Office Laser, Even Occasionally for Singers
Ordinarily, vocal cord microsurgery is only for otherwise irreversible lesions. This is especially so in singers, even though when done well, such surgery is extremely safe and voice restoring. And if time and therapy approaches fail to resolve a lesion, the typical venue for surgery is in the operating room under brief general anesthesia, with use of an operating microscope and tiny instruments.
Still, there is an office option that can occasionally be considered. Capillary ectasia without a nodule or polyp, for example, can be well managed in the videoendoscopy procedure room using only topical anesthesia. And there are circumstances (medical issues, jaw anatomy, etc.) that cause a specific singer to prefer office-based laser surgery with pulsed-KTP, thulium, or “blue” laser.
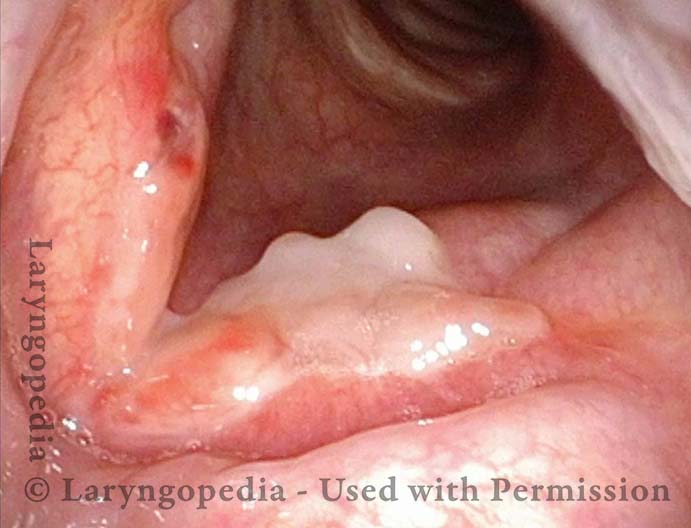
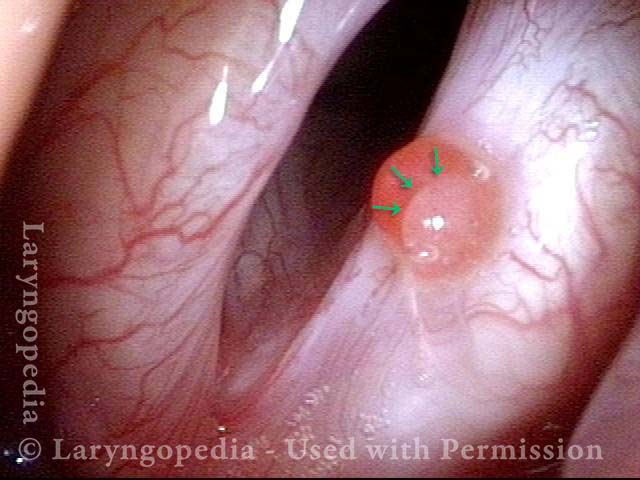
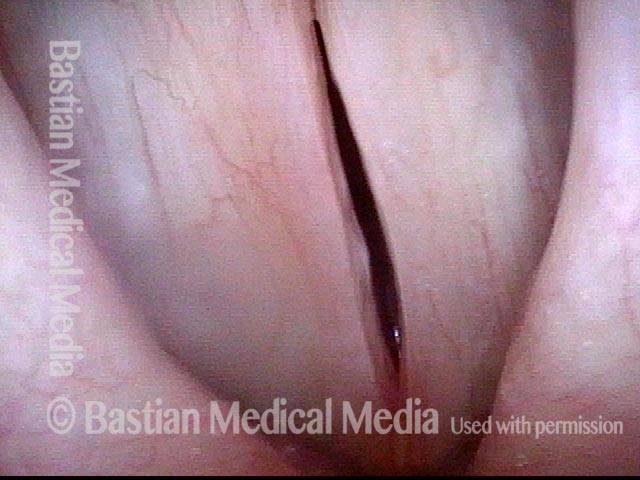
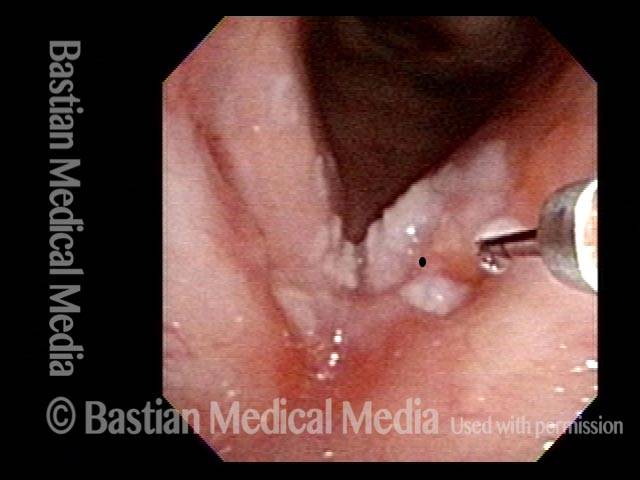
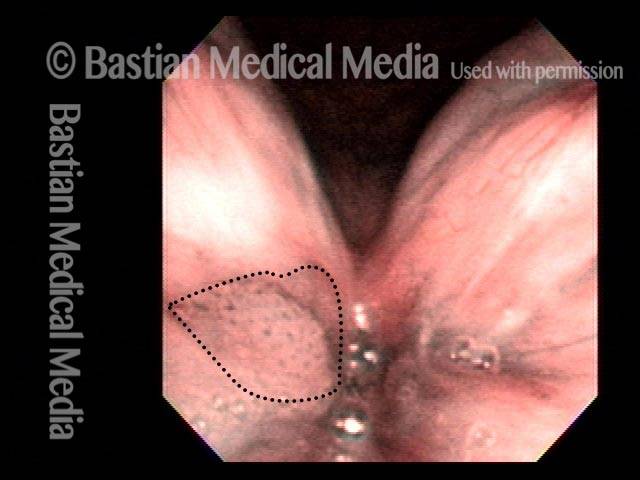
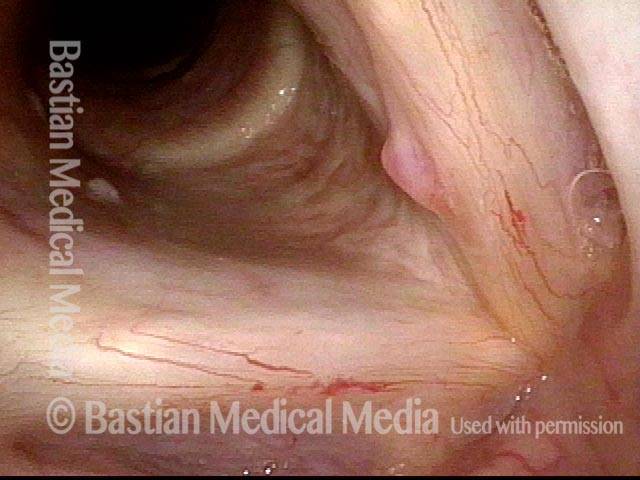
Right Vocal Cord Polyp (1 of 8)
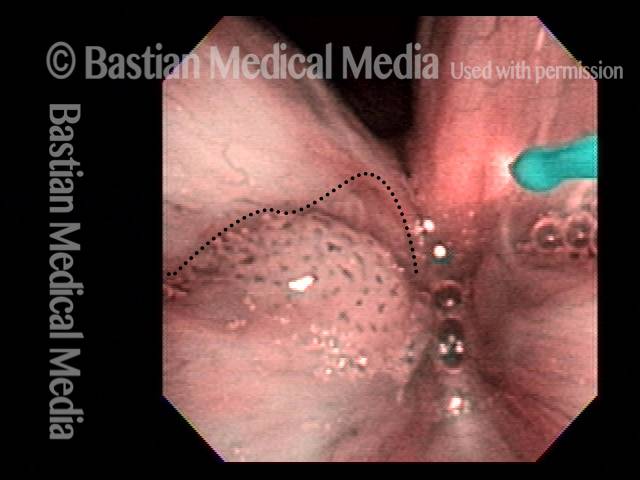
Polyp interferes with voice (2 of 8)

