Hypopharyngeal stenosis is the narrowing of the entrance to the upper esophagus, at the junction of the throat and esophagus. It is a possible but uncommon complication for individuals with larynx or pharynx cancer who undergo radiation therapy as part of their treatment regimen.
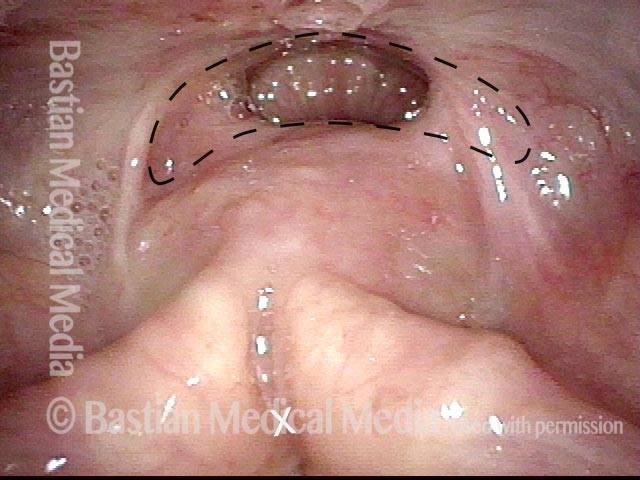
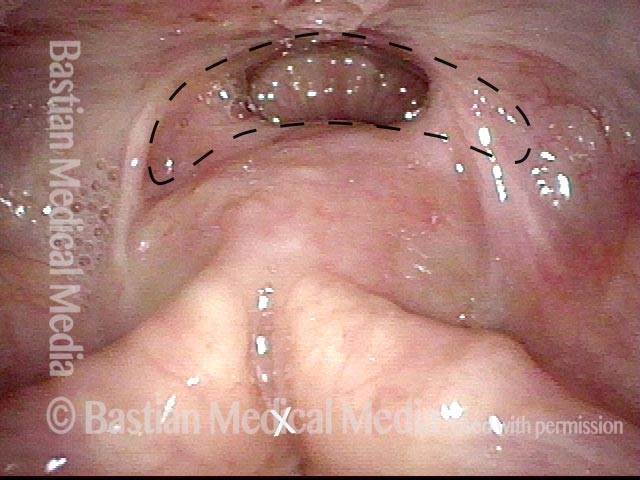
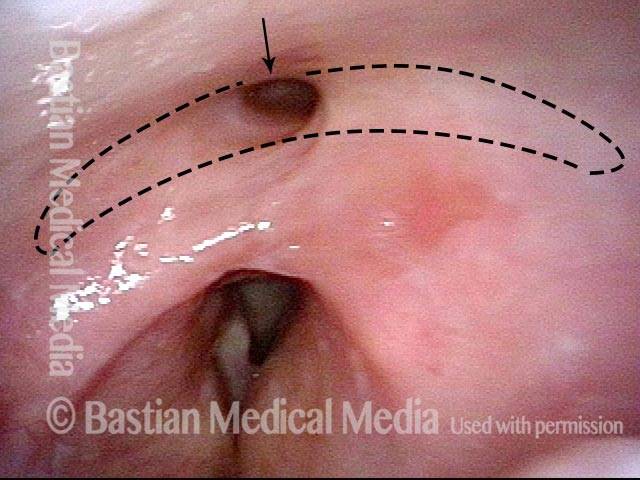
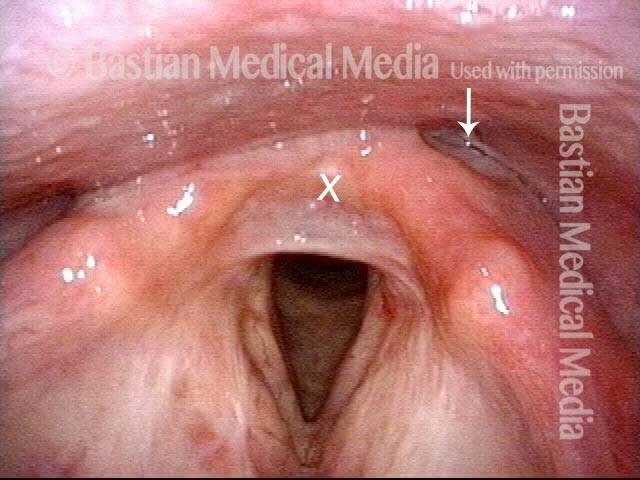
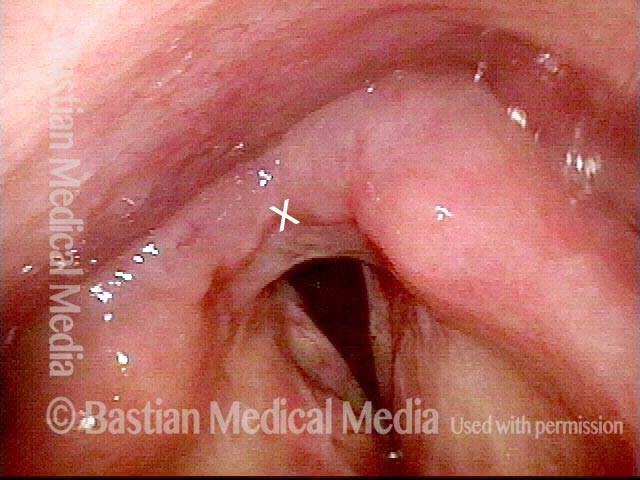
Hypopharyngeal stenosis: not yet visible (1 of 2)
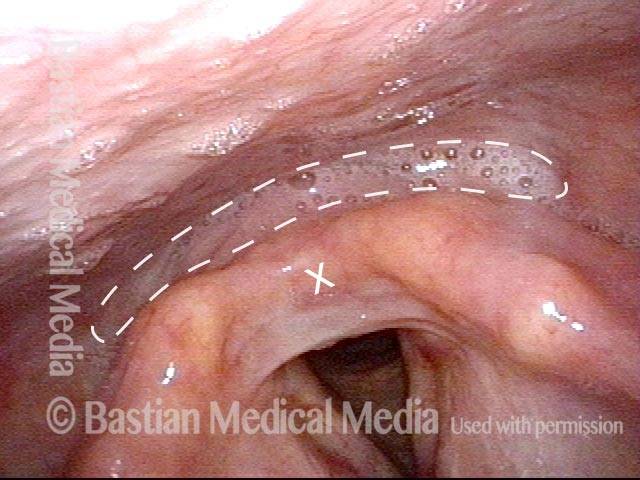
Panoramic view of the larynx, with the swallowing “crescent” in the middle of the view (indicated by the dotted lines). Several months prior, this patient had