Posterior commissuroplasty is an endoscopic procedure performed for individuals who have difficulty breathing, due to either bilateral vocal cord paralysis or bilateral vocal cord fixation. These individuals’ vocal cords are immobile or fixed in a mostly closed position, which inhibits breathing and often causes noisy inspiration.
In a posterior commissuroplasty, the clinician uses a carbon dioxide laser to take small divots from the posterior ends (membranous glottis) of both vocal cords. These divots create more space between the cords so that, during breathing, air can pass through more easily. This procedure can avoid the need for a tracheotomy. It also preserves the voice’s functionality better than a transverse cordotomy typically does.
Office-Based Surgery When General Anesthesia Is too Risky
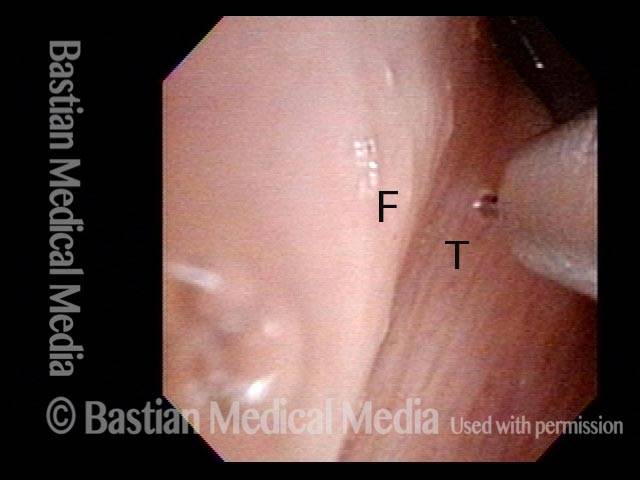
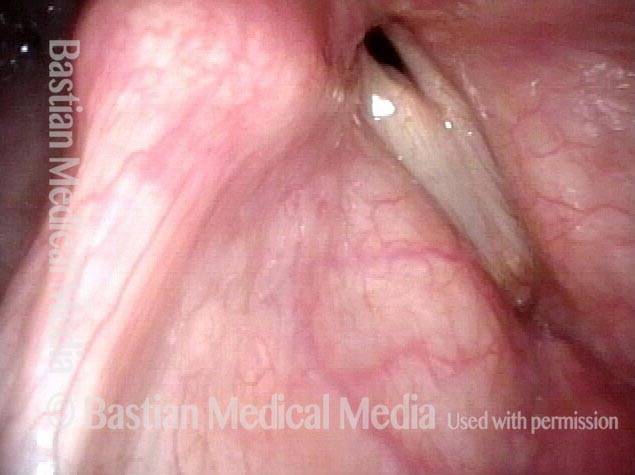
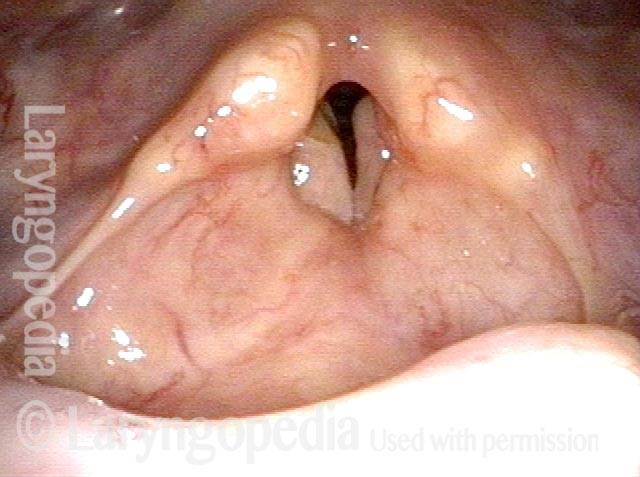
Involuntary inspiratory voice (1 of 6)

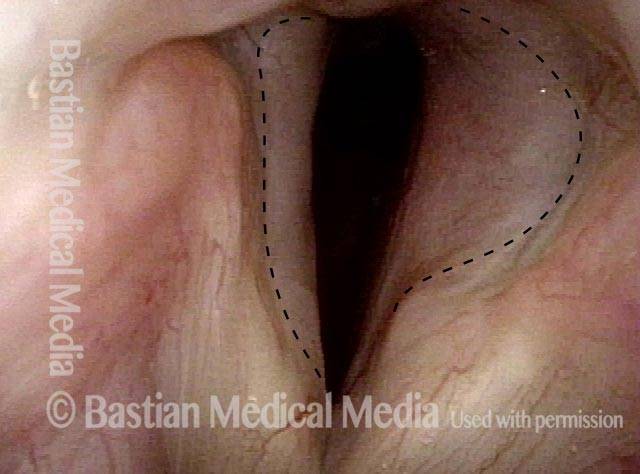
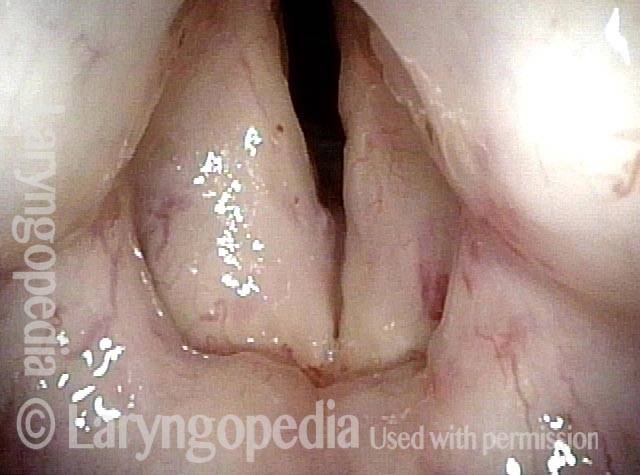
Laser posterior commissuroplasty (2 of 6)
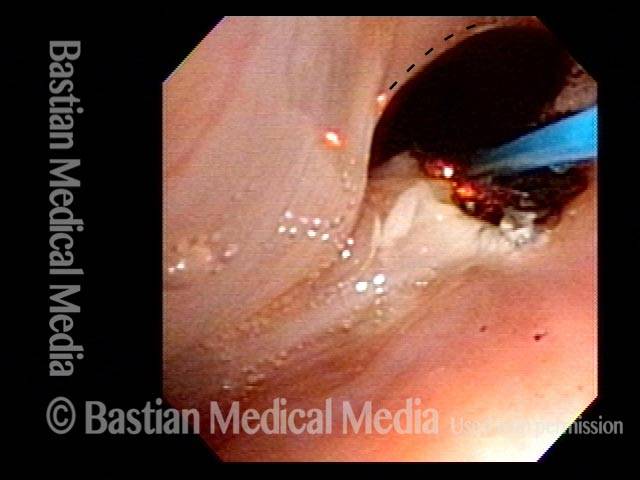
