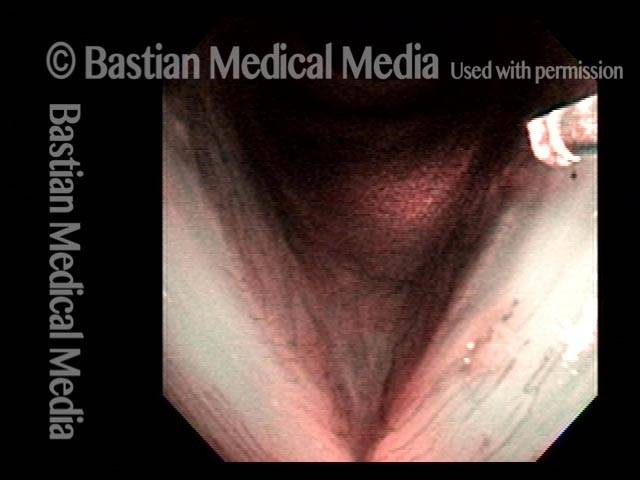
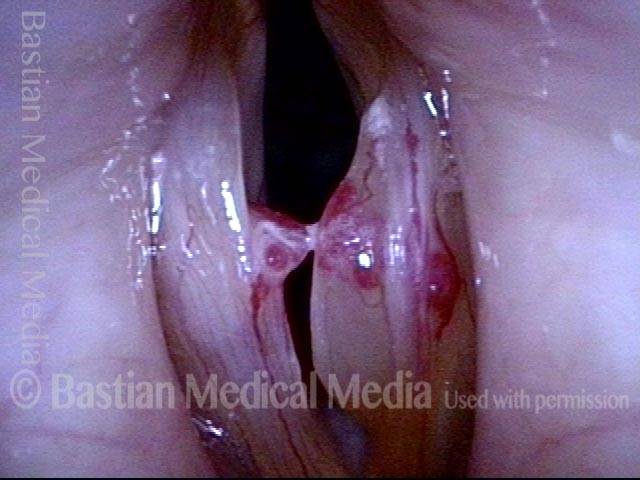
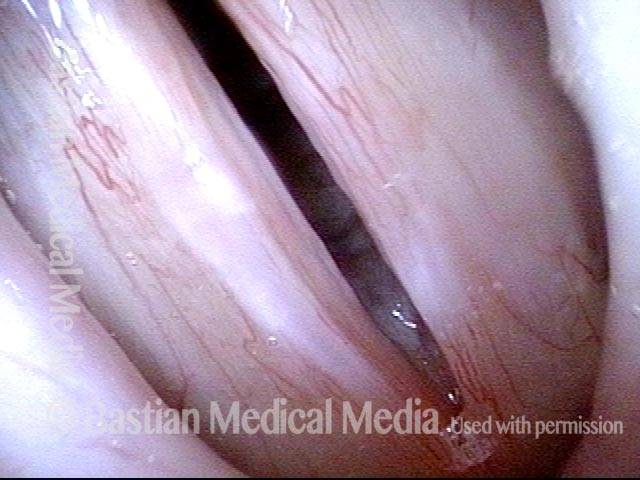
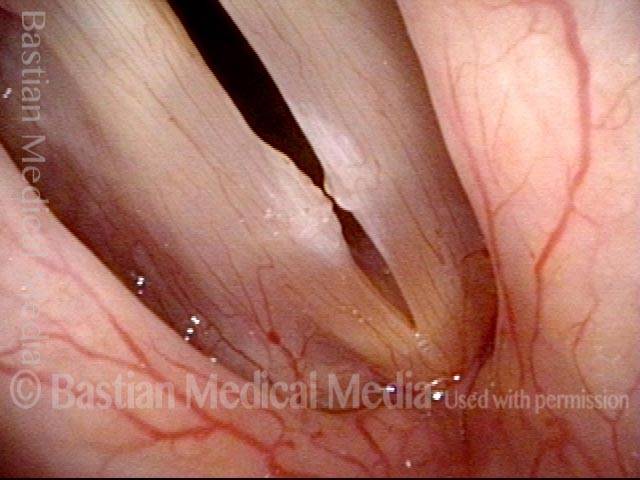
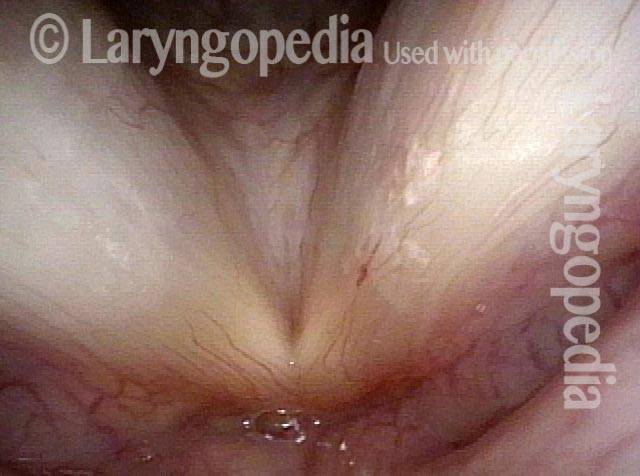
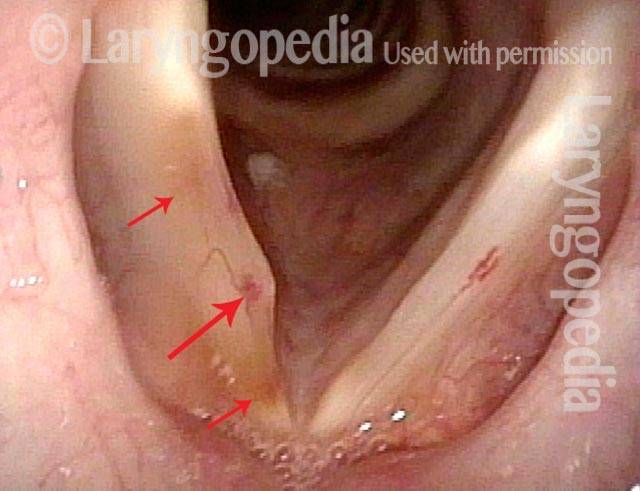
Vocal Cord Bruises (Hemorrhage) often Initially Obscure the Ectatic Capillary “Culprit”
A person can experience sudden hoarseness at a time of sustained heavy voice use, or even immediately following a “scream,” or even a loud sneeze. The explanation might be a bruise of a vocal cord. This can happen to anyone but is far more likely if the person has underlying capillary ectasia.
When a bruised vocal cord is seen, therefore, the question is: “Is this a fluke bruise that can happen to anyone, or is it one explained by capillary ectasia?” In this instance, the answer is “yes.”
Singer’s Bruised Vocal Cord (1 of 8)

