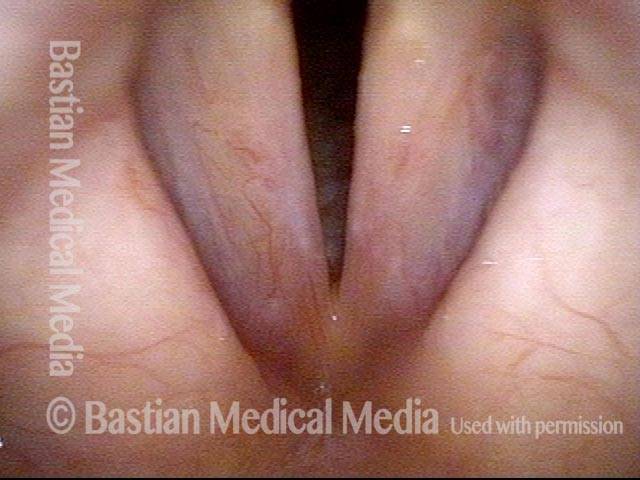
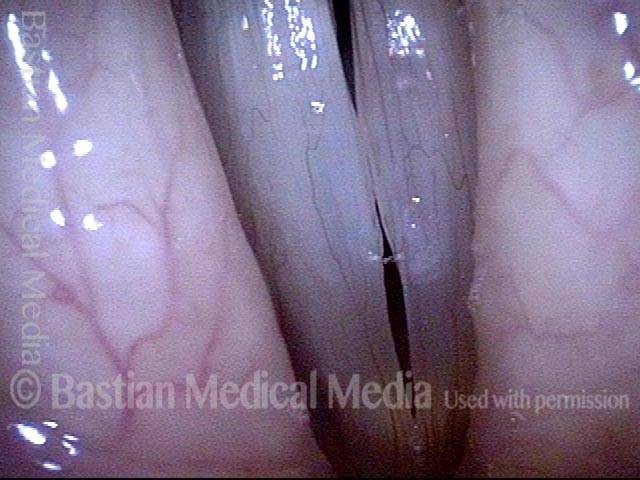
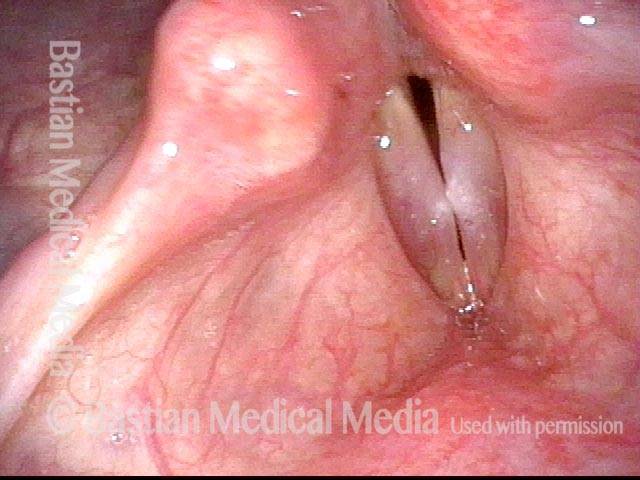
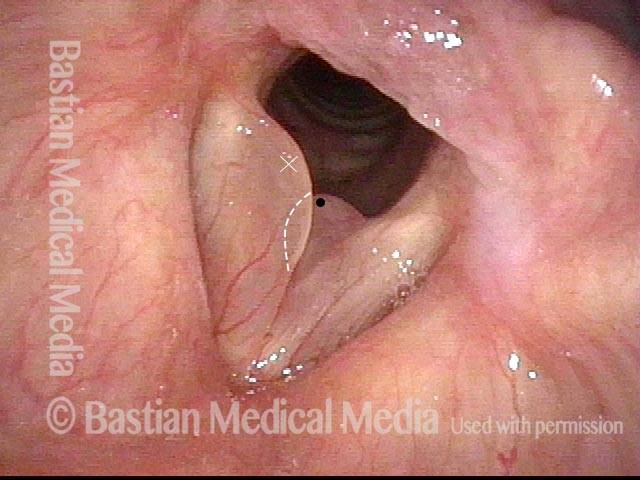
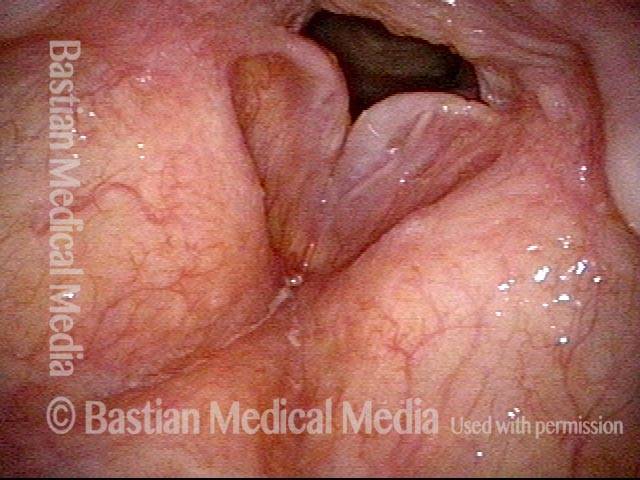
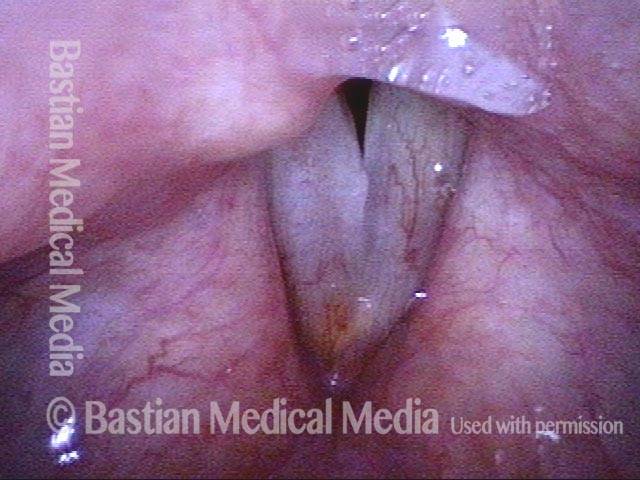
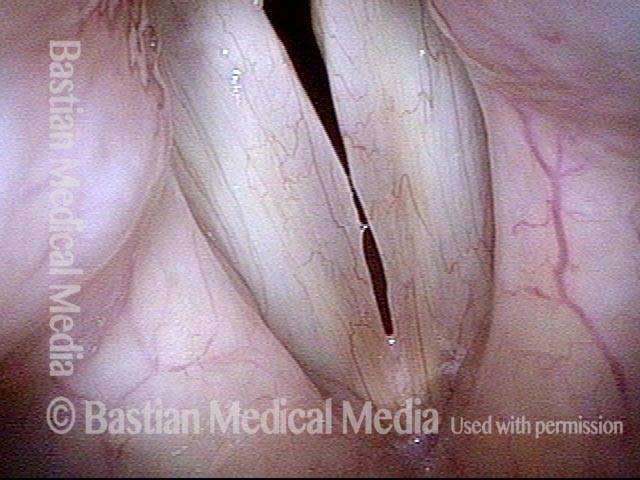
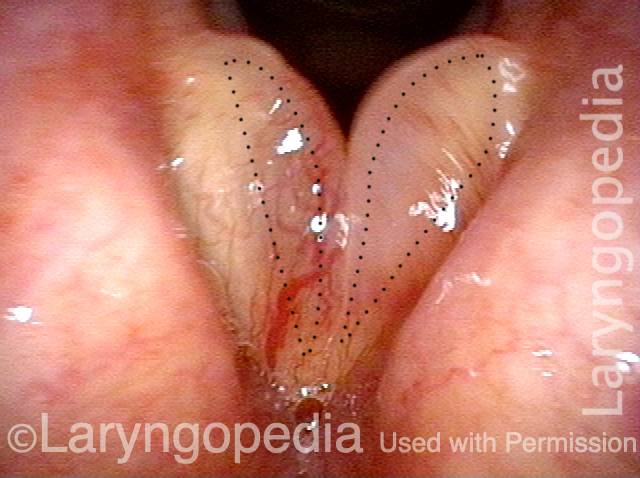