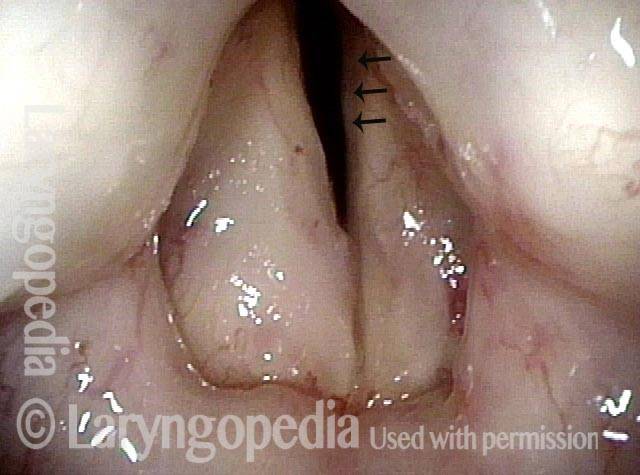
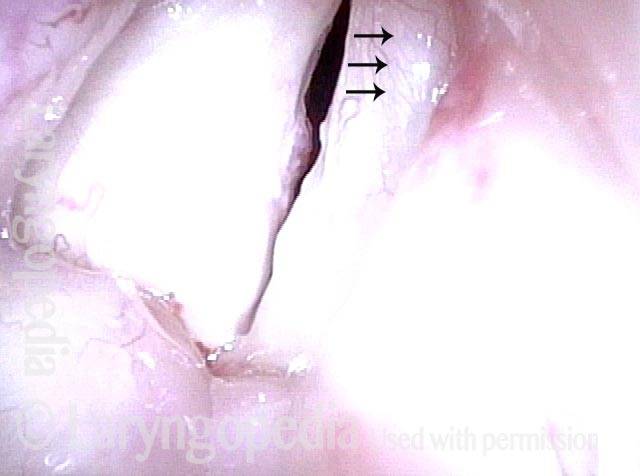
During the commissuroplasty (3 of 6)
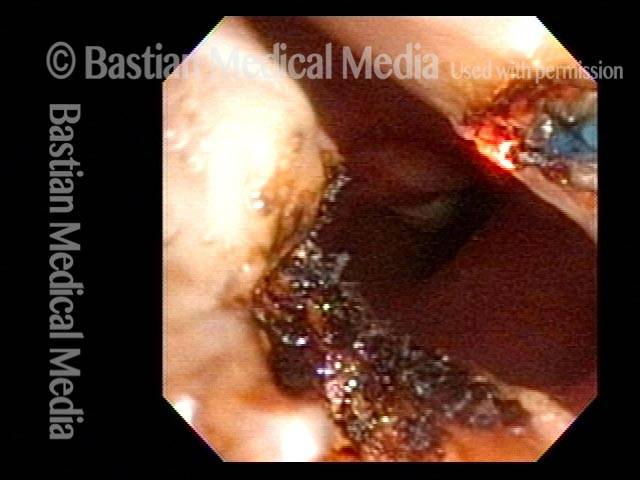
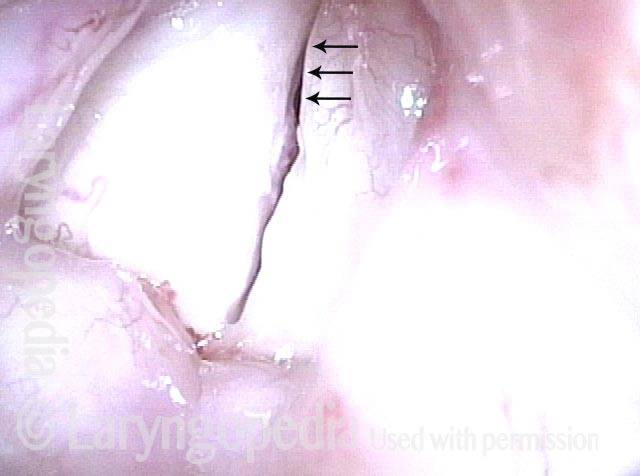
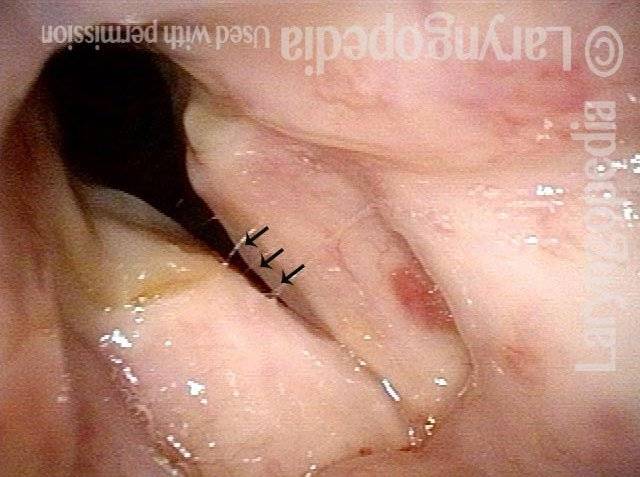
Deepening divot (4 of 6)
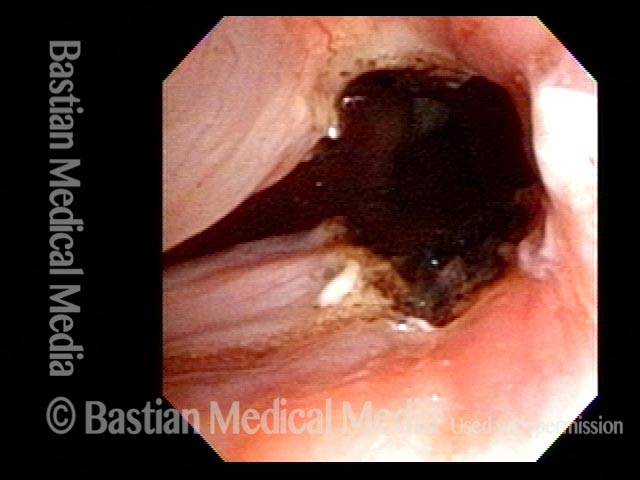
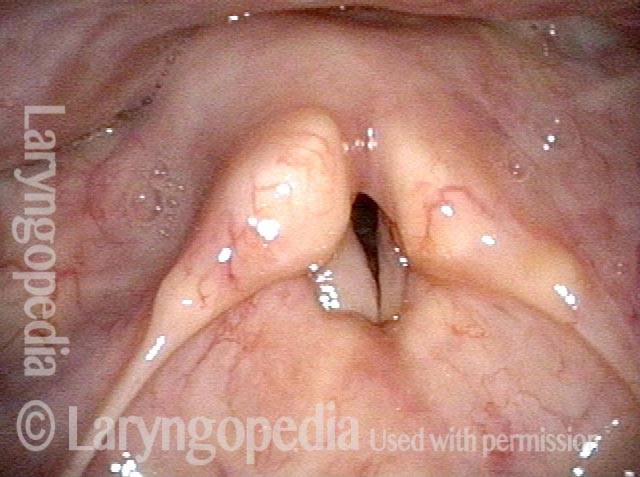
Inspiratory indrawing decreased (5 of 6)
Phonation (6 of 6)
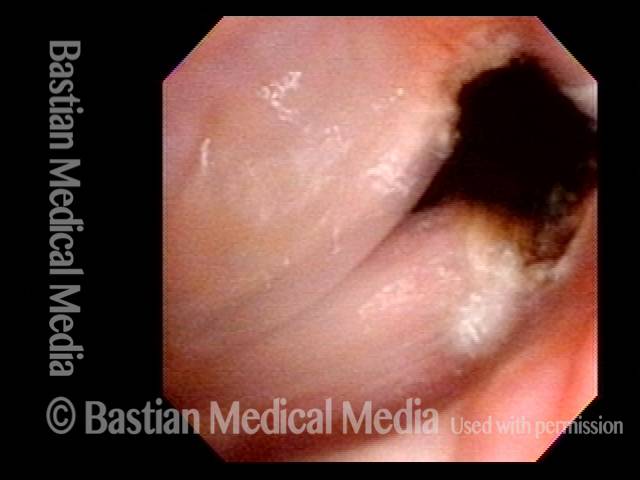
Sometimes you DO Remove Granulation to Avoid Tracheotomy
Granulation (1 of 8)

Closer view (2 of 8)

Post microlaryngoscopies (3 of 8)