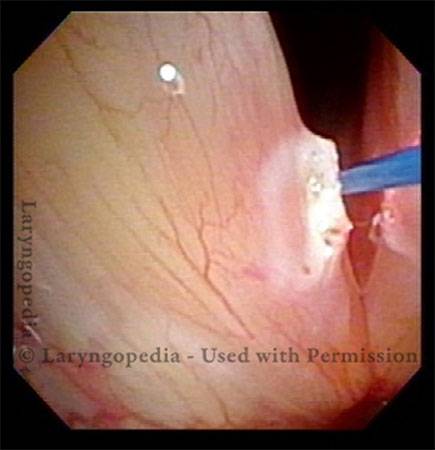
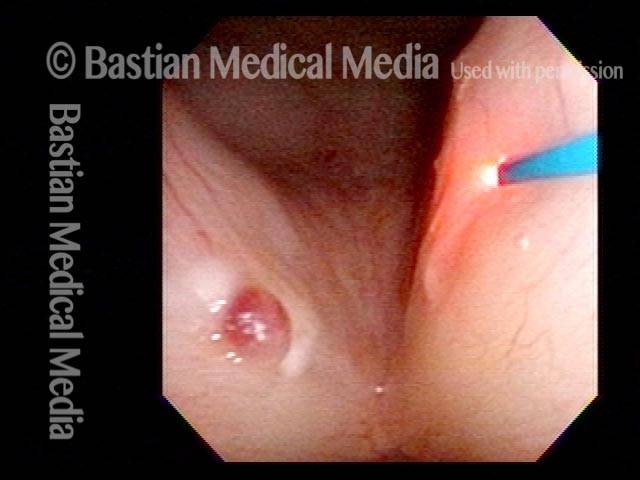
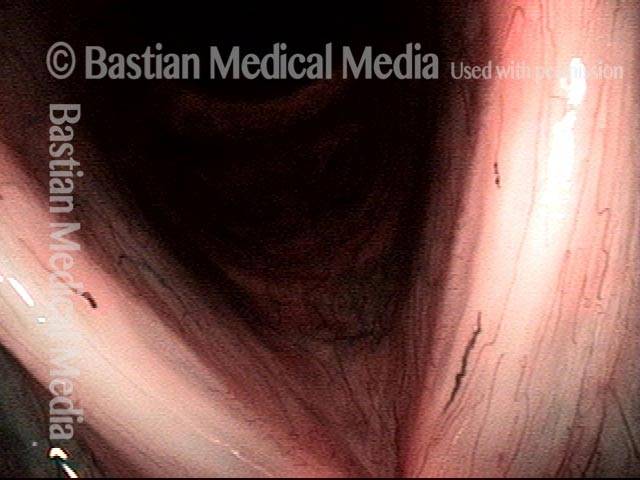
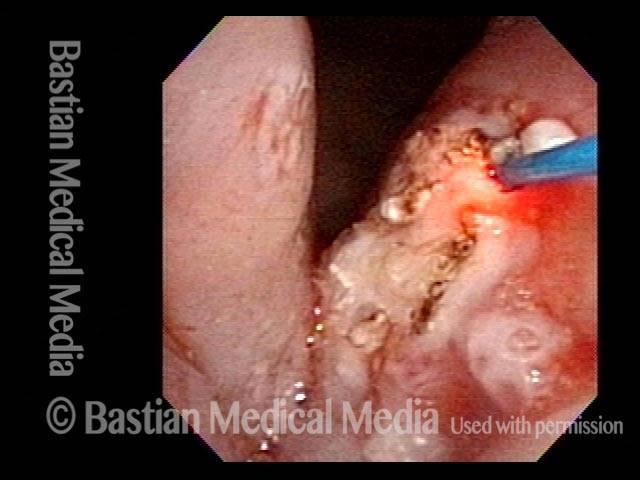
Laser surgery in singer (3 of 8)

