Dysphagia
Dysphagia is the abnormal swallowing, or inability to swallow. It can result from such diverse causes as surgery on the larynx or neck, stroke, the aging process, tumor, injury to the neck, or radiation, among other things.
Treatment for Dysphagia (Swallowing Therapy)
This therapy is typically provided by a speech-language pathologist (and, more informally and adjunctively, by other healthcare professionals). General areas of teaching might include:
- Choosing wisely which food types and consistencies to eat (See Diet Modification below);
- Swallowing maneuvers such as tucking the chin, double swallow, effortful swallow, head turning, and supraglottic swallow;
- Direct exercises for the tongue, pharynx, palate, and larynx.
Diet Modification
These are suggested dietary changes, particularly regarding food consistencies, directed at improving a patient’s ability to swallow and at avoiding aspiration.
For example, an individual who is struggling with aspiration might be advised to avoid thin liquids and use thicker or carbonated liquids instead. Or this individual might be advised to avoid composite foods, since his or her swallowing deficiency could make it harder to “stay organized” with several consistencies in the mouth at once.

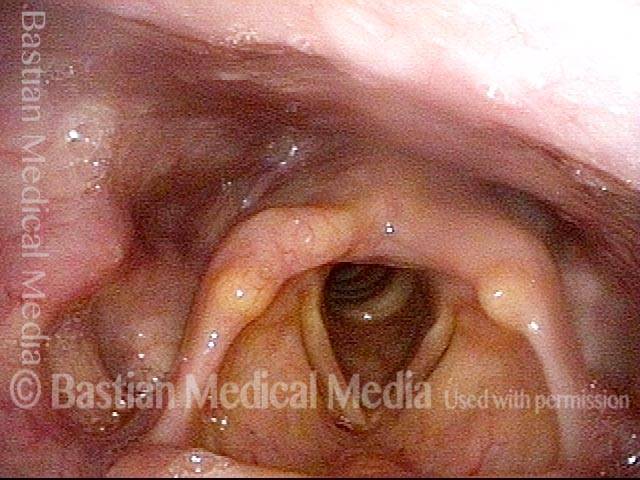
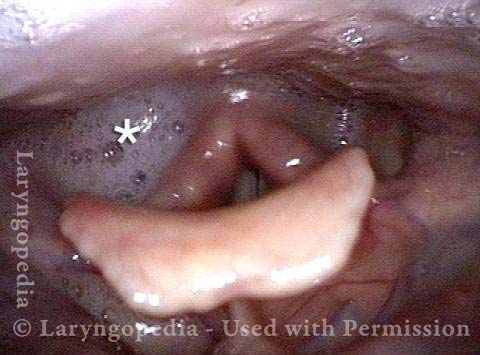
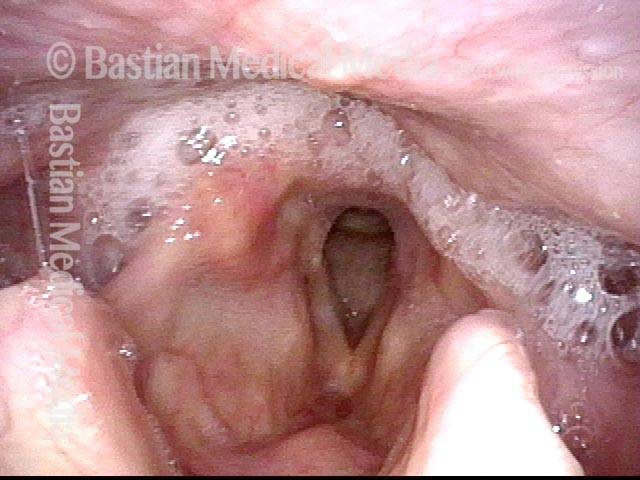
Dysphagia / Delayed Swallow Reflex
Laryngopharynx (1 of 3)
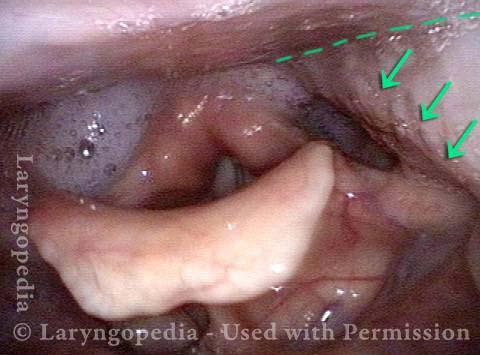
Dysphagia / Delayed swallow reflex (2 of 3)
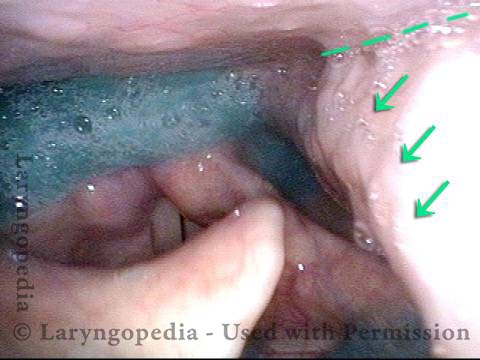
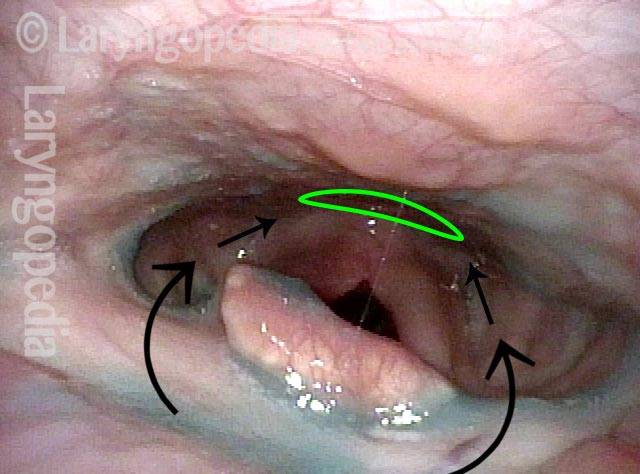
Hypopharyngeal pooling (3 of 3)
High Vagus Nerve Injury