Smoker’s polyps, BEFORE surgery (1 of 4)
Even during quiet breathing, the convexity of the vocal cord margins (dotted lines show where normal margins would be) reveal the presence of smoker’s polyps.
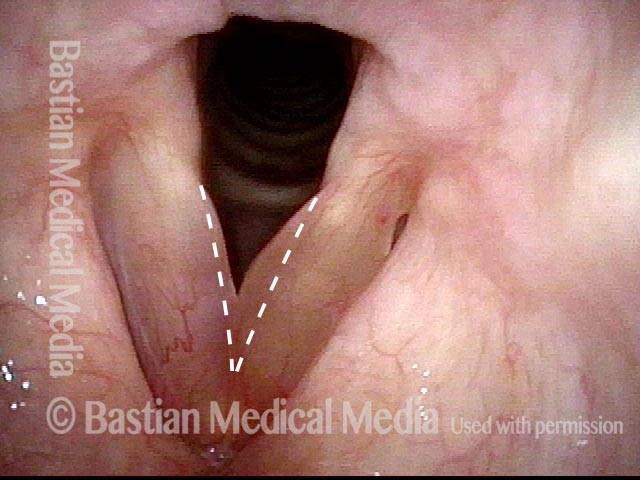
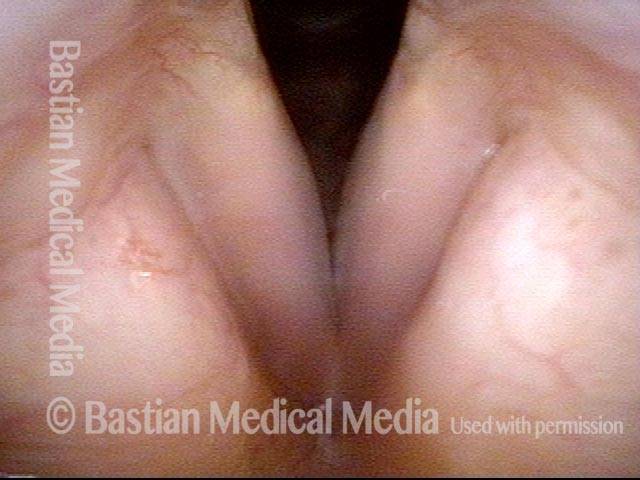
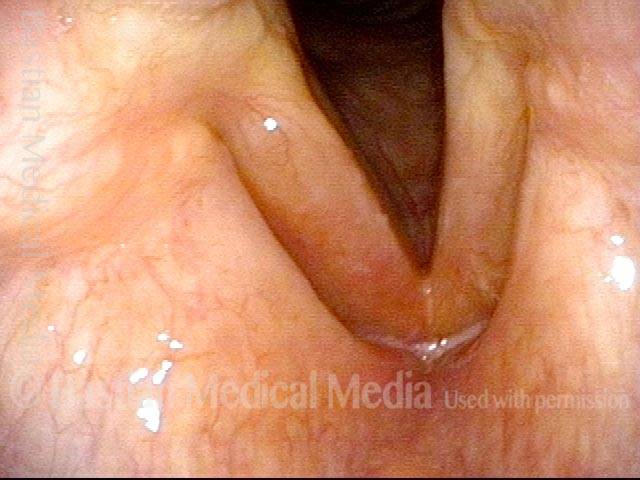
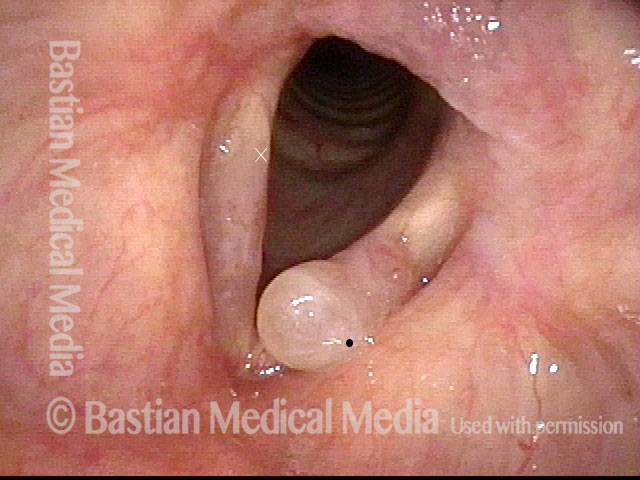