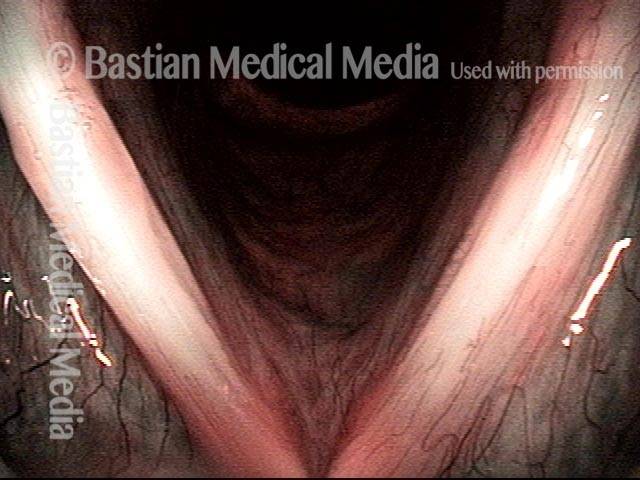
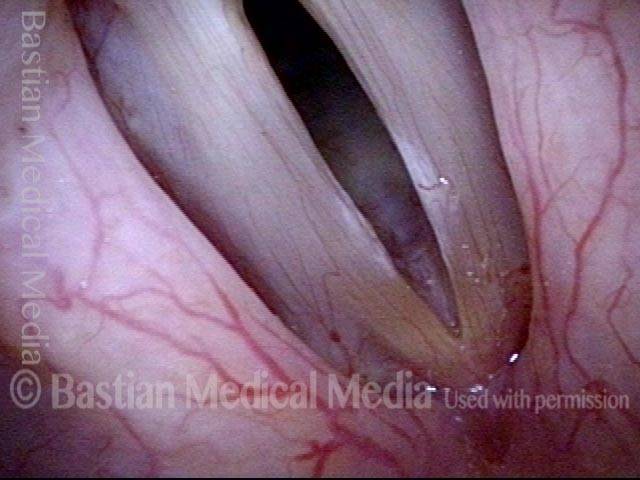
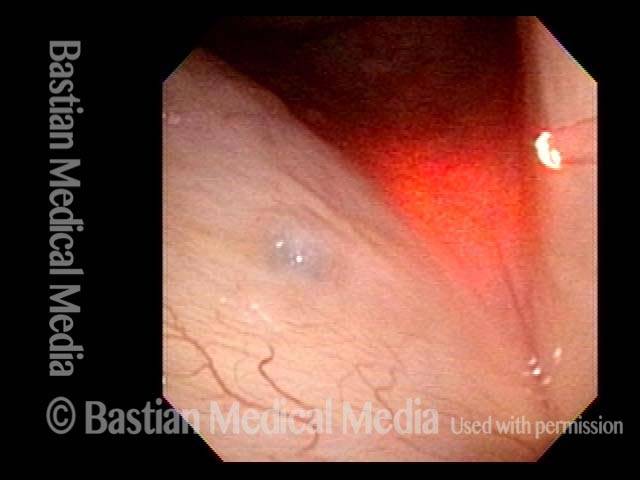
Bruise under Strobe Light (2 of 8)