The vagus (10th cranial) nerve originates from the medulla (part of the brainstem), exits from the base of the skull through the jugular foramen, and among other things, supplies branches to the musculature of palate, pharynx, and larynx. Location of vagus nerve injury is sometimes evident by palate and pharynx findings. But these findings are sometimes overlooked as in this case, especially if palate and pharynx are weak but not completely paralyzed.
Case study: This 50-something woman developed a weak voice and moderate difficulty swallowing upon awakening 5 months prior to this visit. Fortunately, her symptoms of weak voice and difficulty swallowing were not devastating, and are improving. But up to this examination, there has been no diagnosis.
This examination reveals a “lesion” of her right vagus nerve and it has to be at the base of the skull because palate, pharynx, and larynx muscles are all weak. Voice is functional but lacks the ability to project and has a “soft-edged” quality. A sophisticated listener can also hear mild hypernasality. The examination below prompts a scan with special attention to base of skull to be sure there is no mass lesion there.
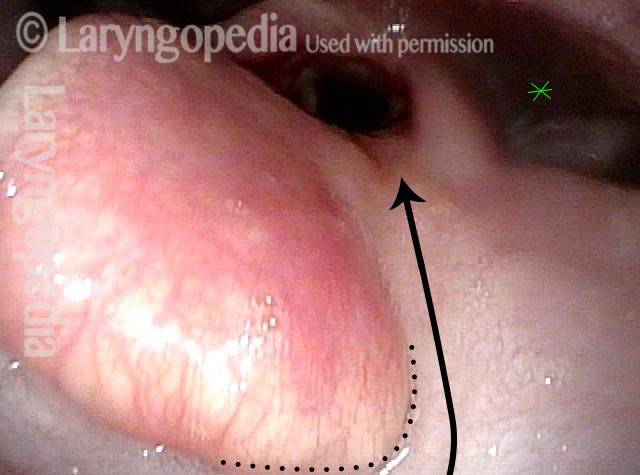
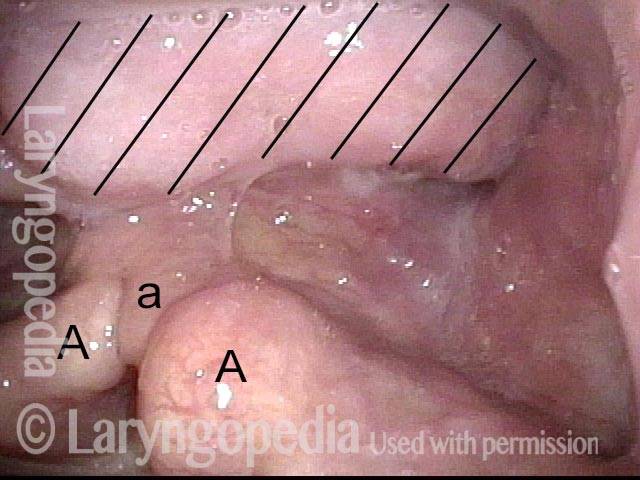
Nasopharynx (1 of 7)
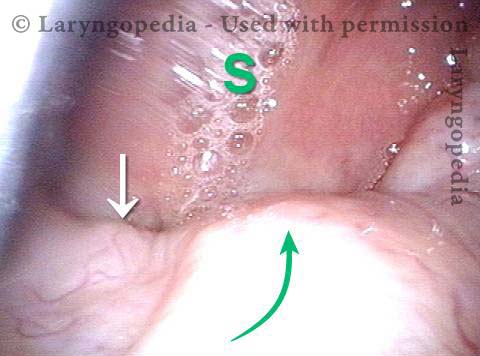
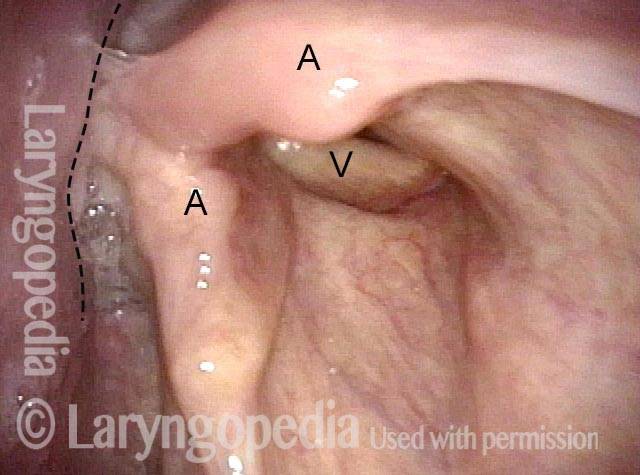
Saliva pooling in right pyriform sinus (2 of 7)
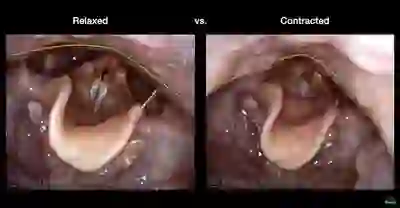
Pharynx contracts (3 of 7)
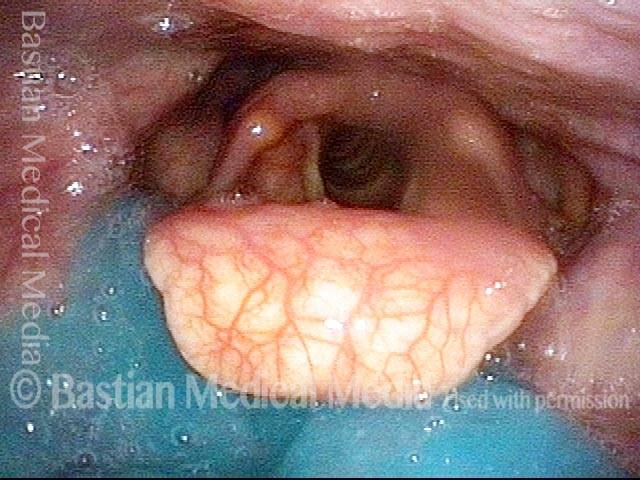
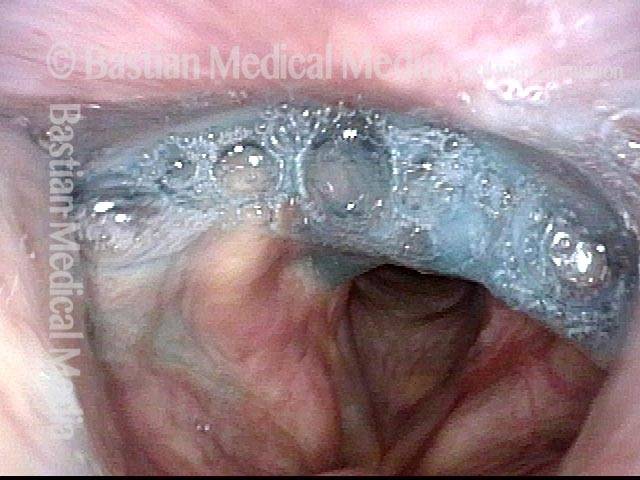
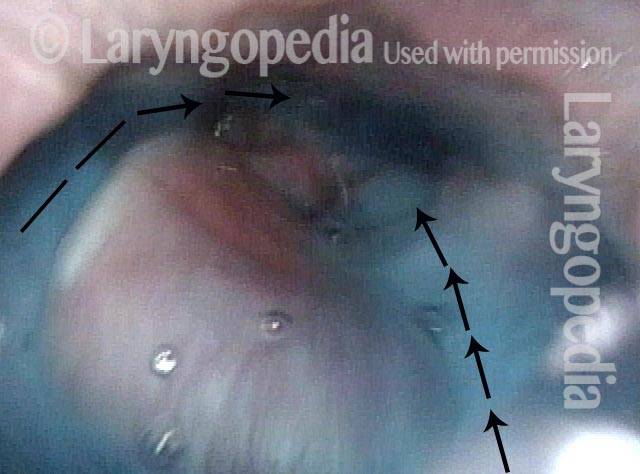
Swallowing blue applesauce (4 of 7)

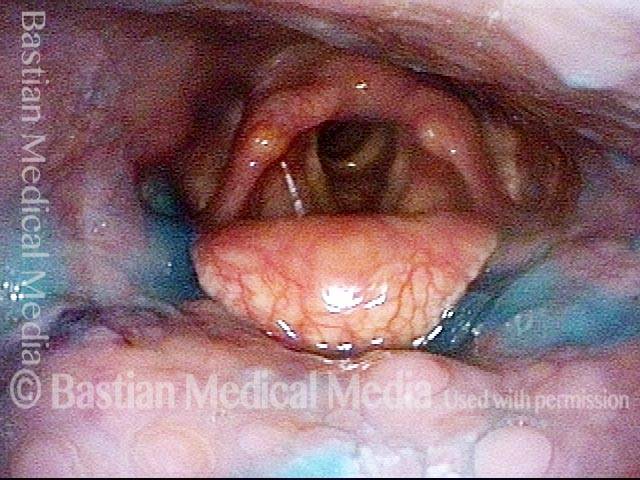
Unilateral pharynx contraction (5 of 7)
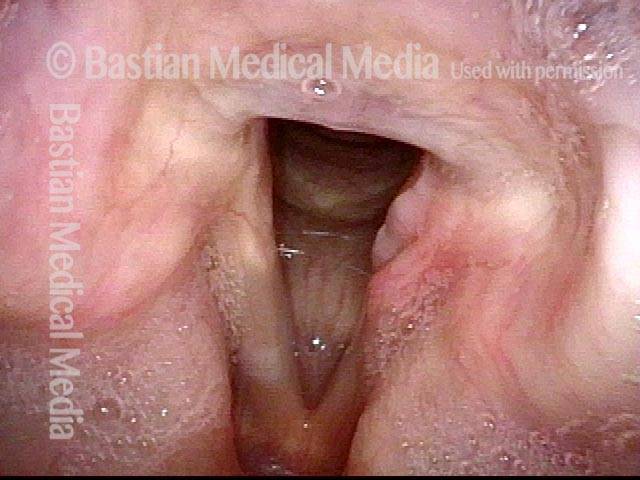
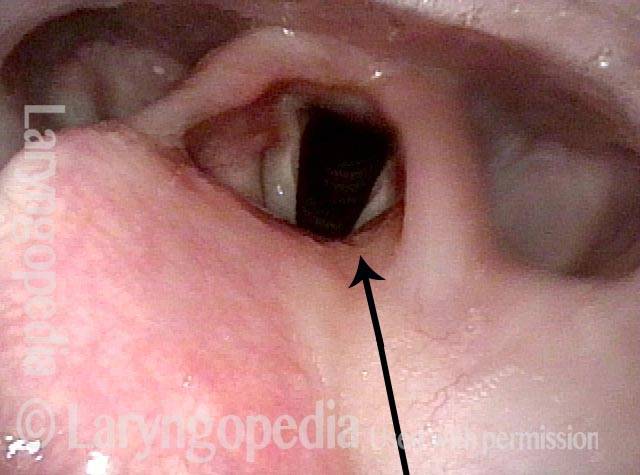
Right vocal cord paresis (6 of 7)
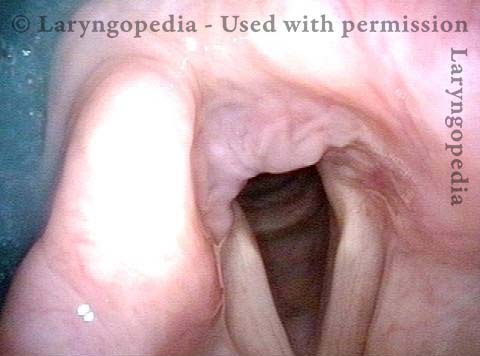
Vocal cord is paretic, not paralyzed (7 of 7)