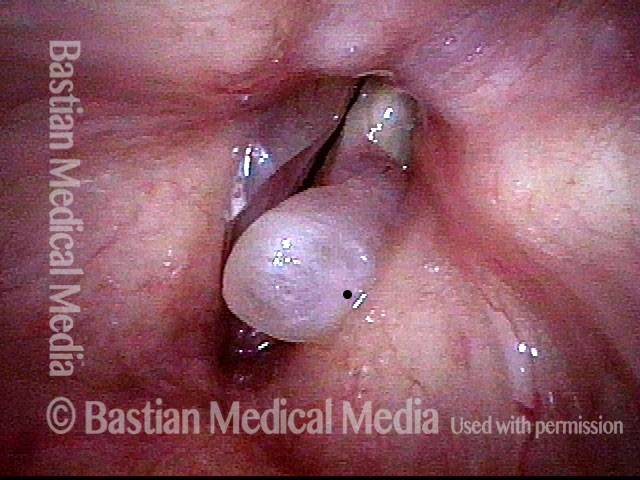
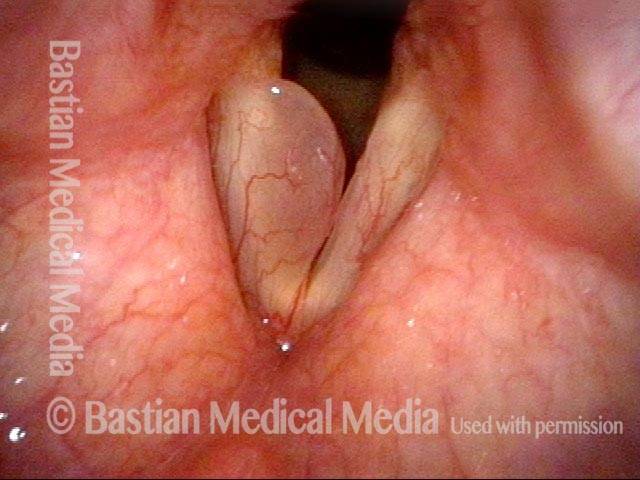
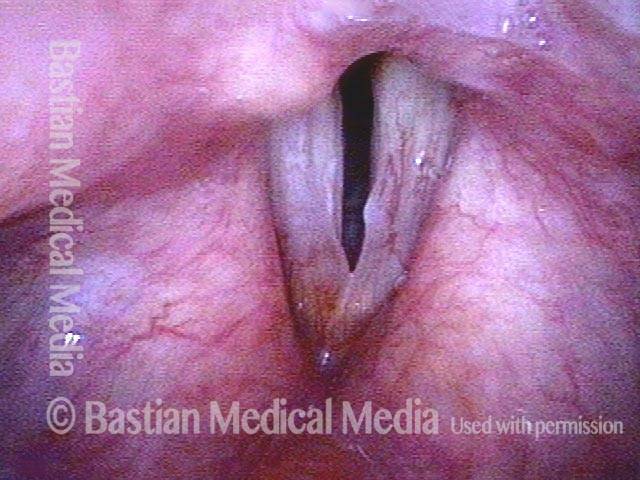
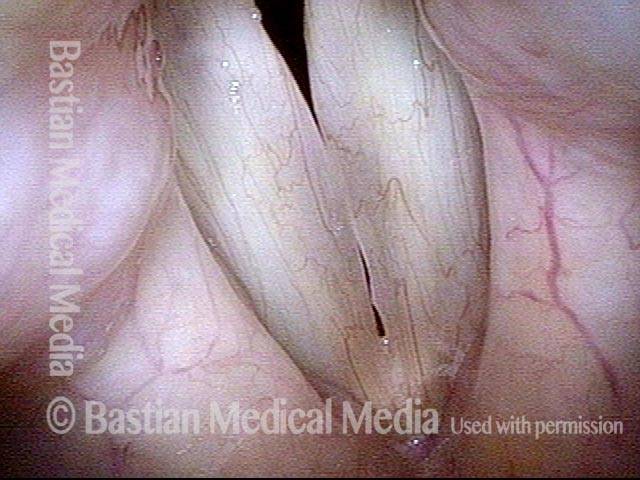
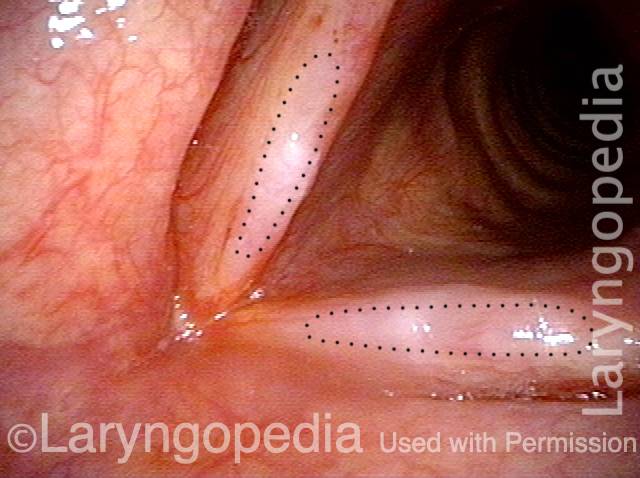
Smoker’s polyps, BEFORE surgery (2 of 4)
During inspiratory phonation: the polyps are drawn inward and are easier to see.