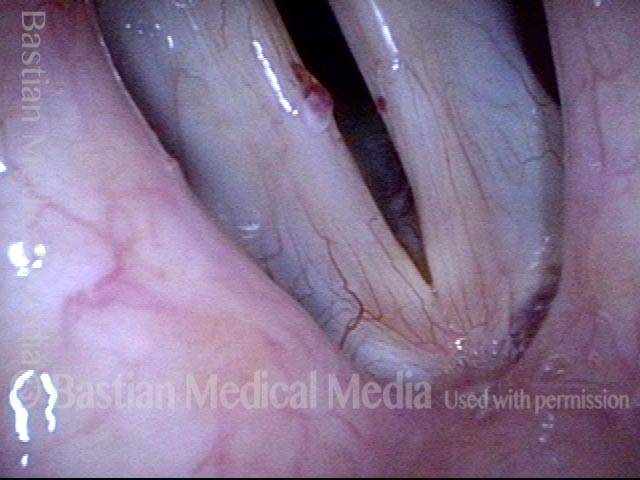
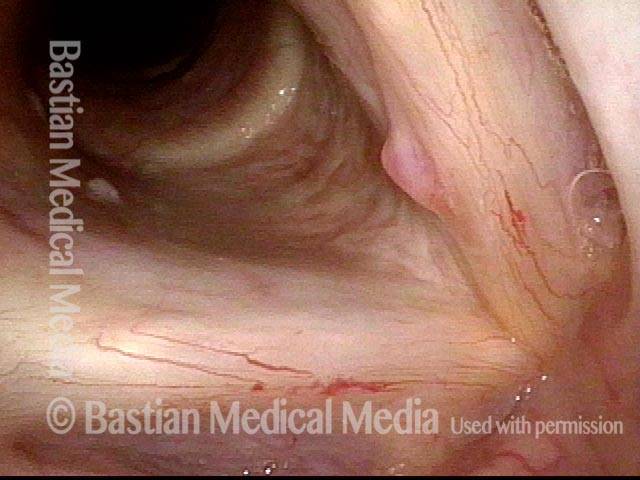
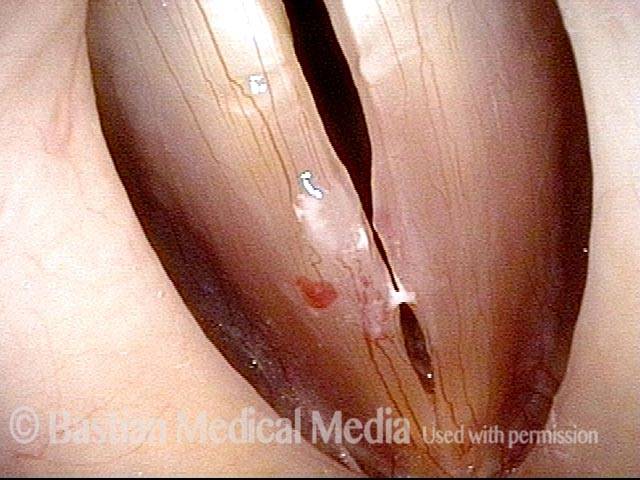
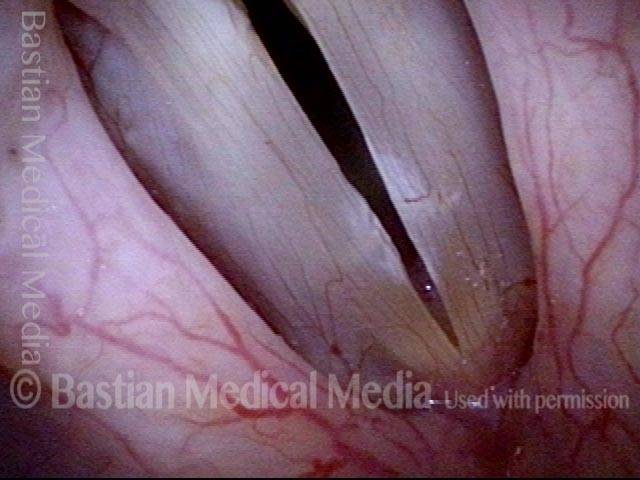