Cricopharyngeal Dysfunction, Before & After Myotomy
Cricopharyngeal dysfunction: before myotomy (1 of 2)

Cricopharyngeal dysfunction: after myotomy, resolved (2 of 2)

Example 2
Cricopharyngeal dysfunction: before myotomy (1 of 2)

Cricopharyngeal dysfunction: after myotomy, resolved (1 of 2)

Dysphagia, Due to Tongue Weakness
Dysphagia, due to tongue weakness (1 of 4)

Dysphagia, due to tongue weakness (2 of 4)
Dysphagia, due to tongue weakness (3 of 4)
Dysphagia, due to tongue weakness (4 of 4)
Scarring Diverts Swallowed Materials Directly Into the Larynx
Post tonsillectomy (1 of 4)
Closer view (2 of 4)
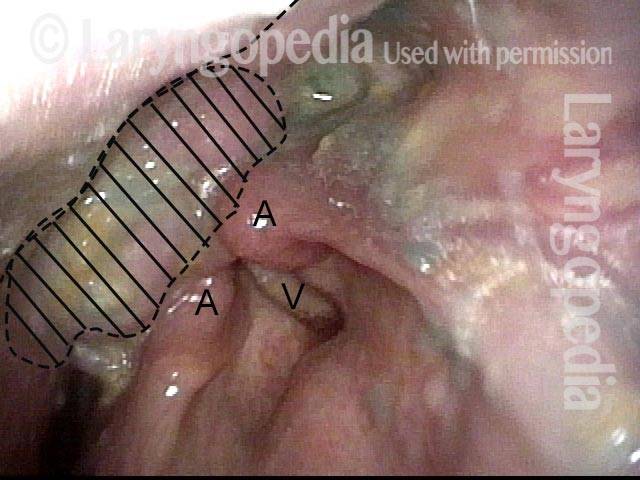
The “chute” (3 of 4)
Abnormal diversion (4 of 4)
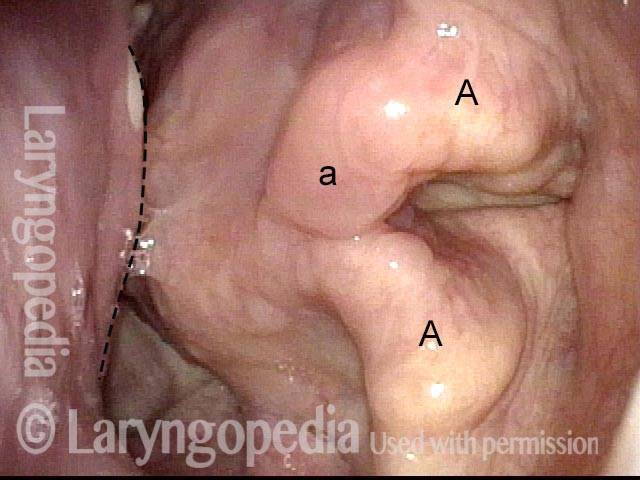
Solid Food Dysphagia Due to An Unexplained Benign Mass
Benign mass (1 of 4)
Closer view (2 of 4)
One week post-op (3 of 4)
Trumpet maneuver post-op (4 of 4)