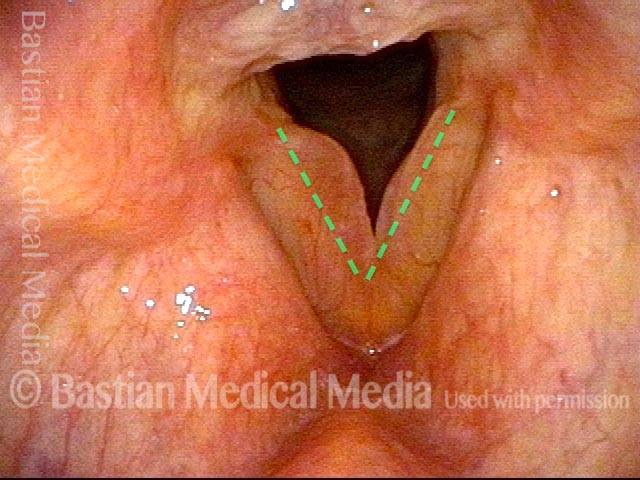
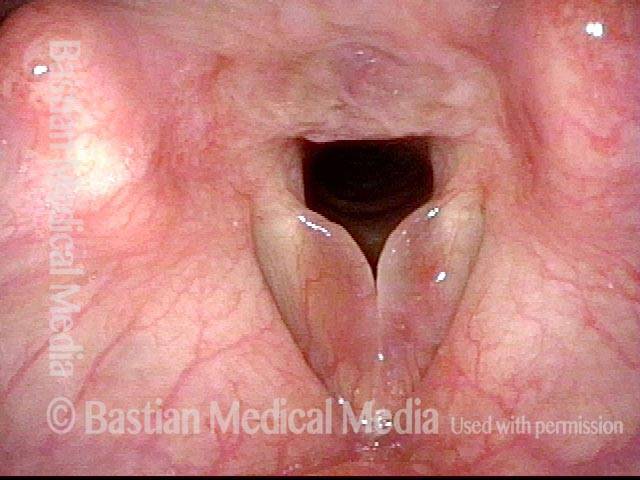
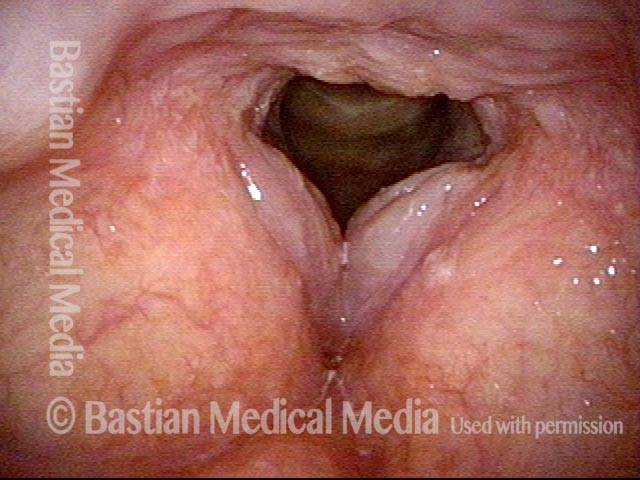
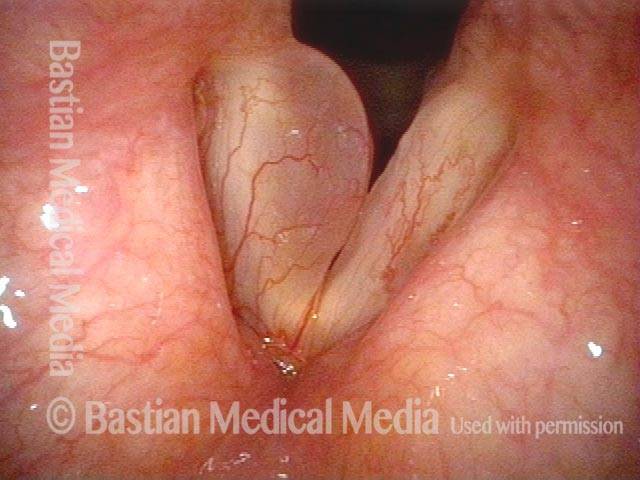
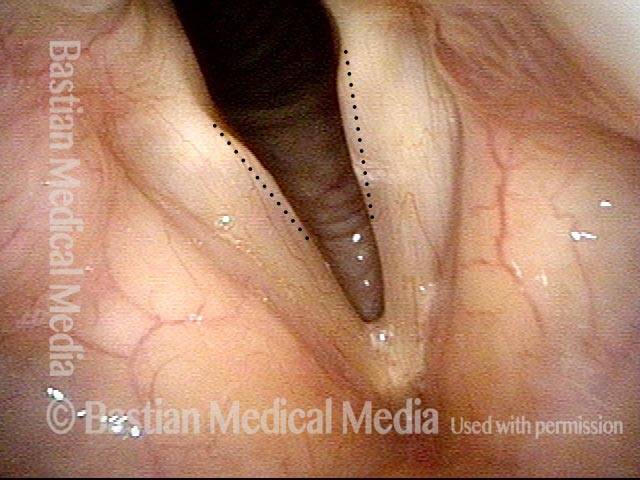
Smoker’s polyps, AFTER surgery (3 of 4)
Two months after surgery, during quiet breathing. The vocal cord margins are now straight.