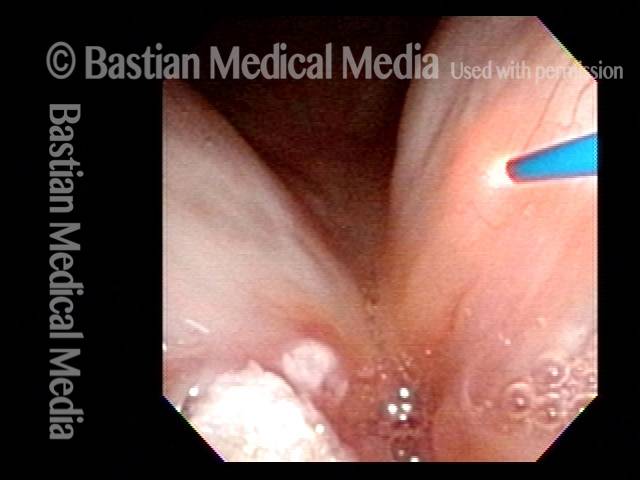
Coagulated polyp (4 of 8)

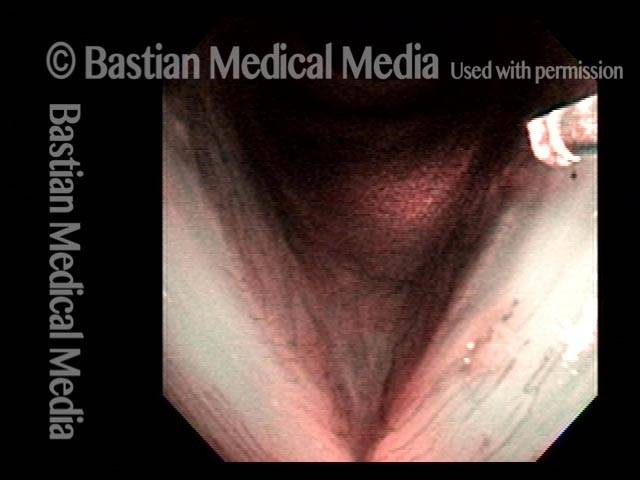
Coagulated polyp (5 of 8)
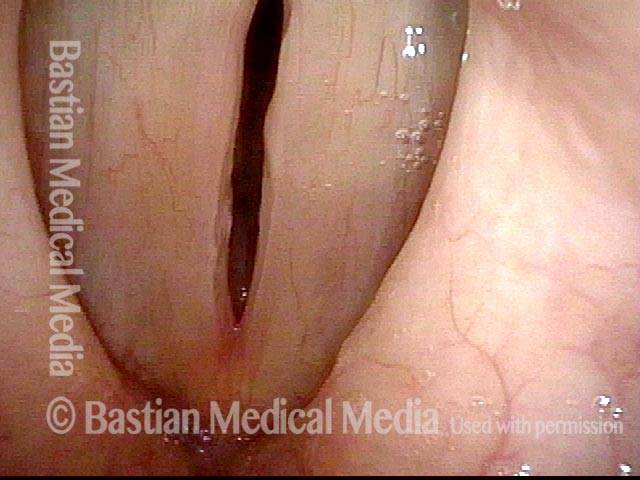
Voice fully restored (6 of 8)

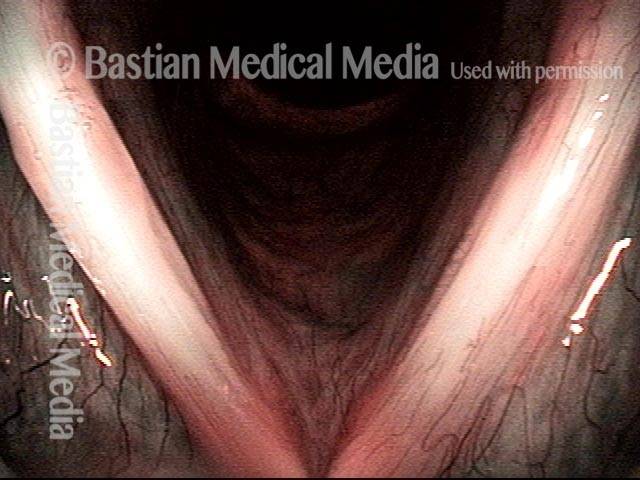
Margins match during phonation (7 of 8)

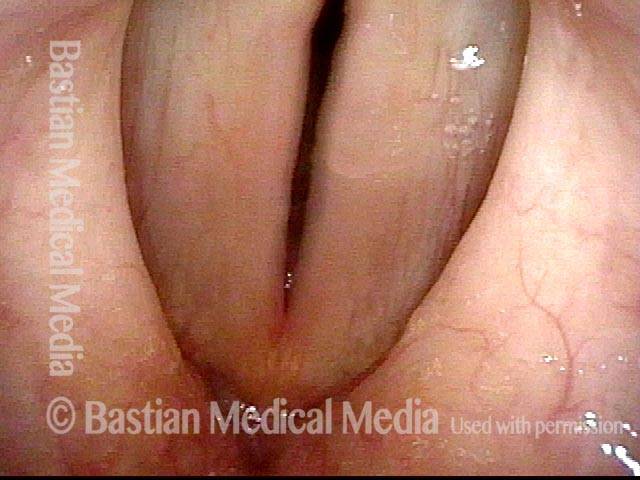
Equal vibration (8 of 8)