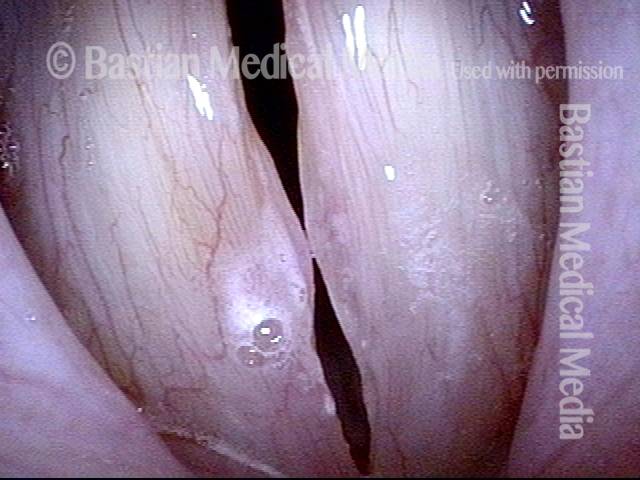
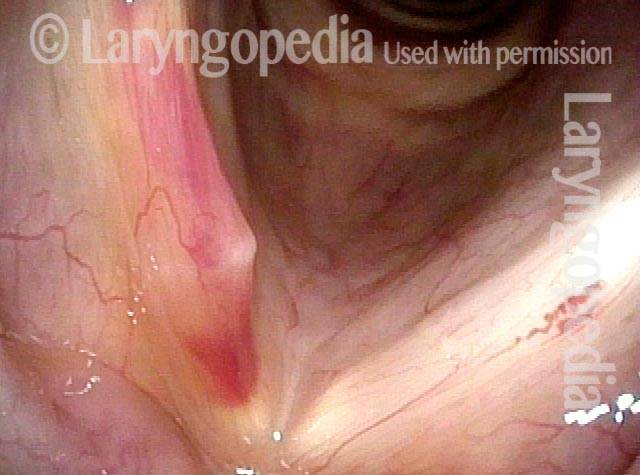
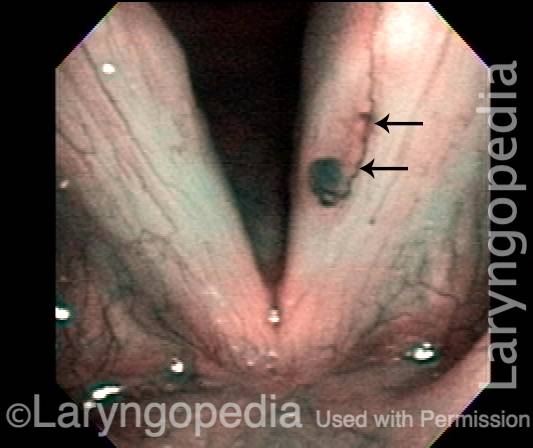
Abnormal capillary (3 of 8)