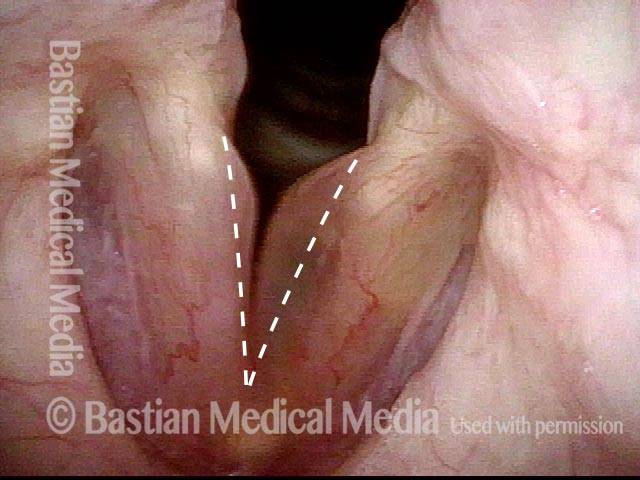
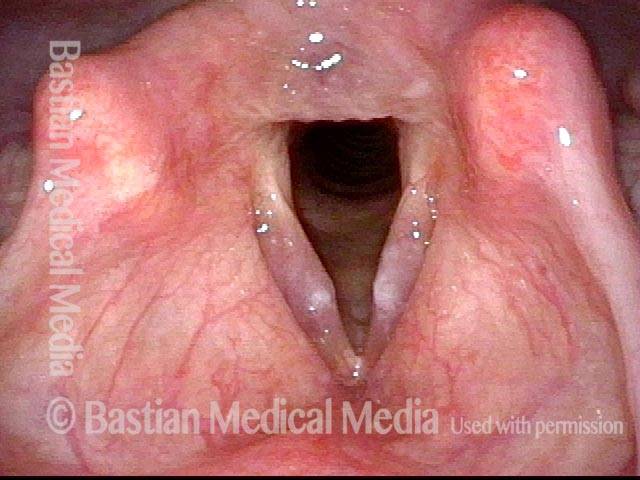
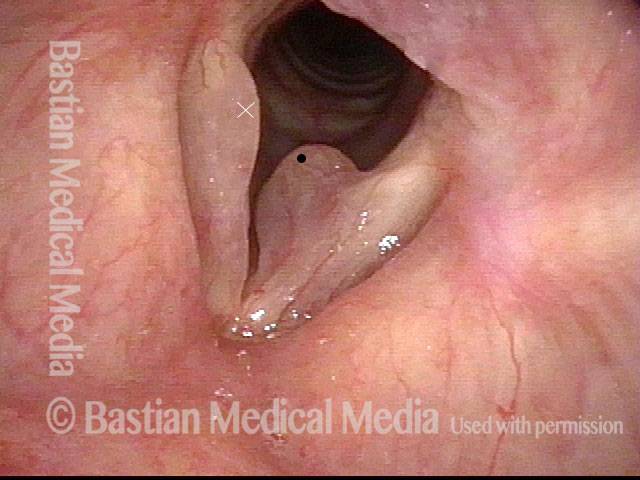
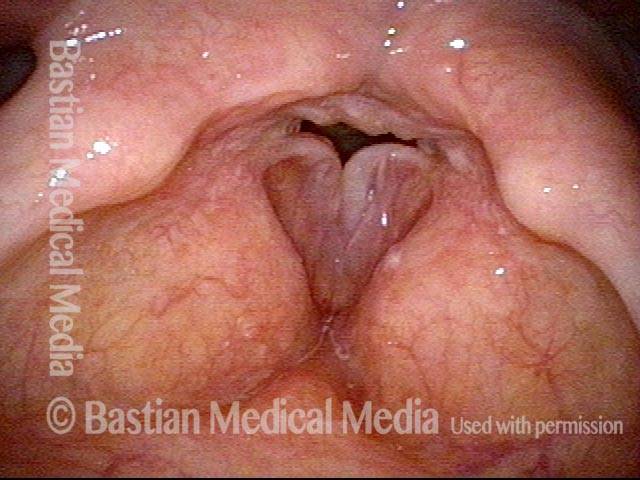
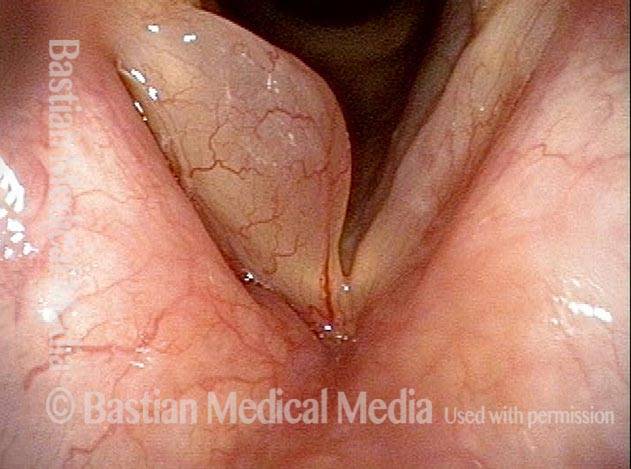
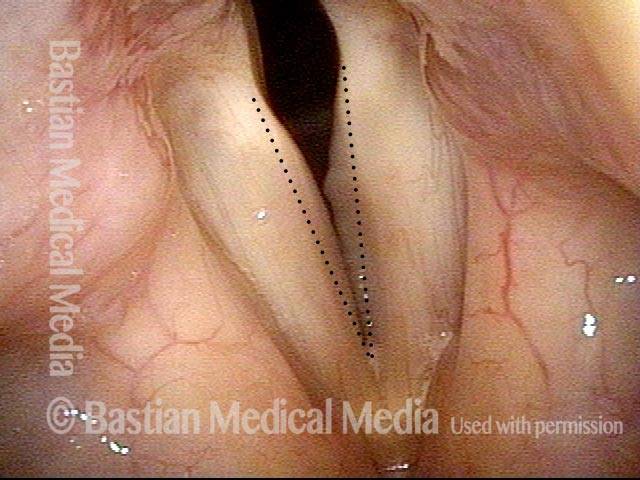
Smoker’s polyps, AFTER surgery (4 of 4)
During inspiratory phonation: the margins are drawn into a mildly convex contour, but far less than preoperatively. The patient’s voice is also much improved, albeit the occasional syllable dropouts due to recentness of surgery (listen to this patient’s voice samples in the audio section of the encyclopedia entry).