Laser Removal of Vocal Cord Cancer with Bilateral Disease
For treatment of early vocal cord cancer, both laser excision and radiotherapy are in competition as good treatment modalities. See also Early Vocal Cord Cancer: Remove with a Laser, or Radiate? Often, radiation is used when disease is bilateral, in the interest of preserving voice.
This is an example of the ability to do fairly extensive laser surgery bilaterally, yet preserving good voice. This man had a friend who had severe difficulty with radiation, and he was therefore opposed to that option.
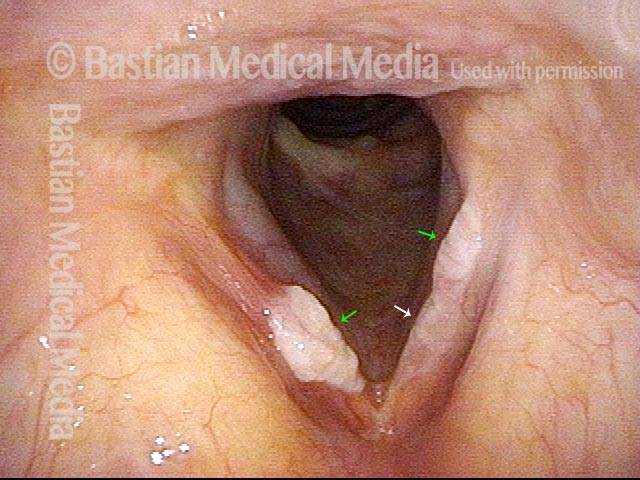
Vocal cord cancer (1 of 10)

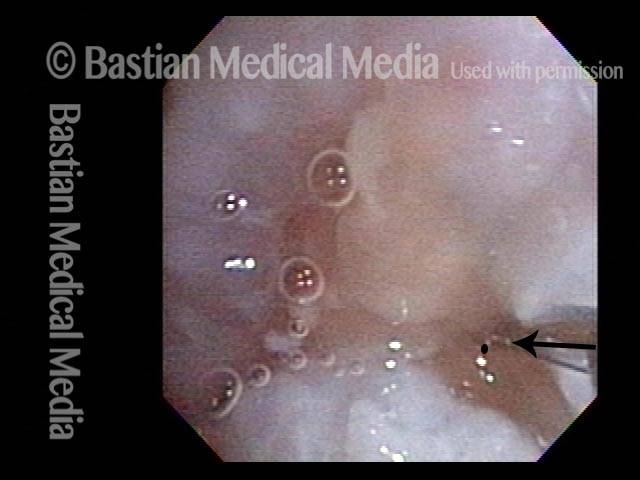
Stippling (2 of 10)
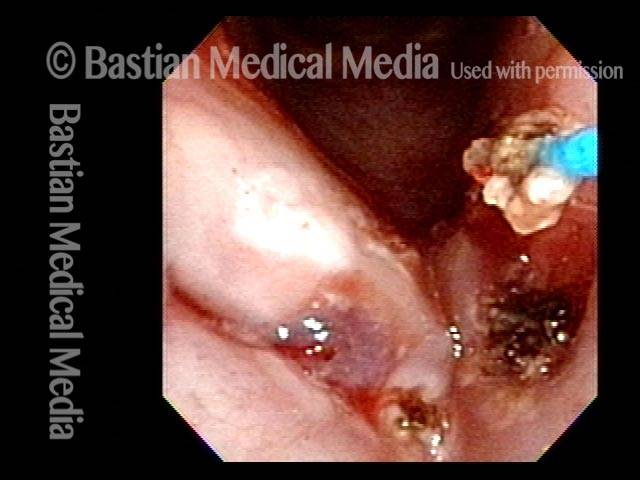
1 week after excision (3 of 10)
Reparative Granuloma emerges (4 of 10)

Granuloma interferes with voicing (5 of 10)

Granuloma fades away (6 of 10)

Closer view (7 of 10)
Granuloma cleft (8 of 10)
Blood tattoo (9 of 10)

Voice is improved (10 of 10)

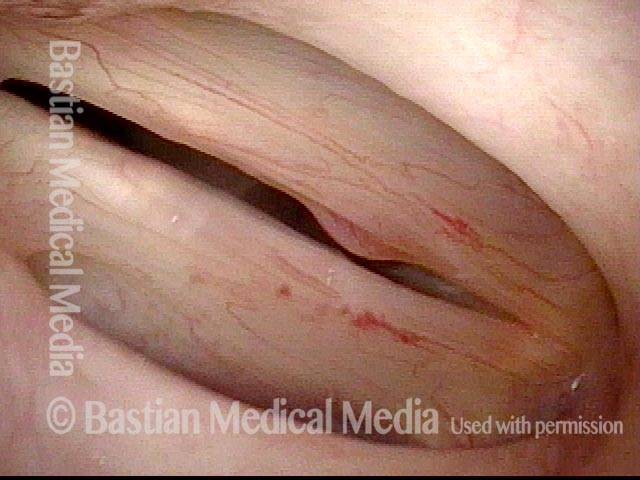
Hemorrhagic Polyp, Treated By Thulium Laser
Hemorrhagic polyp, treated by thulium laser (1 of 8)

Hemorrhagic polyp, treated by thulium laser (2 of 8)
Hemorrhagic polyp, treated by thulium laser (3 of 8)

Hemorrhagic polyp, treated by thulium laser (4 of 8)

12 weeks after thulium laser treatment (5 of 8)
12 weeks after thulium laser treatment (6 of 8)
12 weeks after thulium laser treatment (7 of 8)