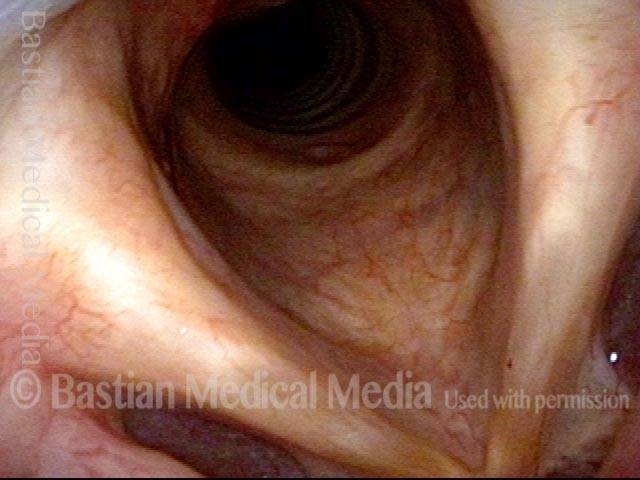
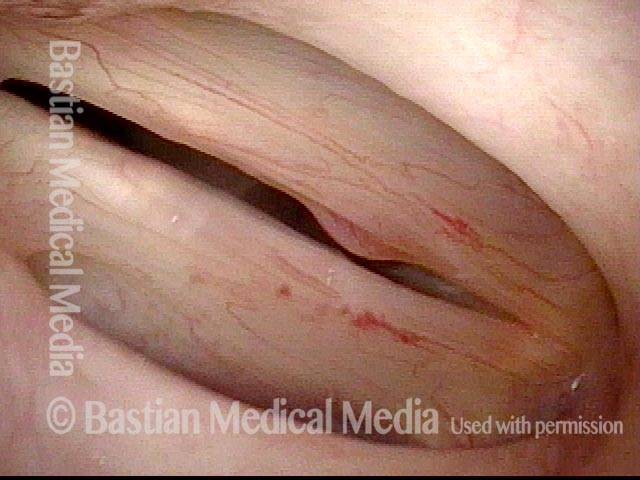
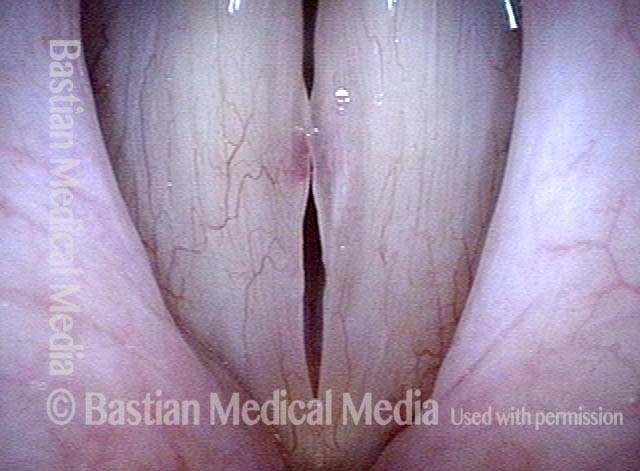
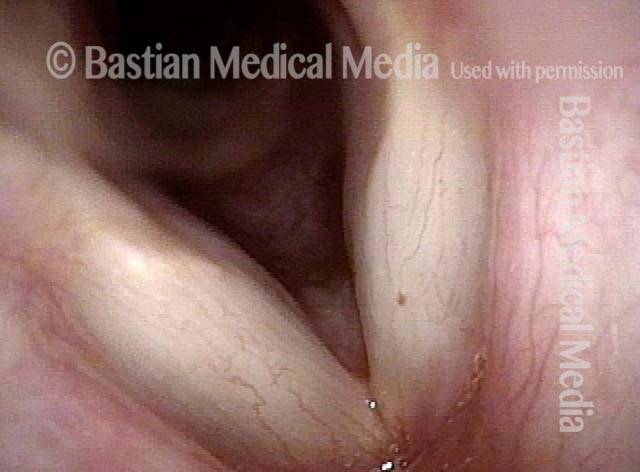
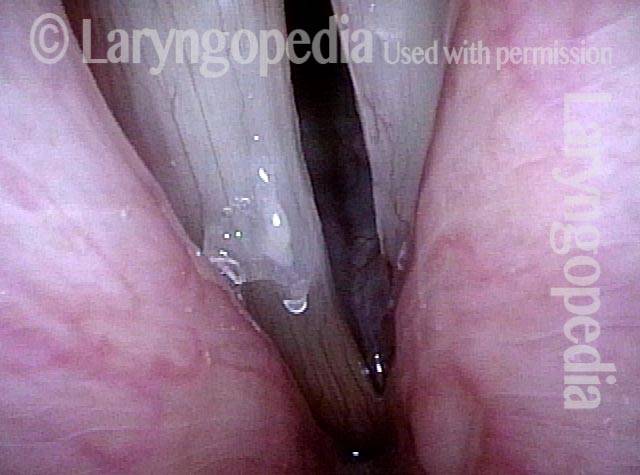
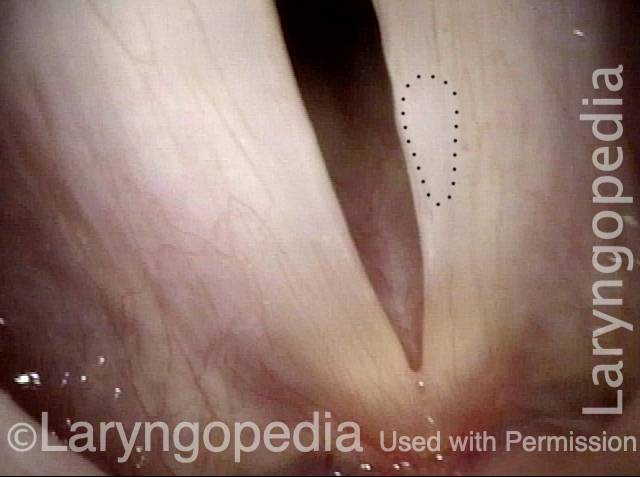
Bruise is gone (4 of 8)