Polyp, smoker’s type
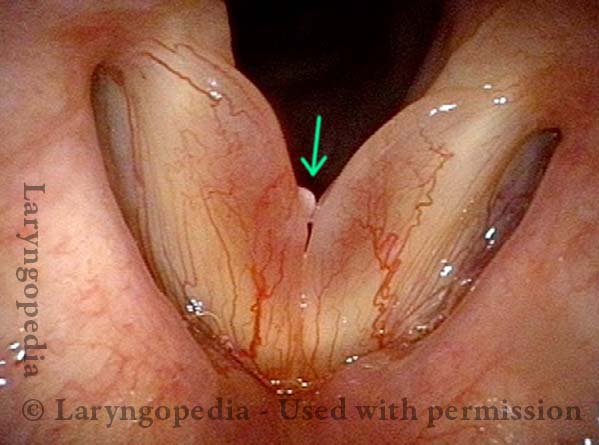
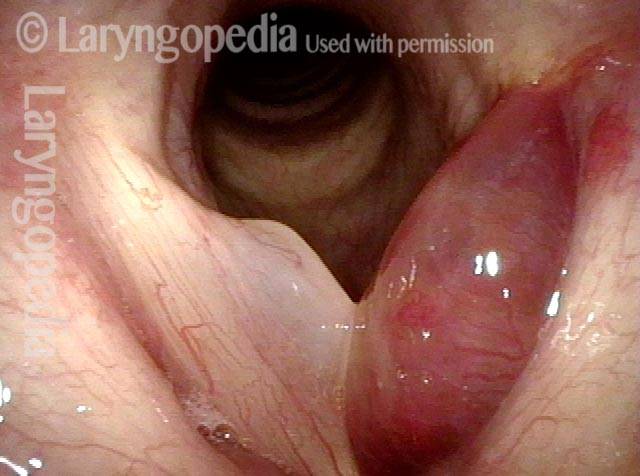
Reinke’s Edema (1 of 2)
Abducted position for breathing. Diffuse submucosal (Reinke’s) edema, along with more focal margin swelling especially on the right at arrow.

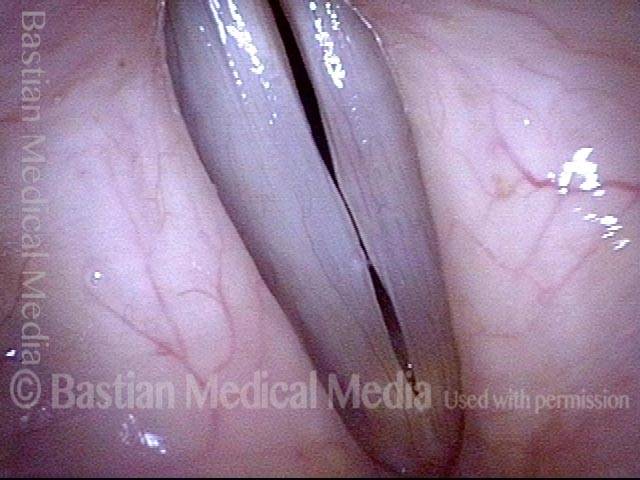
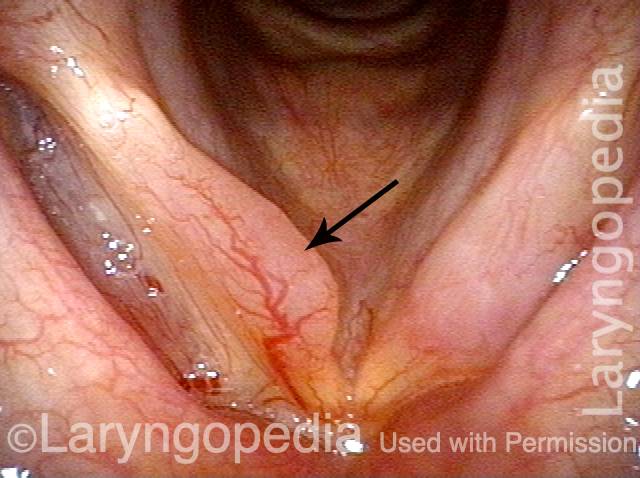
Convex margin (2 of 2)
Rapid inspiration in-draws the polyp to make the margin of the fold more convex as redundant tissue is drawn from the upper surface of the fold into the airway. For reference, the arrow again points to the focal margin swelling.
Polypoid Vocal Nodules
Polypoid vocal nodules (1 of 4)
Polypoid vocal nodules in a “vocal overdoer” with phenomenology typical for a mucosal injury. Narrow band illumination (blue-green light) makes vasculature more prominent. Note also the fusiform (long, low-profile) swelling, best seen on the left cord (right of image).

Incomplete closure (2 of 4)
Phonation, strobe light, at the beginning of the closed phase of vibration; one can see that closure will be incomplete due to early contact of the polypoid nodules.
Polypoid vocal nodules (3 of 4)
Phonation, strobe light, closed phase of vibration, with persistent gaps anterior and posterior to the polypoid nodules.
Polypoid vocal nodules (4 of 4)
Phonation, strobe light, open phase of vibration, continues to show the mid-cord swellings.

Smoker’s Polyps / Reinke’s Edema / Polypoid Degeneration
Smoker’s polyp / Reinke’s edema (1 of 2)
Quiet breathing, under standard light. The edematous mucosa is not yet evident.
Smoker’s polyp / Reinke’s edema (2 of 2)
Elicited inspiratory phonation in-draws and thereby reveals the edematous mucosa, greater on the right (left of image) than the left. The dashed lines indicate the normal location and contour of the vocal cords’ free margins.