laser resection for hypopharyngeal cancer. Expected scarring from the surgery led to a stenosis (that is, a narrowing) at the entrance to the esophagus. The stenosis cannot be seen here, but is revealed in the next photo (for reference, an “X” marks the same point in the larynx in both photos).
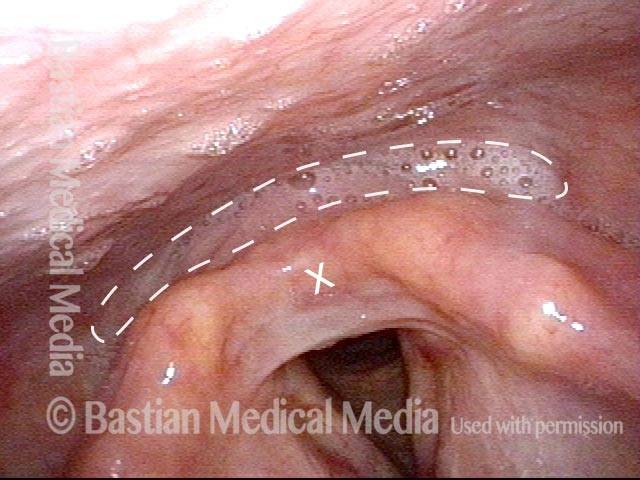
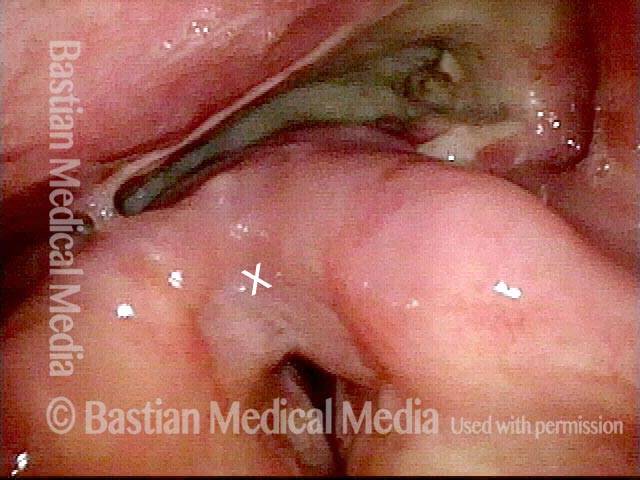
Hypopharyngeal stenosis: revealed (2 of 2)
The patient performs the trumpet maneuver, which splays open the hypopharynx, revealing the stenosis; the dotted lines represent what would be a normal-sized opening. This stenosis affects swallowing of solid food, but the patient says this is no problem for him, if he eats a little more slowly and chews well.
