CPM Procedure
CPM is accomplished under general anesthesia, in one of two ways: The preferred, newer methodology, is performed endoscopically. Using this method, a hollow, lighted “tube”—called an esophagoscope—is inserted into the throat and upper esophagus to examine the area and plan the next step. Then, a special laser scope is placed in the upper esophagus. A microscope permits a magnified, brightly-lit view of the offending ring of muscle.
The laser is used to divide the muscle and break its “grip.” If a Zenker’s sac is apparent, it is “marsupialized,” which means that its opening is widened in order to be sure the sac doesn’t retain food, but instead empties its contents directly into the esophagus.
Depending upon patient and surgical issues, a suction drain may be placed within the upper esophagus and brought out through the nose. A second small tube for feeding may also be placed through the nose, and down into the stomach. When placed, both tubes are removed the morning following surgery.
If a clear view cannot be achieved during esophagoscopy due to difficult patient anatomy (e.g., jaws won’t open well, small lower jaw, short neck, large upper teeth), then we return to a more traditional approach through an incision on the lower left neck. In this case, the muscle is divided from outside in. Depending on a number of issues, an associated Zenker’s diverticulum may or may not be removed at the same time.
Cricopharyngeal myotomy (1 of 7)
Cricopharyngeal myotomy (2 of 7)
Cricopharyngeal myotomy (3 of 7)
Cricopharyngeal myotomy (4 of 7)
Cricopharyngeal myotomy (5 of 7)

Cricopharyngeal myotomy (6 of 7)
Cricopharyngeal myotomy (7 of 7)