Example 2
Smoker’s polyps / Reinke’s edema (1 of 3)
This patient is a long-term smoker, and also is talkative. Her voice has been gradually deepening for years. Here, with the vocal cords in abducted breathing position, one can only see somewhat underwhelming, broad-based, low-profile swelling, along with some hazy leukoplakia in the mid-cord.
Smoker’s polyps / Reinke’s edema (2 of 3)
Phonation. Again, there is only very low-profile, broad-based convexity of the margins, and again, the hazy leukoplakia in the mid-cords.
Smoker’s polyps / Reinke’s edema (3 of 3)
Elicited inspiratory phonation. Now, one can see that, contrary to the appearance in the prior two views, this patient in fact has moderate-sized “smoker’s-type” polyps, aka Reinke’s edema. The increased mass explains the virilization of the sound of this woman’s voice.
Smoker’s Polyps in Various “Poses”
Smoker’s polyps in various “poses” (1 of 4)
Vocal cord abduction for breathing, during expiratory phase. Left polyp (right of photo) appears to be the only finding. This is in a middle aged smoker with several years of gradually deepening / masculinized and now rough voice. The black dot and white “X” are reference points, facilitating comparisons with the other photos.
Polyp begins to fall off (2 of 4)
At the beginning of elicited rapid inspiration, showing the polyp beginning to be displaced from upper surface to the margin. That is, previously-unseen polypoid tissue (at ” X”) is now indrawing from upper surface of the right cord (left of photo) as well, and margin has become convex rather than straight as it was in photo 1.
Polyps displace (3 of 4)
The left-sided polyp (right of photo) is now displaced below the margin of that cord. The right polyp (left of photo) is now fully displaced/ indrawn to the margin of the right cord (left of photo).
Edematous tissue causes a rough voice (4 of 4)
During voice-making, most of the edematous tissue relocates back to the upper surface of the cords where it vibrates chaotically to add not only masculine but also rough voice quality.
Smoker’s Polyps with Leukoplakia
Long-term smoker (1 of 4)
A long-term smoker whose (female) voice has become deep and rough. Note the rounded (convex) vocal cord margins, “fat” vocal cords, and hazy leukoplakia. Interarytenoid pachyderma can be from acid reflux or chronic smoking.
Forced inspiration (2 of 4)
Forced inspiration sucks the excess polypoid tissue inward and reduces the space available for air to pass, explaining the harsh inspiratory noise one hears at the same time.
Closer view (3 of 4)
Closer visualization.

Rapid inspiration (4 of 4)
Rapid inspiration. The demarcation of the leukoplakia is seen well here.
Smoker’s Polyps and Thulium Laser
Pre-laser surgery, respiration (1 of 12)
During respiration, showing the large right vocal cord (left of photo) smoker’s-type polyp. The voice is accordingly deep, rough, and effortful to produce.
Pre-laser surgery, onset of phonation (2 of 12)
Onset of phonation, with vibratory blurring, and showing the mismatch of the cords.
Pre-laser surgery (3 of 12)
Just before starting laser treatment, in-drawing of large right vocal cord polyp (left of photo).
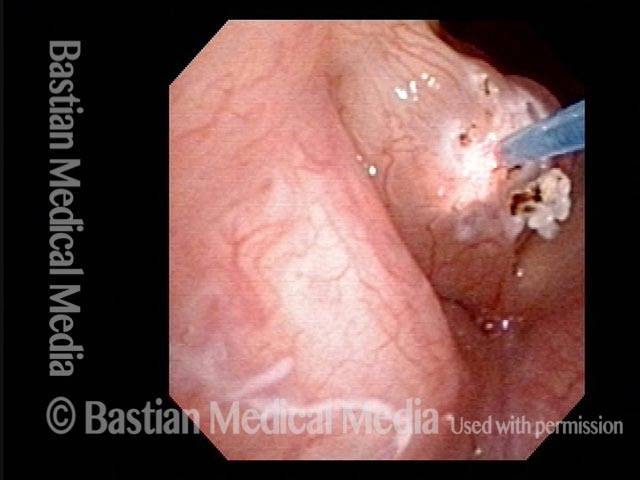
During laser surgery (4 of 12)
Mostly contact mode Thulium laser treatment. The glass fiber is piercing the polyp to deliver laser energy to the gelatinous content of the polyp.
Post surgery, 28 days later (5 of 12)
28 days later, the upper 2/3 of this gelatinous polyp has sloughed away, but the portion on the free margin “escaped,” and remains visible.

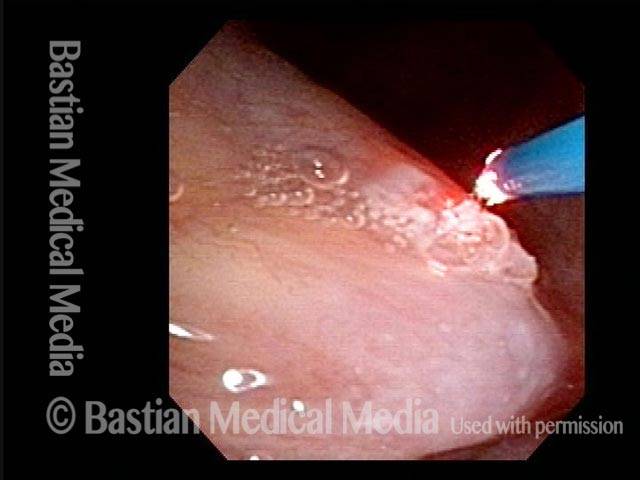
Second laser surgery (6 of 12)
A second Thulium laser treatment of the residual polyp.