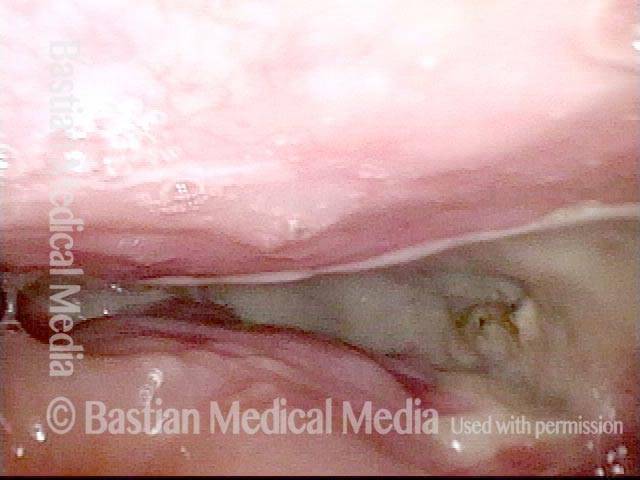
Esophageal Stenosis from Radiation
Post radiation therapy (1 of 3)
This man finished chemotherapy + radiation therapy elsewhere for base of tongue cancer with neck disease, finishing a year prior to this examination. Despite swallowing therapy and VitalStim treatments, he was unable to swallow even his own saliva.The actual diagnosis is seen in the next photo. Panoramic view of hypopharynx.

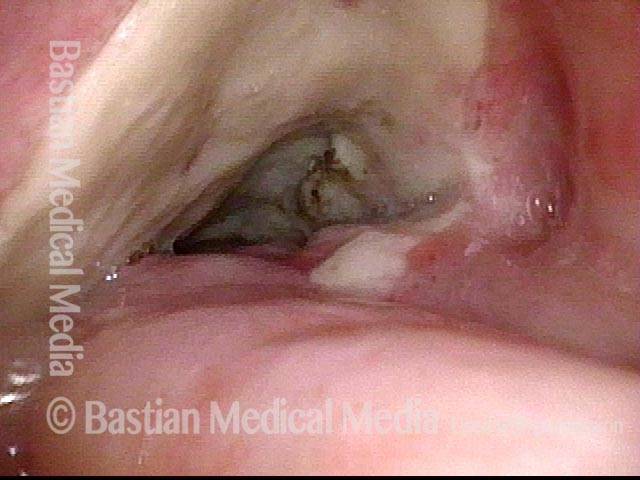
Small stricture (2 of 3)
During “trumpet maneuver,” the larynx pulls anteriorly and reveals a stricture of very small size, at arrow. This would normally allow passage of saliva, but in this case it does not. View photo 3 for explanation.
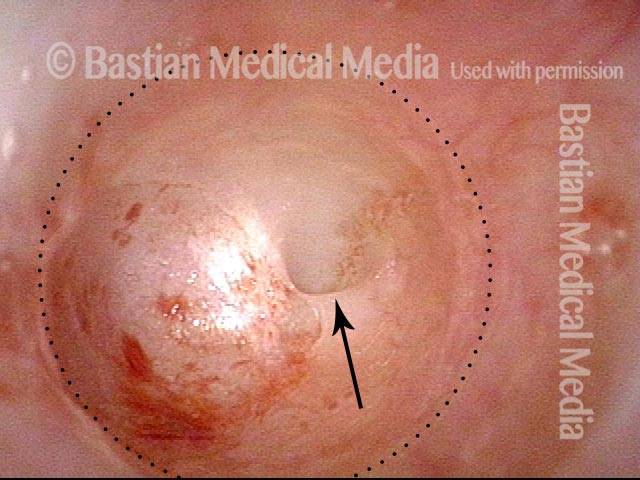
Esophageal stenosis (3 of 3)
The stricture ends as a virtually blind pouch. Here, the scope has been inserted to a distance of nearly an inch into the stricture seen in prior photo, at which point a near-total stenosis is found. The arrow shows a pinhole opening less than a millimeter in diameter. The dotted line shows the expected size of opening at this level.