A-CPD, Before, During, and After CPM.
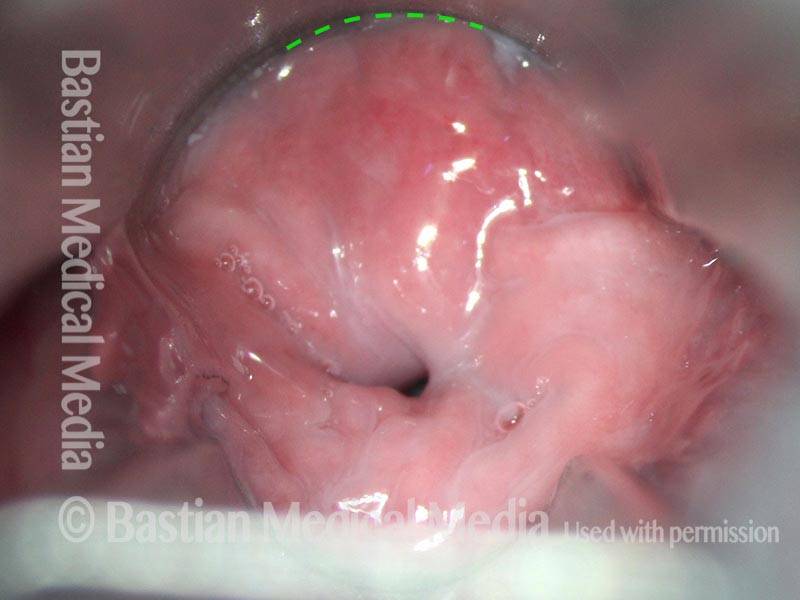
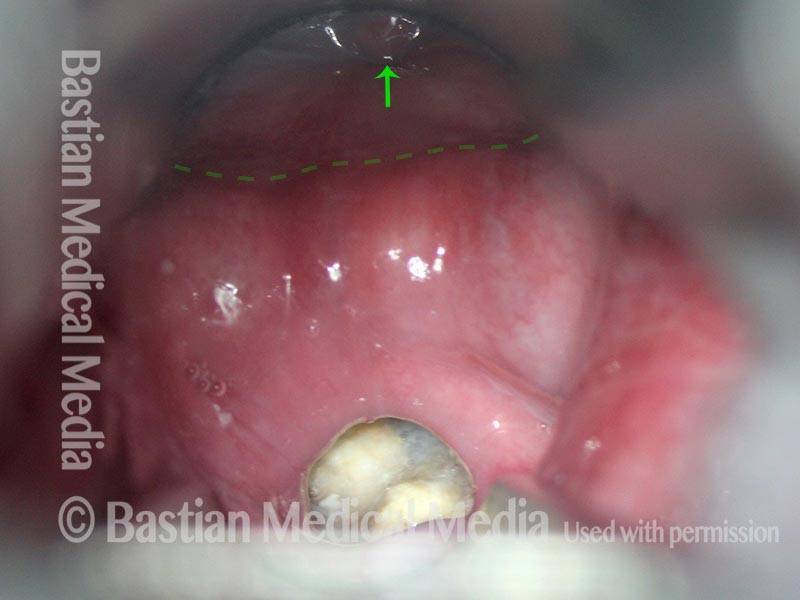
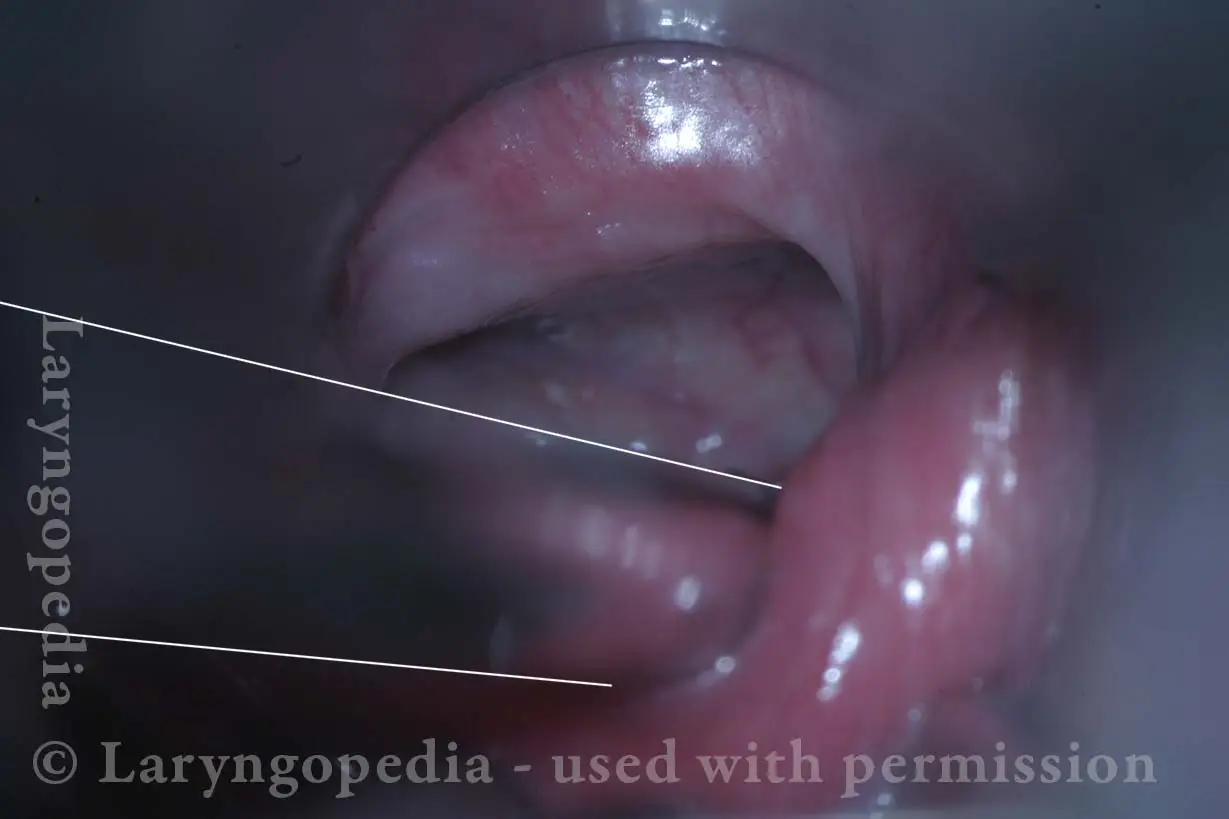
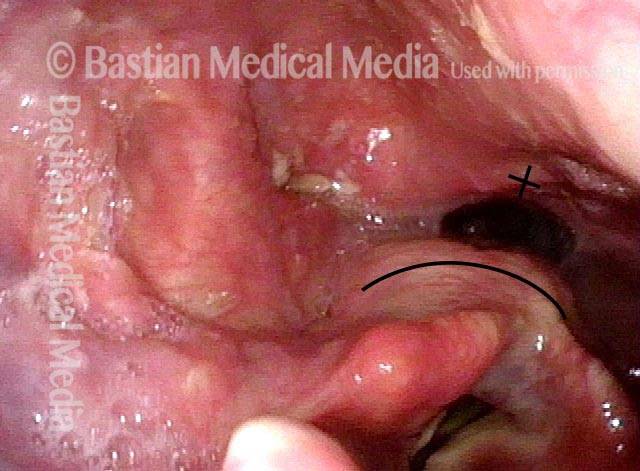