Scarring (4 of 8)
Post posterior commissuroplasty (5 of 8)
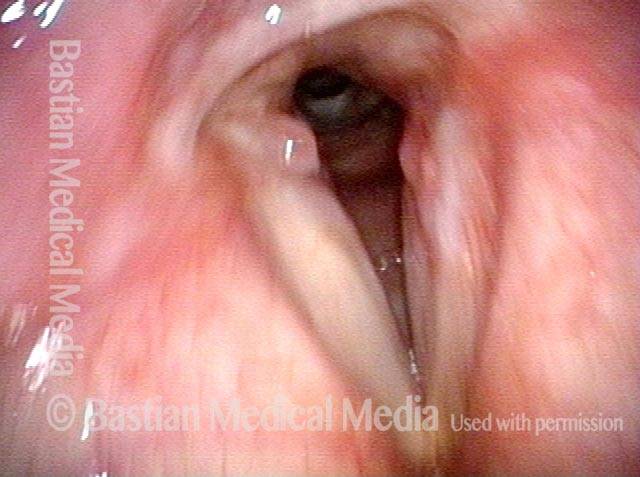
Breathing improved (6 of 8)
Closer view (7 of 8)

Phonatory view (8 of 8)
Progressive Radiation Fibrosis Effects on the Larynx and a Solution to some of It
Forty years post-radiation (1 of 8)
Involuntary inspiratory voice (2 of 8)
Only capable of high pitch (3 of 8)
Open phase vibration (4 of 8)
One week post-commissuroplasty (5 of 8)
Rapid inhalation, closer view (6 of 8)
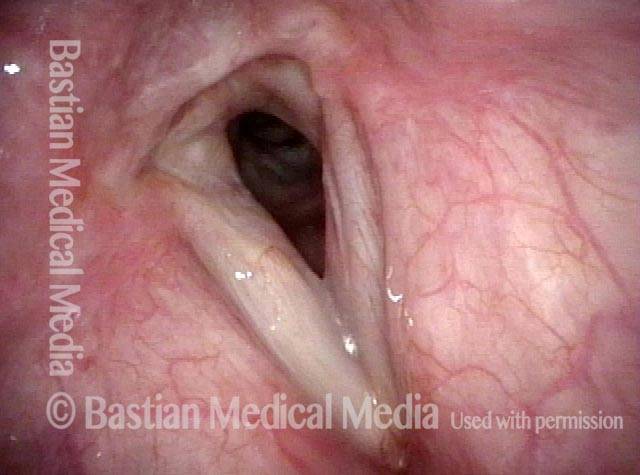
Three months post-surgery (7 of 8)
Closer view, post-surgery (8 of 8)