Dilation for Post-Radiation Hypopharyngeal Stenosis
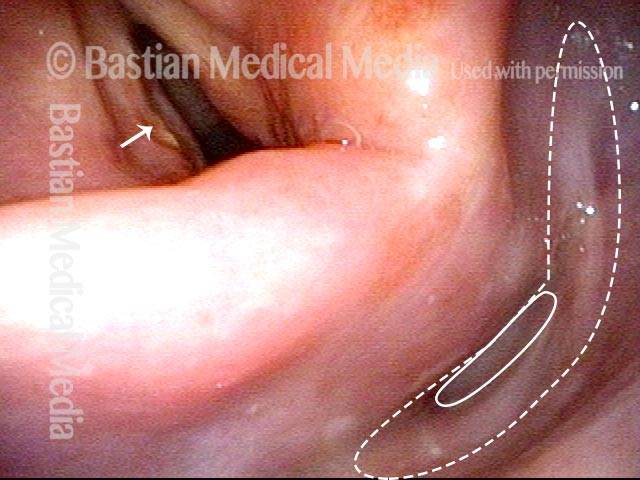
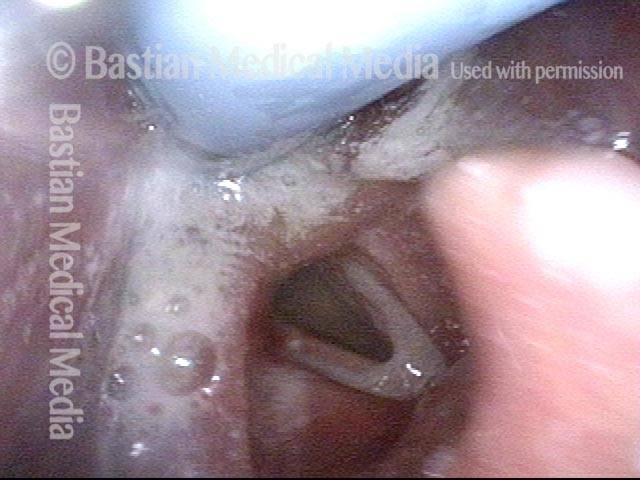
Dilation for post-radiation hypopharyngeal stenosis (1 of 4)
Early after radiotherapy for left vocal cord cancer (indicated by arrow), tumor seems to have responded, but it has become difficult to swallow solid foods due to a radiation-induced stricture (indicated by solid oval) with expected lumen (indicated by the dotted lines).
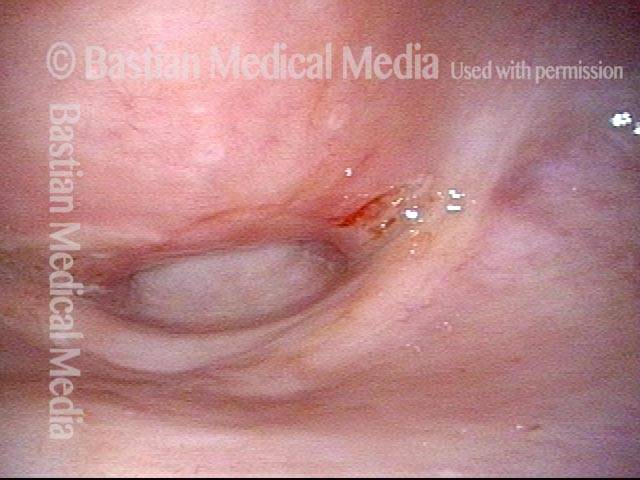
Dilation for post-radiation hypopharyngeal stenosis (2 of 4)
Closer-range view of the stricture at opening to the esophagus.
Dilation for post-radiation hypopharyngeal stenosis (3 of 4)
A tapered device used for dilation (bougie) is now inserted into the stricture and down into the upper esophagus in order to enlarge the entrance to the esophagus.
Dilation for post-radiation hypopharyngeal stenosis (4 of 4)
Immediately following dilation, the opening is enlarged (compare with photo 2). The patient’s ability to swallow food improved noticeably, but not to normal.