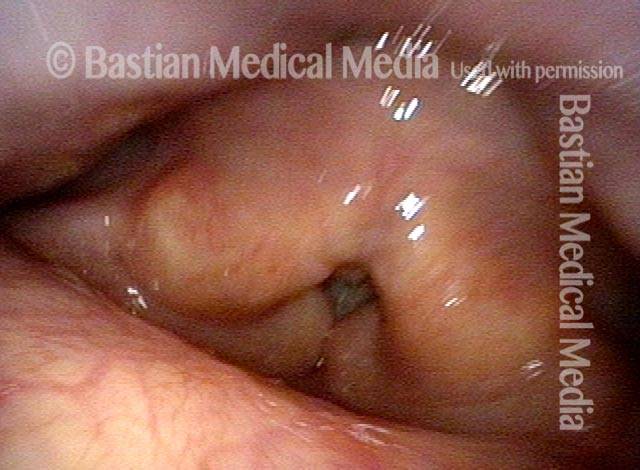
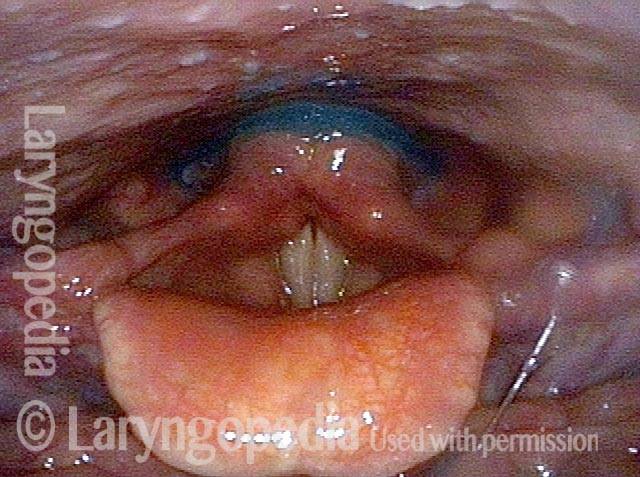
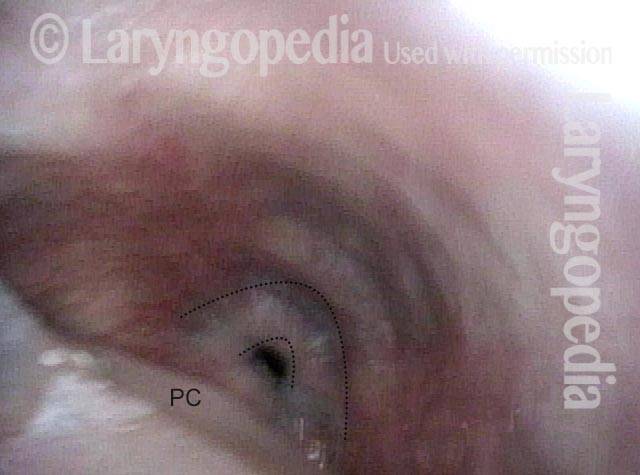
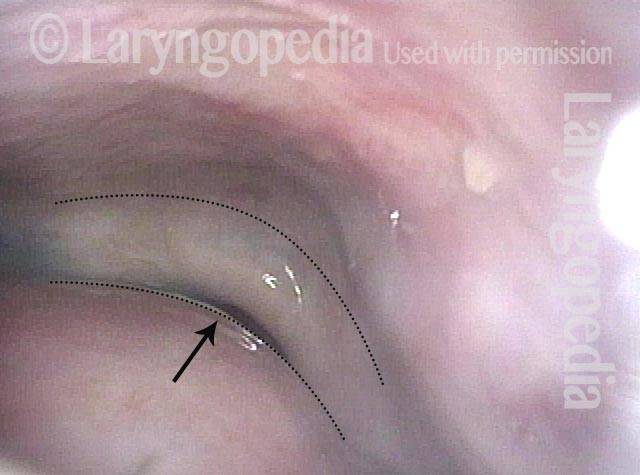
Non-relaxing cricopharyngeus muscle (1 of 4)