12 weeks after thulium laser treatment (8 of 8)
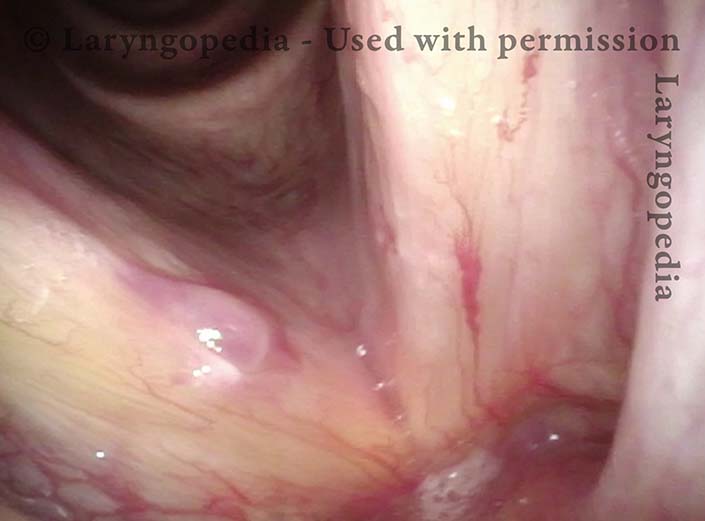
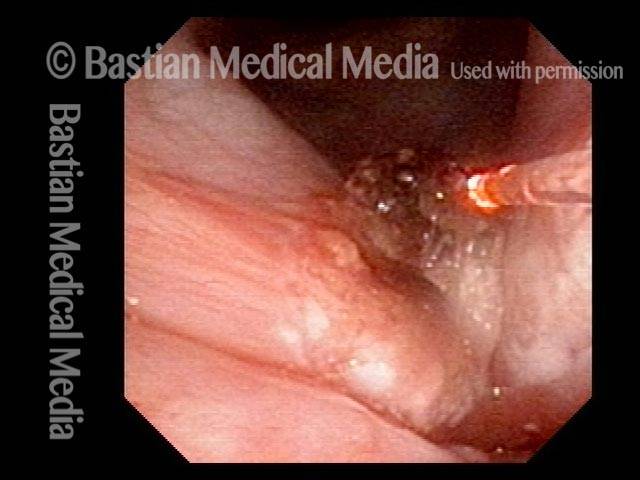
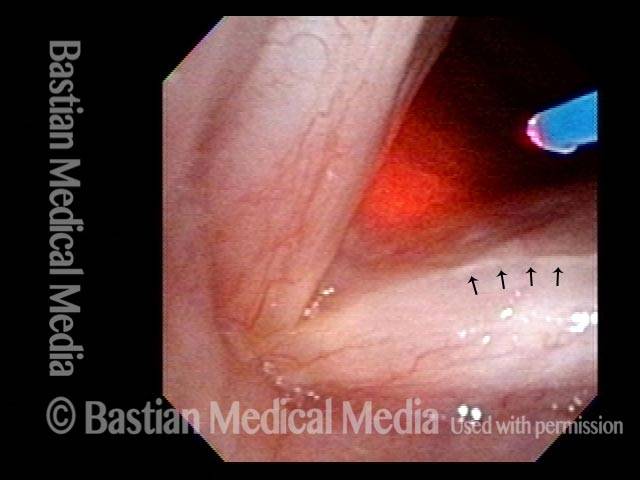
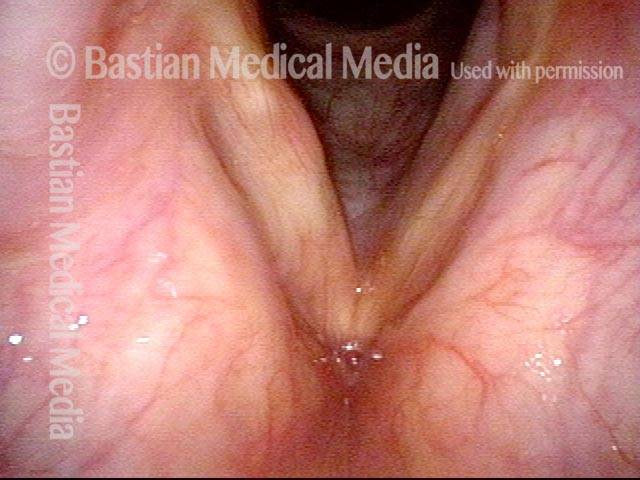
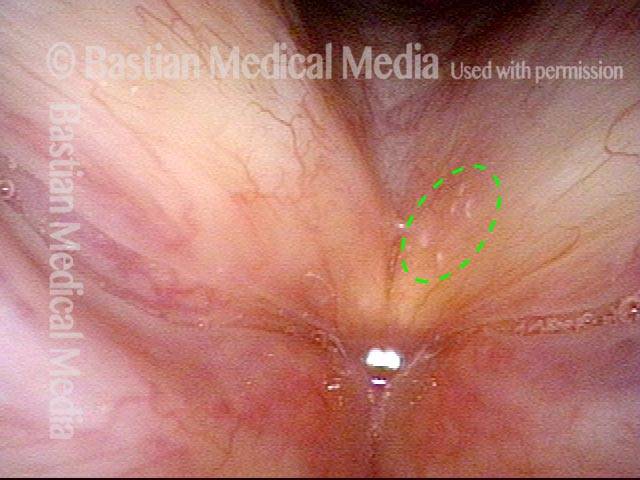
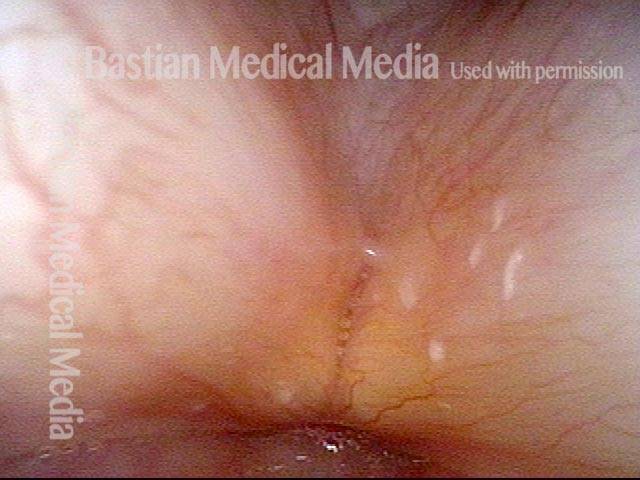
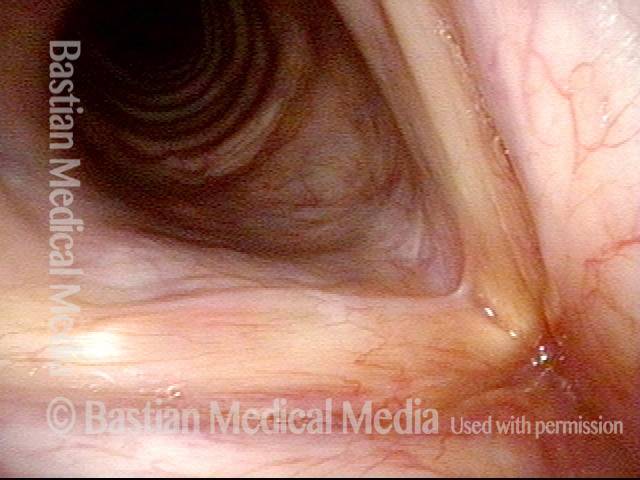
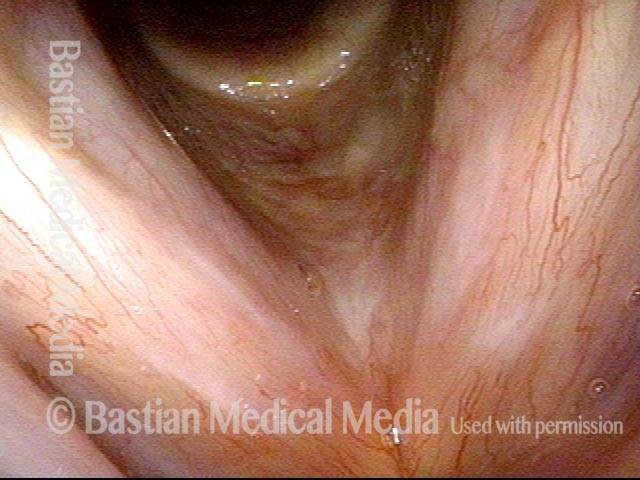
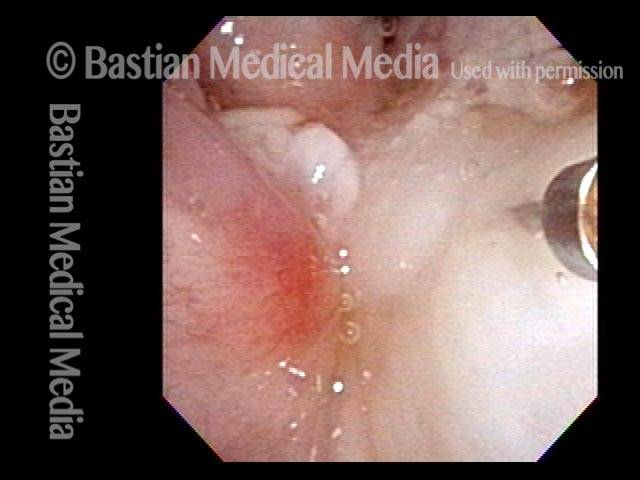
Capillary Ectasia, Before & After Laser Coagulation