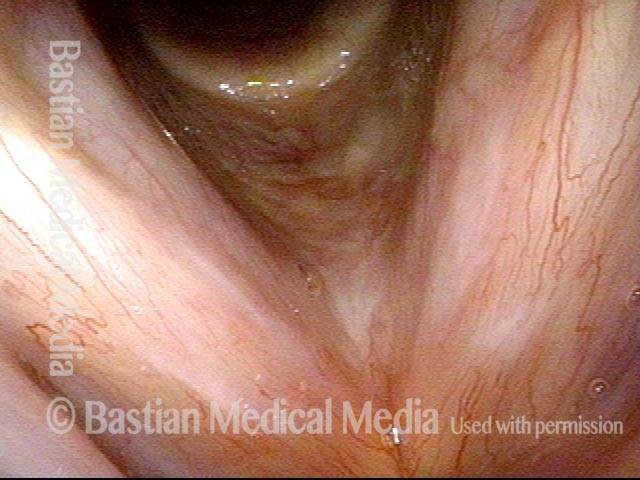
Capillaries under narrow band light (5 of 8)

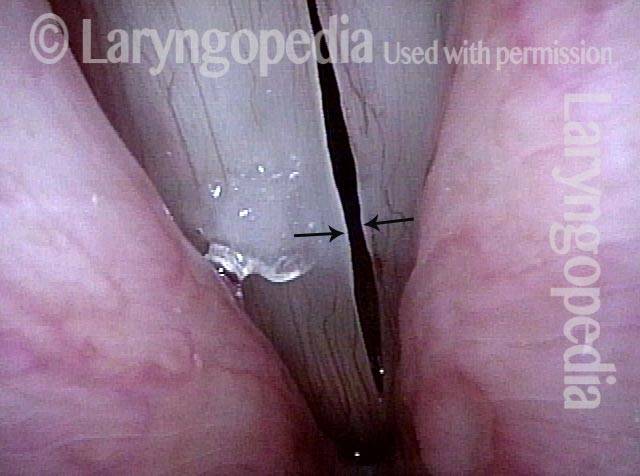
Capillaries touch during phonation (6 of 8)

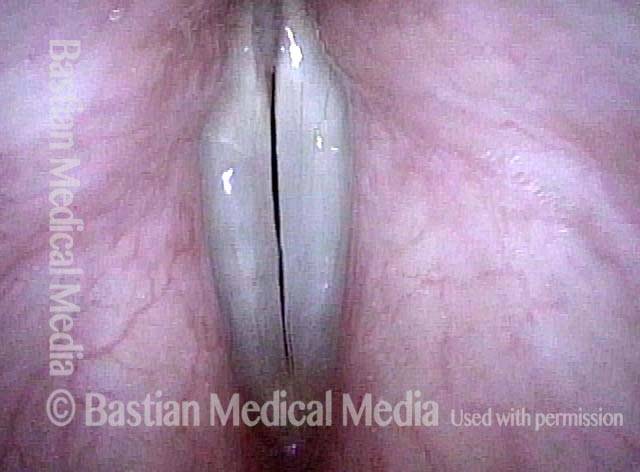
Post-surgical repair (7 of 8)

Margins match (8 of 8)

Capillary Ectasia, Before and After Laser Coagulation
Capillary ectasia (1 of 7)

Capillary ectasia (2 of 7)

Capillary ectasia (3 of 7)
Closed phase (4 of 7)
Capillary ectasia, after laser coagulation (5 of 7)

Capillary ectasia, after laser coagulation (6 of 7)

After laser coagulation (7 of 7)