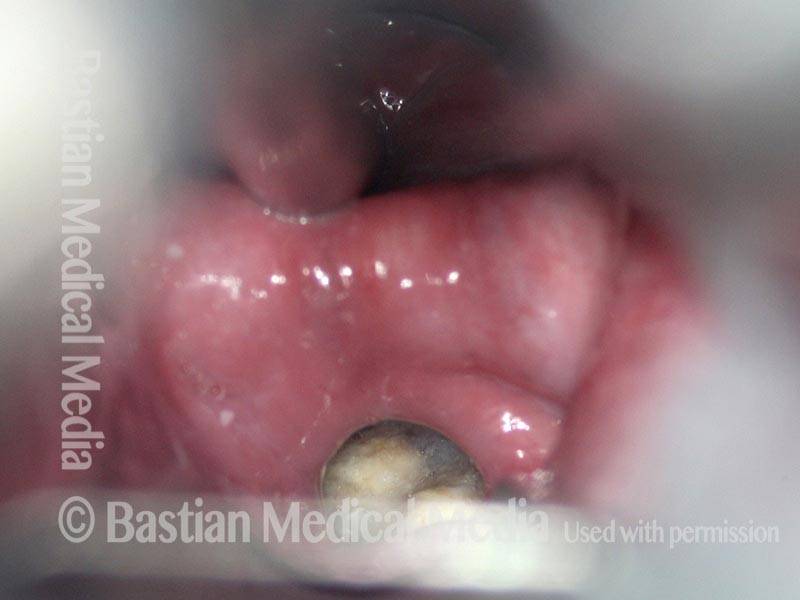
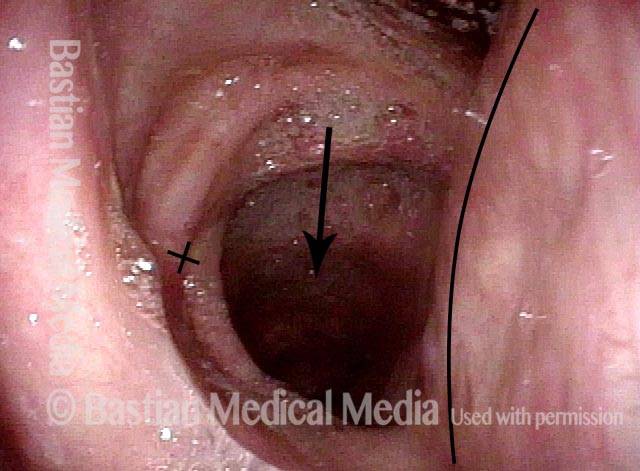
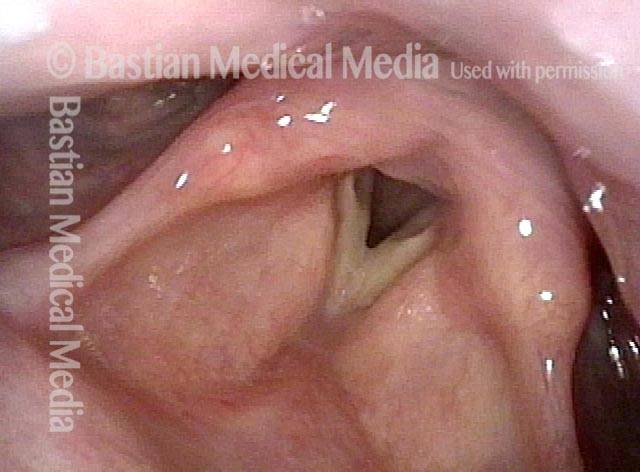
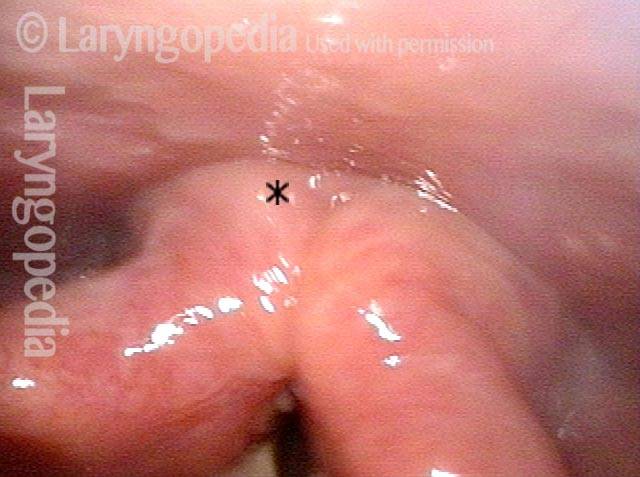
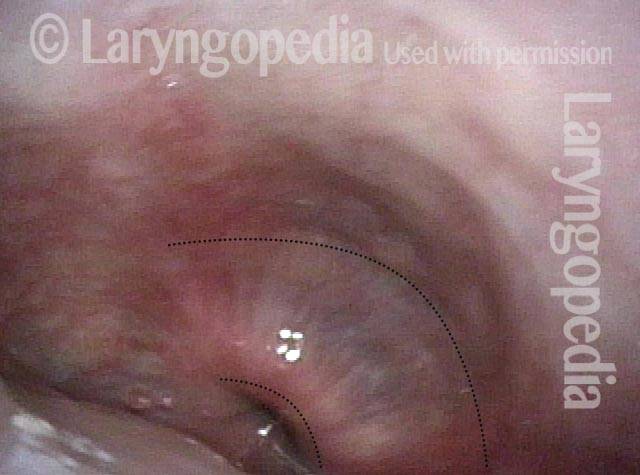