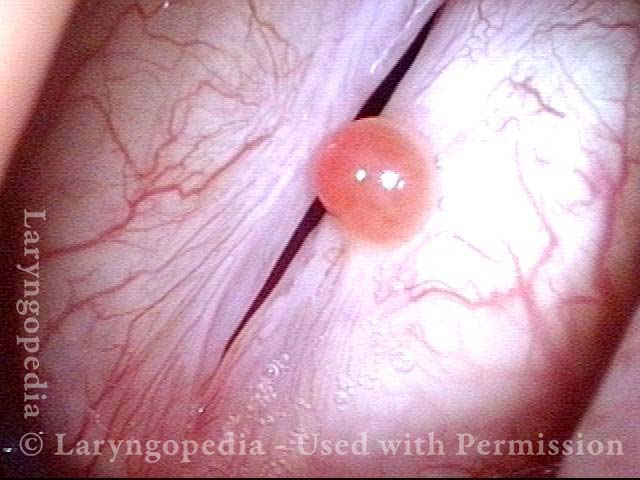
Capillary ectasia (1 of 3)
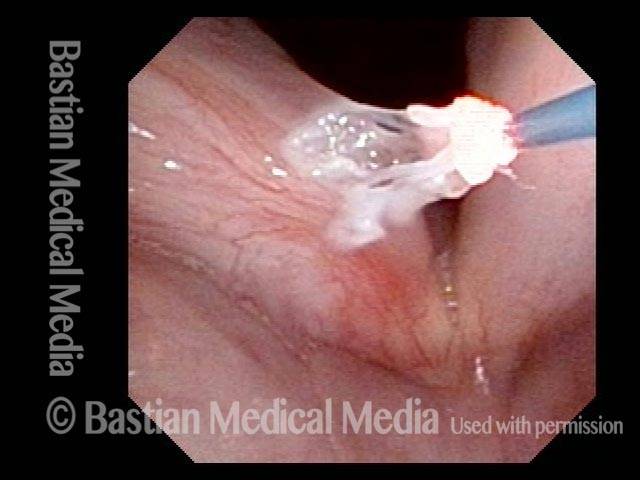
Capillary ectasia, right after laser coagulation (2 of 3)
Capillary ectasia, 6 weeks after laser coagulation (3 of 3)
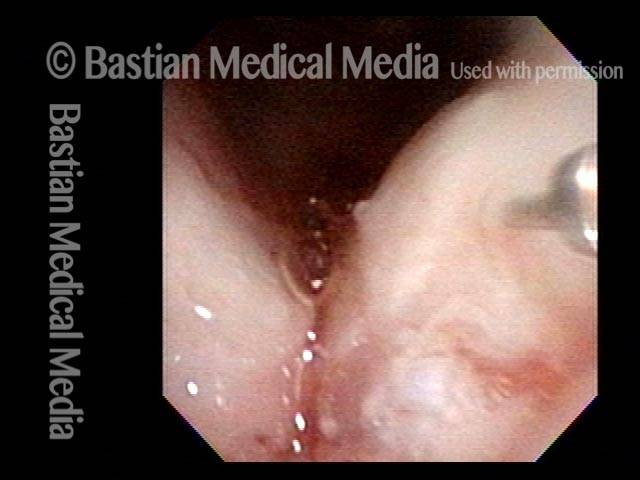
Lidocaine Injection for Aggressive “Office” Laser Treatments
Laser ablations performed in office (1 of 6)
Infiltrating anesthetic (2 of 6)
Thulium laser procedure (3 of 6)
Post-surgery (4 of 6)