Example 2
Capillary ectasia (1 of 3)
Capillary ectasia, right after laser coagulation (2 of 3)
Capillary ectasia, 6 weeks after laser coagulation (3 of 3)
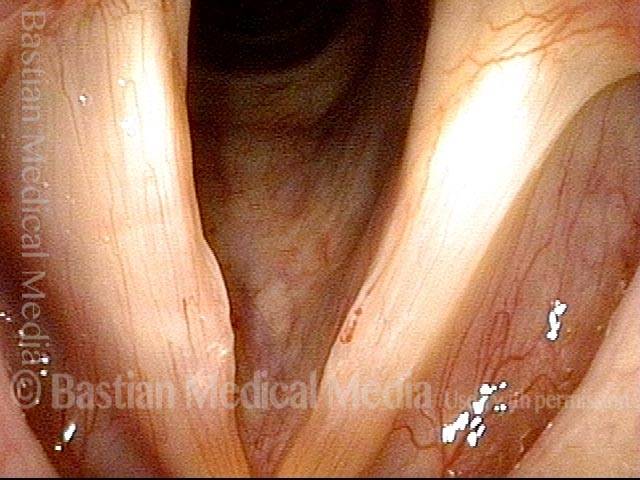
A Vocal Cord Bruise That Could Happen To Anyone
While capillary ectasia (as seen in other photo series here) markedly increases vulnerability to vocal cord bruising, every human vocal cord has capillaries on its service, and even normal capillaries can leak and cause a bruise with sufficient vocal trauma. In this person, with an aggressive cough, her normal capillaries are the source of the bruise.
Bruised Vocal Cord (1 of 2)

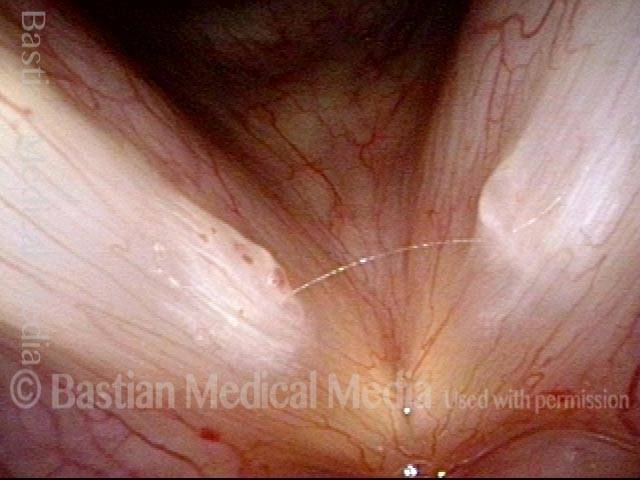
Bruised Vocal Cord (2 of 2)

Capillary Ectasia and Hemorrhagic Polyp, Before and After Treatment
Capillary ectasia and hemorrhagic polyp (1 of 4)
Capillary ectasia and hemorrhagic polyp (2 of 4)

Capillary ectasia and hemorrhagic polyp, after treatment (3 of 4)
Capillary ectasia and hemorrhagic polyp, after treatment (4 of 4)

Capillary Ectasia and Hemorrhagic Polyp
Capillary ectasia and hemorrhagic polyp (1 of 2)

Capillary ectasia and hemorrhagic polyp (2 of 2)
Capillary Ectasia and Hemorrhagic Polyp, Treated by Thulium Laser
Capillary ectasia and hemorrhagic polyp (1 of 7)
Capillary ectasia and hemorrhagic polyp (2 of 7)
Capillary ectasia and hemorrhagic polyp, thulium laser treatment (3 of 7)

Capillary ectasia and hemorrhagic polyp, thulium laser treatment (4 of 7)

Capillary ectasia and hemorrhagic polyp, after treatment (5 of 7)
Vocal cord margin (6 of 7)