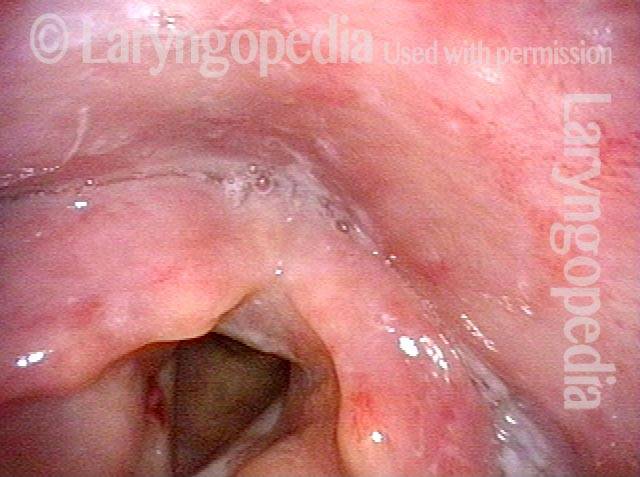
Opening the esophageal orifice (2 of 4)
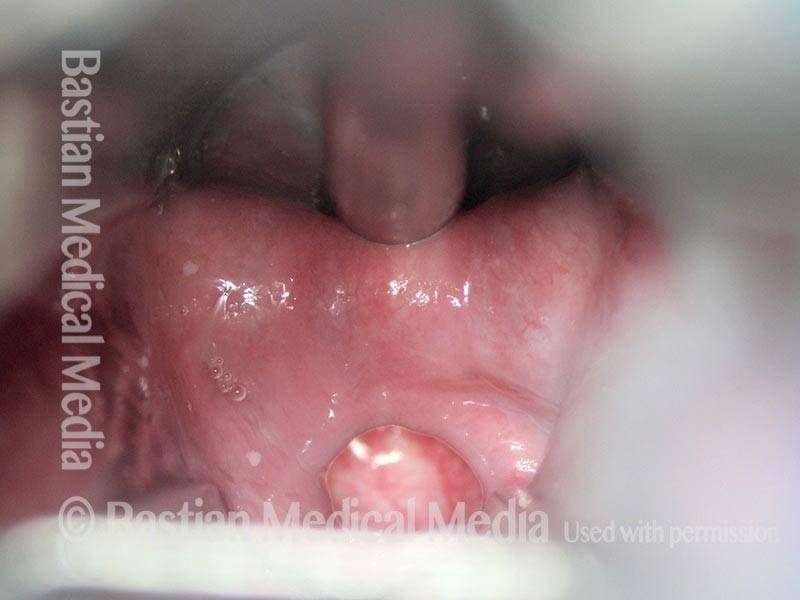
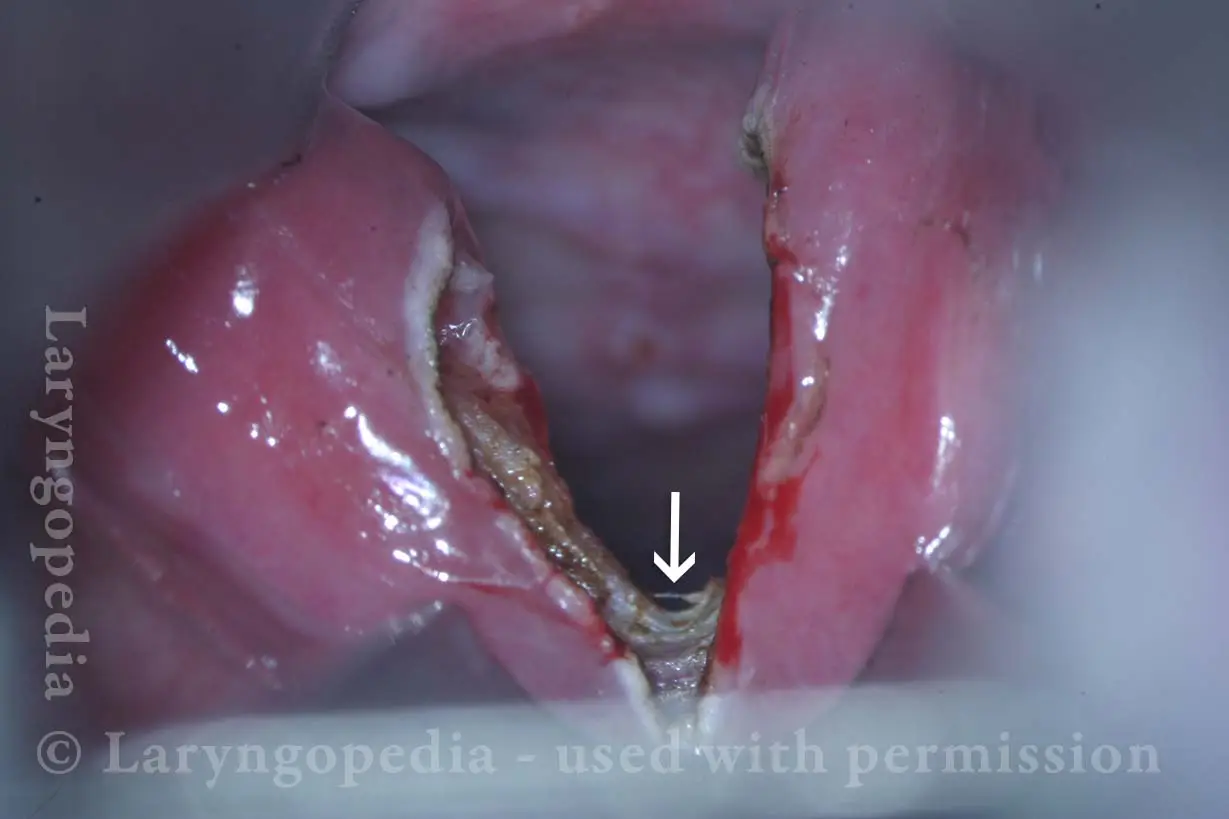