Six weeks post-surgery (5 of 6)

Second laser sugery (6 of 6)
Perfect Candidate for Thulium Laser
Lesion (1 of 4)
Lesion under narrow-band light (2 of 4)
Coagulated with thulium laser (3 of 4)
Finishing up (4 of 4)

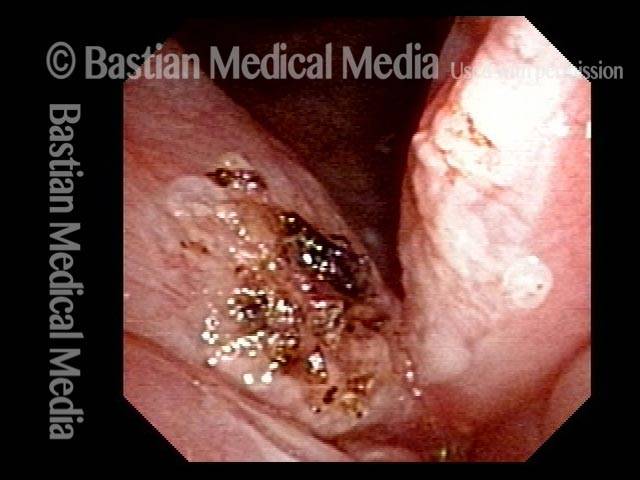
Leukoplakia Battled Over Time
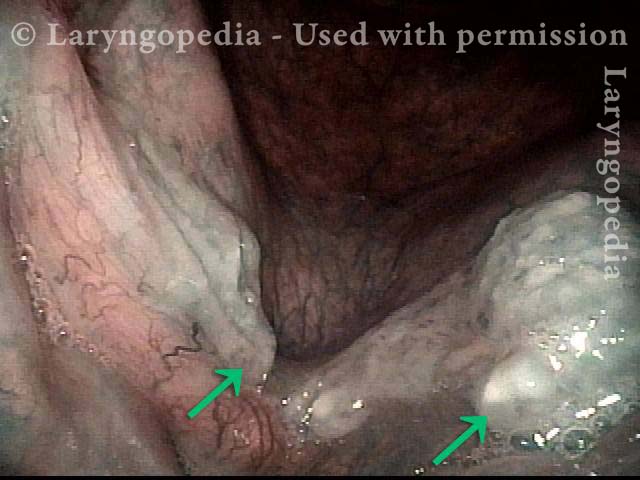
Leukoplakia (1 of 8)
Spilled Milk (2 of 8)

Thulium laser (3 of 8)
Coagulated tissue (4 of 8)
Leukoplakia (5 of 8)

Detachment (6 of 8)
Superficial vascular pattern (7 of 8)
Coagulated tissue (8 of 8)

Leukoplakia, Before, During, and After Laser Coagulation
Leukoplakia, not yet seen (1 of 6)
Leukoplakia (2 of 6)
Leukoplakia (3 of 6)
Leukoplakia, coagulated by laser (4 of 6)