Capillary ectasia and hemorrhagic polyp, after treatment (7 of 7)
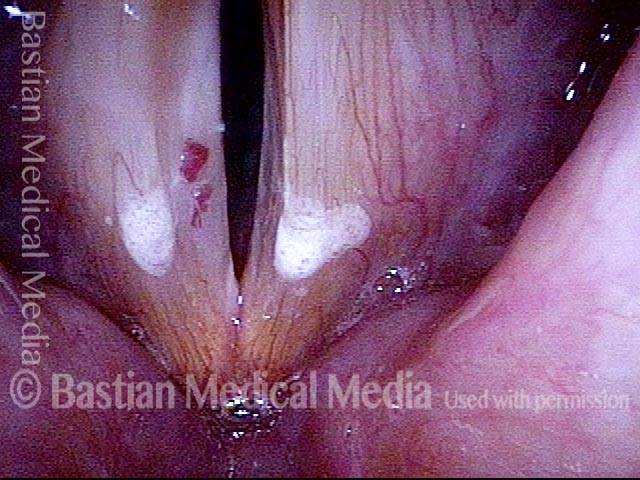
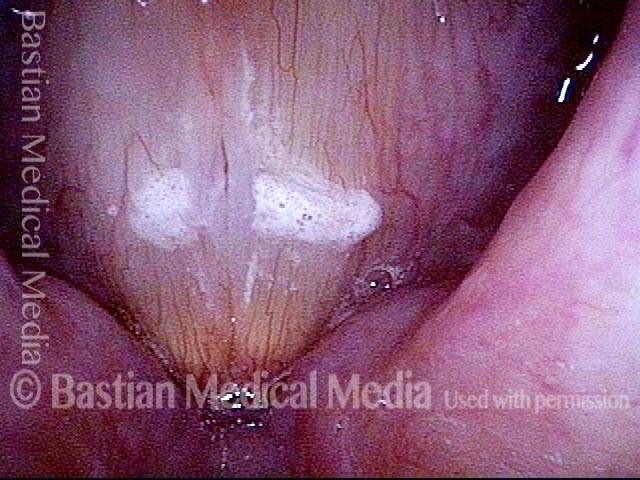
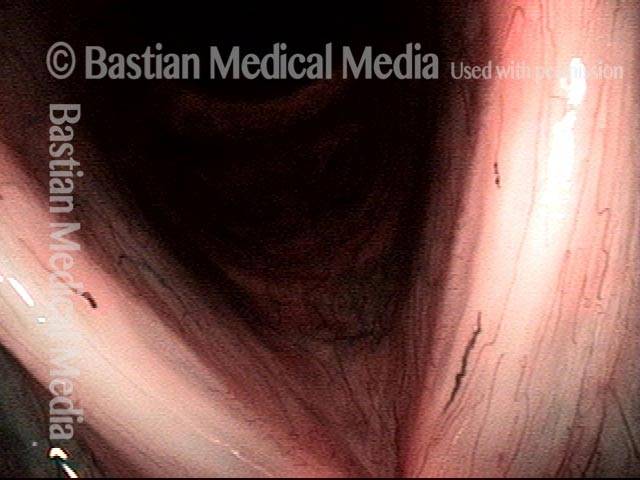
Capillary Ectasia with Vocal Nodules
Capillary ectasia with vocal nodules (1 of 2)

Capillary ectasia with vocal nodules (2 of 2)
Example 2
Capillary ectasia with vocal nodules (1 of 3)
Capillary ectasia with vocal nodules (2 of 3)

Capillary ectasia with vocal nodules (3 of 3)

Vocal Nodules, Leukoplakia, and Capillary Ectasia
Vocal nodules, leukoplakia, and capillary ectasia (1 of 4)
Vocal nodules, leukoplakia, and capillary ectasia (2 of 4)
Vocal nodules, leukoplakia, and capillary ectasia: 6 months later (3 of 4)
Vocal nodules, leukoplakia, and capillary ectasia: 6 months later (4 of 4)
Capillary Lake and KTP
Capillary lake (1 of 8)

Mucosal fatigue (2 of 8)
Prep for laser coagulation (3 of 8)

KTP laser coagulation (4 of 8)

Post laser ablation (5 of 8)
Post laser ablation, distant view (6 of 8)

After a weekend of vocal overuse (7 of 8)
Capillary (8 of 8)

Choral Singer’s Voice Fully Restored
Hoarse choral singer (1 of 4)

Residual bruising (2 of 4)

2 months post-surgery (3 of 4)
Margins match (4 of 4)
Red Herring Capillary Ectasia and Mucosal Injuries
Ectatic capillary (1 of 4)
Ectatic capillary, narrow band light (2 of 4)

Margin swelling (3 of 4)
Bowing, atrophy, and flaccidity (4 of 4)
Ask Both Voice (via vocal phenomenology) and Larynx (via a motivated examination) to Give up their Secrets
Obvious mucosal injury (1 of 3)

Vocal nodules (2 of 3)

Capillary ectasia (3 of 3)

The Evolution of Vocal Cord Bruising and Emergence of a Vulnerable Capillary
Margin swelling and bruising (1 of 2)
Six weeks later (2 of 2)
Pulsed KTP Laser Treatment of Vascular Abnormalities in a Singer
Ectatic capillary (1 of 7)

Polyp (2 of 7)

Feeding capillary (3 of 7)
Glass fiber (4 of 7)

At the conclusion of the laser procedure (5 of 7)

Blanched area (6 of 7)
Polyp is gone (7 of 7)