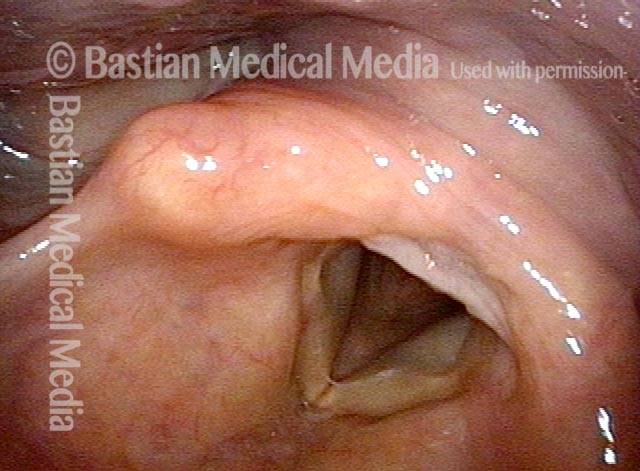
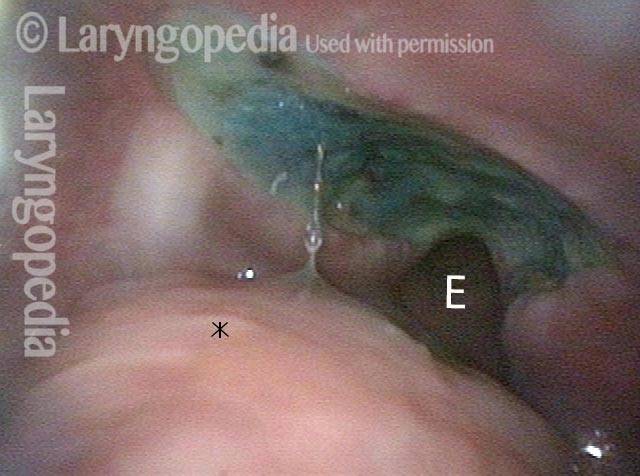
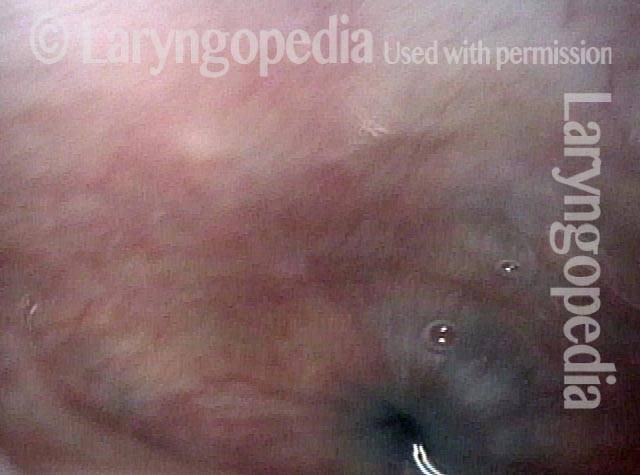
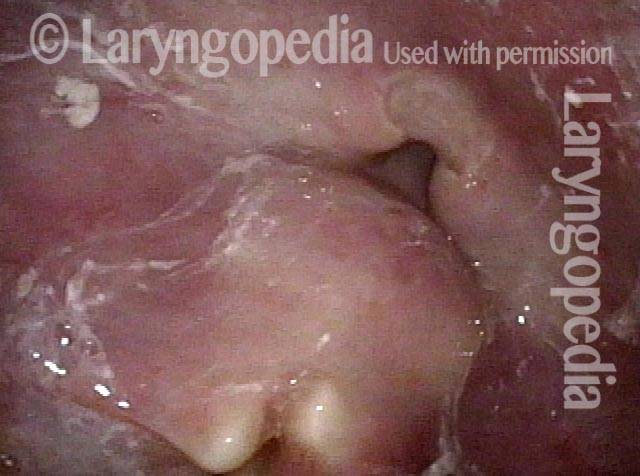
Laser cricopharyngeus myotomy (3 of 4)