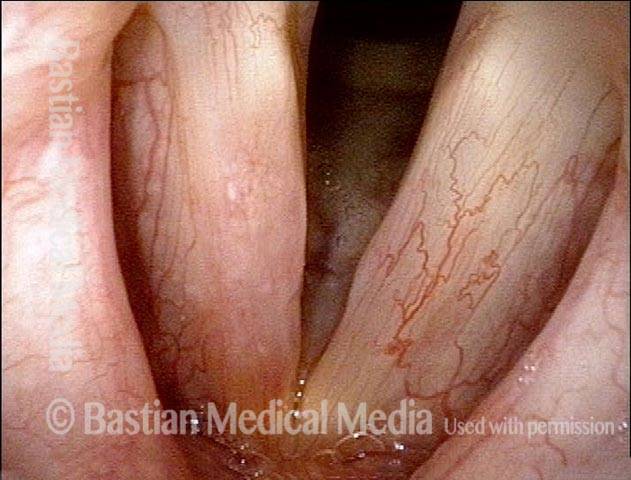
Post surgery, 21 days later (7 of 12)
Twenty-one days after second laser treatment , the polyp is no longer seen. Voice is dramatically improved from the time of original evaluation. Mild right vocal cord (left of photo) inflammatory changes remain, as expected.
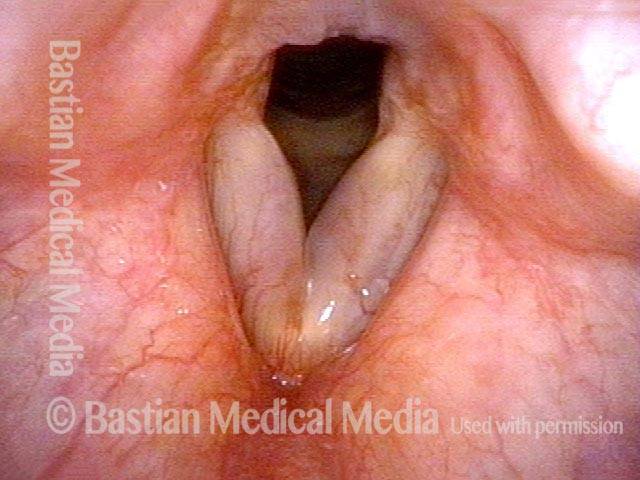
Post surgery, in-drawing of vocal cords (8 of 12)
At same examination, after asking the patient to produce inspiratory phonation, notice the indrawing of both vocal cord margins, consistent with mild residual Reinke’s edema.

Post surgery, one year later (9 of 12)
One year later. Voice remains excellent.
Post surgery, residual Reinke’s edema (10 of 12)
With inspiratory phonation, the patient is able to in-draw to a convex vocal cord margin bilaterally, again indicating residual Reinke’s edema.

Post surgery, closed phase of vibration (11 of 12)
Strobe light: mostly closed phase of vibration.
Post surgery, open phase of vibration (12 of 12)
Strobe light: open phase of vibration, showing good oscillatory flexibility of both cords.
Reinke’s edema (smoking-related) and how to see it
Convexed vocal cords (1 of 4)
Abducted, breathing position. Note that the margin of both vocal cords is slightly convex. See dotted line for normal, perfectly straight margin.
Inspiratory phonation (2 of 4)
Inspiratory phonation in-draws the mild Reinke’s edema (smoker’s type polyp formation).
Open phase, faint translucency (3 of 4)
Strobe illumination, at E4 (approximately 330 Hz), mostly open phase.
Closed phase, faint translucency (4 of 4)
Note again in closed phase.
Smoker’s Polyps with Two Explanations for Bruising
Bruising of left vocal cord (1 of 4)
With a 40-year smoking history, this woman has a masculine voice quality. She is often called “sir” on the phone by people who don’t know her. Note her large smoker’s polyps. The left vocal cord (right of photo) has suffered a recent bruise. As a quiet person, the explanation for her bruise may not be due to vocal overuse, but may be due in part to her use of aspirin.
A year later (2 of 4)
A year later, she returns for re-examination. The bruising has resolved. However, the convex margins and translucence remain. Note the large ectatic capillaries, that may have (along with aspirin) increased vulnerability to the bruising that happened a year earlier (see photo 1).

Inspiratory phonation (3 of 4)
The elicitation of inspiratory phonation makes the left-sided polyp (right of photo) even more obvious.

Translucent polyp, different view (4 of 4)
A different inspiratory view sucks the left polyp (right of photo) underneath the right (left of photo), and now the right-sided more translucent polyp (left of photo) is more obvious.

Smoker’s Polyp Reduction Improves Voice Even Though the Larynx Result May not be “Pretty”
Smokers Polyp (1 of 5)
Six years after vocal polyp removal elsewhere. As a result of continued smoking, the voice is deep and rough, and an obvious recurrent/residual “smoker’s” polyp is seen on the right vocal cord(arrow, left of photo). The patient “hates” her rough and masculine voice quality.
Reine’s edema (2 of 5)
Inspiratory phonation is elicited to “pull” the redundant tissue medially, revealing a lot of Reine’s edema of the left vocal cord, too. The dotted lines show the ellipse of mucosa that will be removed during surgery. Mucose will be preserved at the margins and the gelatinous lateral within the polyps will be suctioned away if liquid, and dissected away if fibrotic.
A week after surgery (3 of 5)
The dotted lines show the extent of mucosal excision—an area that will take a few weeks to re-mucosalize. Since this was a polyp “reduction,” though hoarse this early post, she has a ” functional” voice. There should be no alarm if patients are aphonic for a week or even a few weeks while inflammation resolves.
Residual Reinke’s edema (4 of 5)
At two months post, the patient is very pleased and says the improvement to voice is “large.” Here, it appears there may be some residual Reinke’s edema especially of the left vocal cord (right of photo) judging by the slightly convex margin.

Residual submucosal edema (5 of 5)
With inspiratory phonation, the residual submucosal edema is made obvious, especially on the left. This was (as intended) a polyp “reduction” approach, rather than polyp “removal” as the latter is too hard on voice, and it is not possible to “put back” if too much tissue is taken. Here, there is no stiffness, and if desired, more can be removed. Of course, since the patient is so pleased with her voice, no further treatment is needed.