Hypopharyngeal Cancer, before and after Surgery
Hypopharyngeal cancer (1 of 10)
Years after successful radiotherapy for glottic cancer, during a routine, yearly follow-up examination, a new hypopharyngeal cancer (invasive squamous cell carcinoma) is barely seen, at arrow. (For reference, X marks the same location in the larynx throughout this series.)
Hypopharyngeal cancer (2 of 10)
Trumpet maneuver begins, to splay open the post-arytenoid part of the posterior pharyngeal wall (arrows and dotted lines), as well as the pyriform sinuses on each side. The tumor is now seen clearly. (Note the change of perspective from photo 1, using X as a reference point.)

Hypopharyngeal cancer (3 of 10)
Similar view to photo 2 (still with the trumpet maneuver), but now with the tumor outlined.
Hypopharyngeal cancer (4 of 10)
Closer view than photos 2 and 3 (again, still with the trumpet maneuver), with the tumor still outlined. Radiation is not an option for this tumor because of prior larynx irradiation; an attempt at laser surgery was selected.
Hypopharyngeal cancer: 1 week after surgery (5 of 10)
One week after laser excision of the tumor. Note the widespread redness, and the swollen arytenoid mounds, especially on the right side of the image. Compare with photo 1.
Hypopharyngeal cancer: 1 week after surgery (6 of 10)
Panoramic view, with the patient beginning the trumpet maneuver. The surgical wound is coming into view. Compare with photo 2 (again, using X as a reference point).
Hypopharyngeal cancer: 1 week after surgery (7 of 10)
Maximum trumpet maneuver. Closer view of the surgical wound. Compare with photo 4.
Hypopharyngeal cancer: 1 week after surgery (8 of 10)
View into the left pyriform sinus, where the tumor was most bulky.
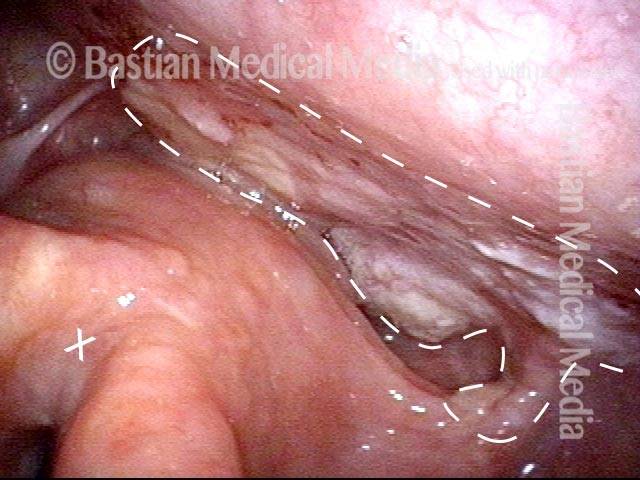
Hypopharyngeal cancer: several months after surgery (9 of 10)
Months after laser resection, panoramic view, showing the swallowing “crescent” (within dotted lines), at the upper limit of where the laser resection occurred. There is surgical stenosis at the entrance to the esophagus (shown in the next photo). This stenosis affects swallowing of solid food, but the patient says this is no problem for him, if he eats a little more slowly and chews well.
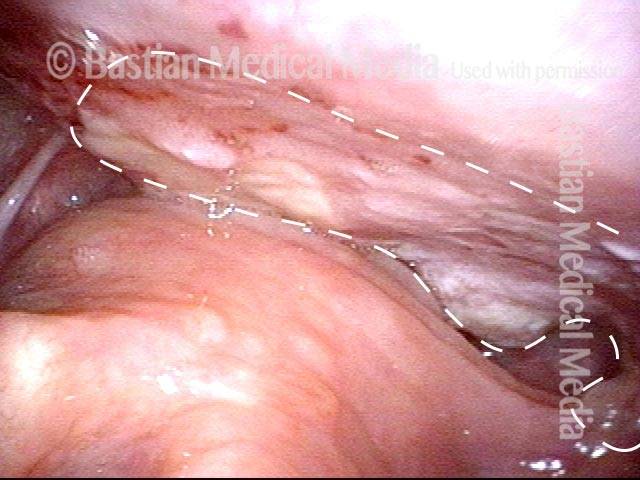
Hypopharyngeal cancer: several months after surgery (10 of 10)
With the trumpet maneuver, again splaying open the hypopharynx, as in photo 2. Notice the hypopharyngeal/ postcricoid stenosis; the dotted lines represent what would be a normal-sized opening.