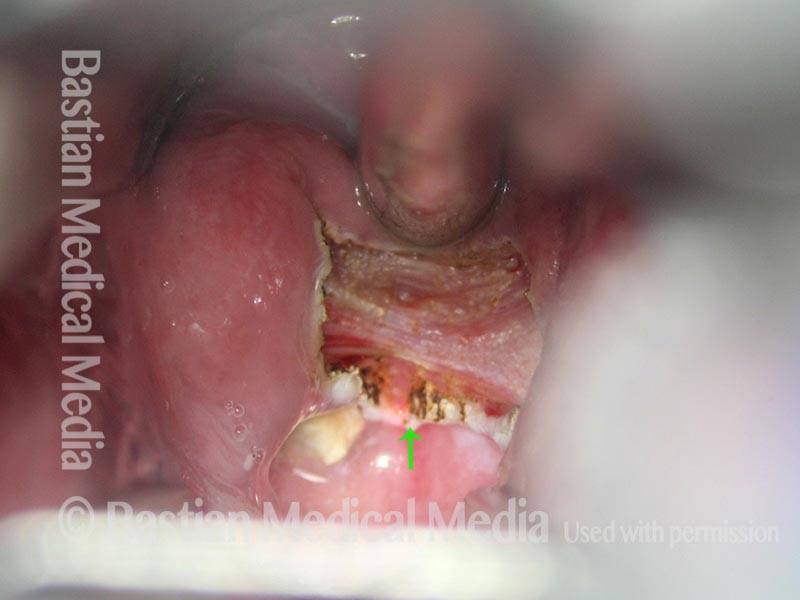
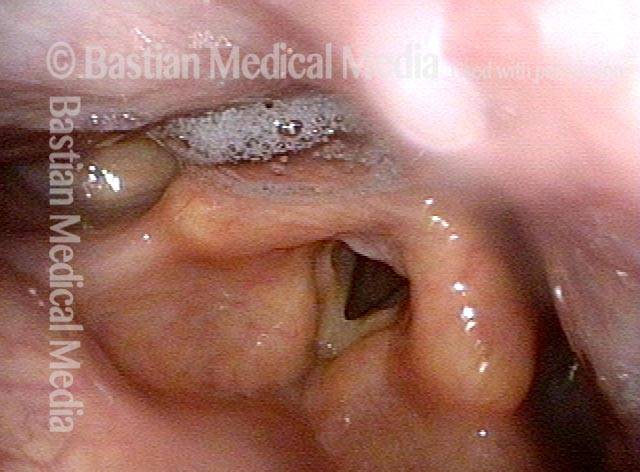
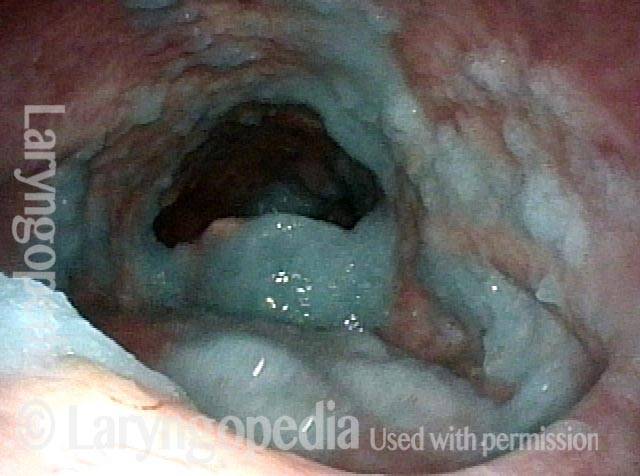
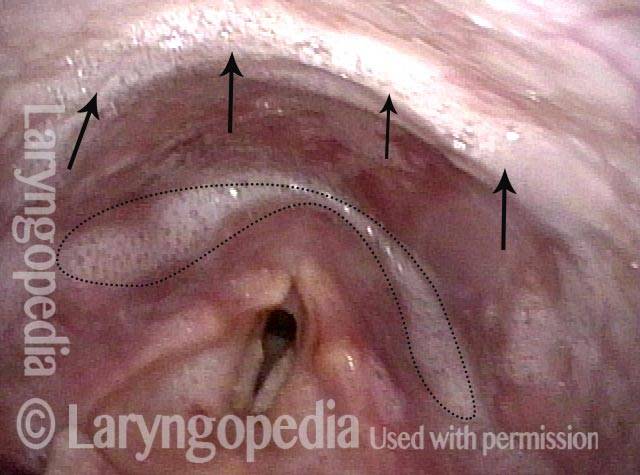
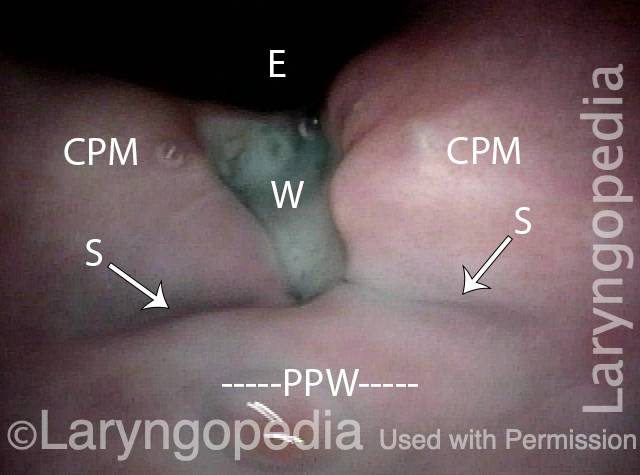
Cricopharyngeus myotomy nearly complete (4 of 4)
A-CPD X-rays, Before and After CPM
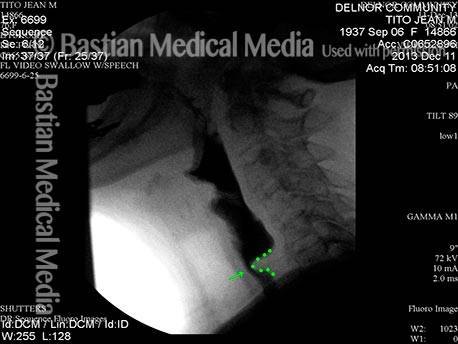
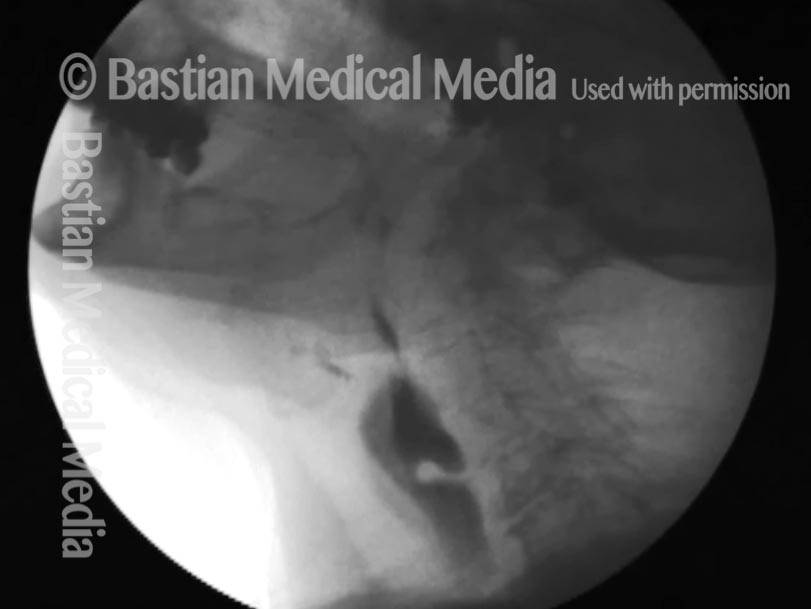
Cricopharyngeal dysfunction: before myotomy (1 of 2)

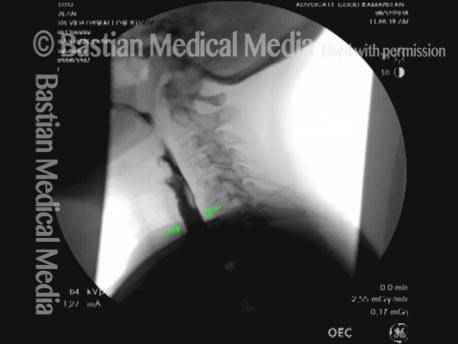
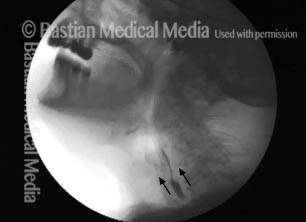
Cricopharyngeal dysfunction: after myotomy, resolved (2 of 2)

Example 2
Cricopharyngeal dysfunction: before myotomy (1 of 2)

Cricopharyngeal dysfunction: after myotomy, resolved (1 of 2)

Example 3
Cricopharyngeal dysfunction: before myotomy (1 of 2)
Cricopharyngeal dysfunction: after myotomy (2 of 2)
CPM for Recreational Eating and Management of Saliva
Panormaic view, post CPM (1 of 4)

Trumpet maneuver (2 of 4)
Closer view (3 of 4)
Well-managed saliva (4 of 4)

98 Year-old before and after CPM
Immediately after swallowing (1 of 10)
Zenker’s (2 of 10)
Dysphagia (3 of 10)
Residue from Zenker’s (4 of 10)

X-ray showing Zenker’s (5 of 10)
Moments later (6 of 10)
After myotomy (7 of 10)
No residue (8 of 10)

Zenker’s gone (9 of 10)

No barium in hypopharynx (10 of 10)

Great View of Fresh CPM Surgical Wound
CPM dysfunction (1 of 4)
VFSS six years later (2 of 4)

Five days post-op (3 of 4)
Cervical esopagus (4 of 4)
Bolus Stream before and after CPM
Pre-myotomy (1 of 2)

Post-myotomy (2 of 2)

VESS Findings after Radiotherapy
Narrowed pharyngeal wall (1 of 7)

Swallowing applesauce (2 of 7)
After sipping water (3 of 7)

Gravity aiding in swallowing (4 of 7)

Lifting larynx (5 of 7)
A closer look (6 of 7)
Gravity aiding again in swallowing (7 of 7)
The Evolution of a CPM Wound
Difficulty swallowing solid foods (1 of 8)
Pooled saliva (2 of 8)

Muscle bulge (3 of 8)
Residue in swallow crescent (4 of 8)

Three weeks later (5 of 8)
Residual “wound” (6 of 8)

Three months post-op (7 of 8)
At close range (8 of 8)

Zenker’s Diverticulum a Week after CPM
Zenker’s Sac (1 of 3)
Zenker’s Sac (2 of 3)

Zenker’s Sac (3 of 3)