Leukoplakia, 3 months after laser treatment (5 of 6)
Leukoplakia, 3 months after laser treatment (6 of 6)
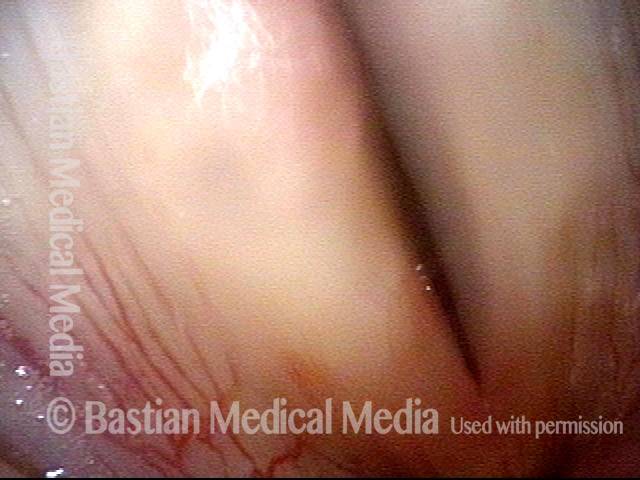
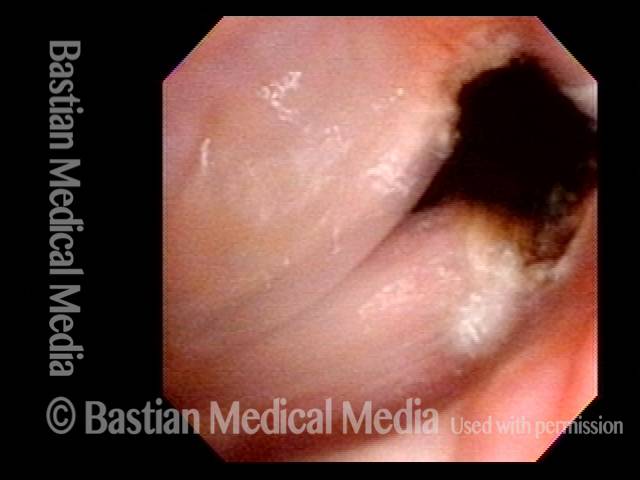
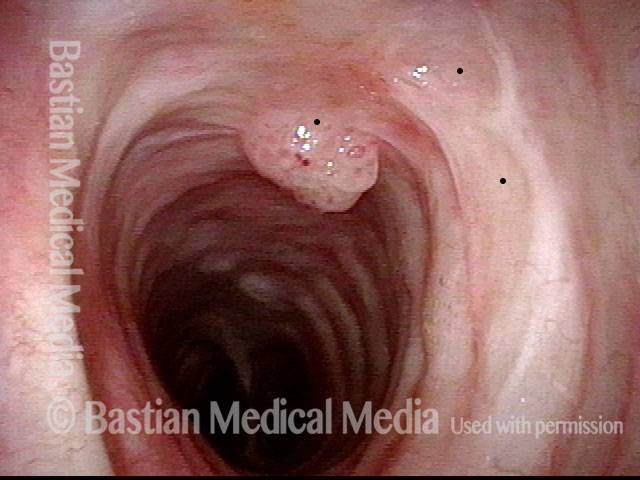
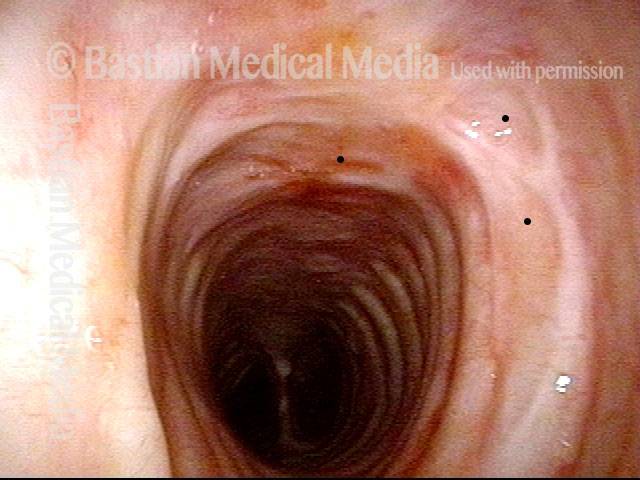
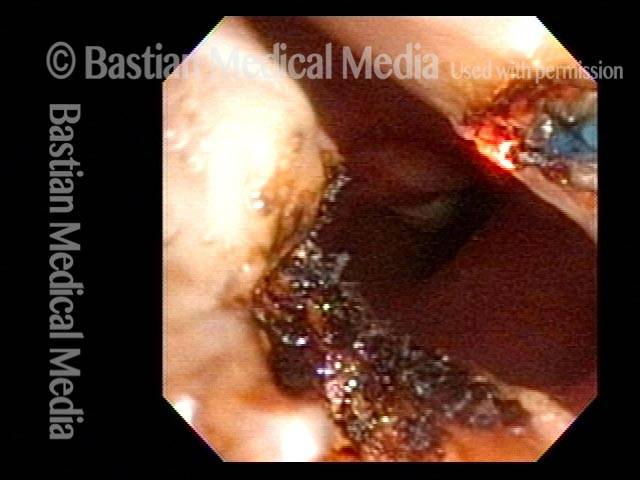
Mid-Tracheal Papilloma, Treated By Thulium Laser
Mid-tracheal papilloma, being treated by thulium laser (1 of 5)
Months after treatment: no papilloma (5 of 5)
Mid-tracheal papilloma, being treated by thulium laser (2 of 5)
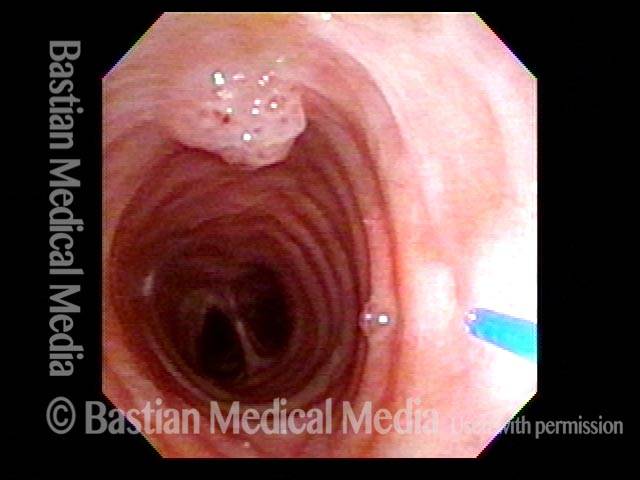
Mid-tracheal papilloma, being treated by thulium laser (3 of 5)

Mid-tracheal papilloma, being treated by thulium laser (4 of 5)

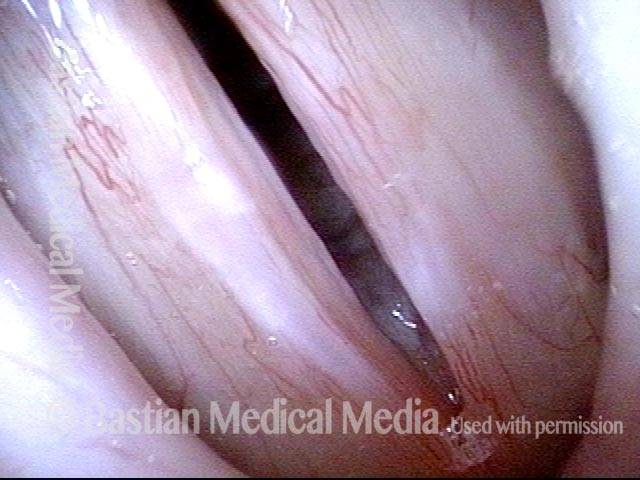
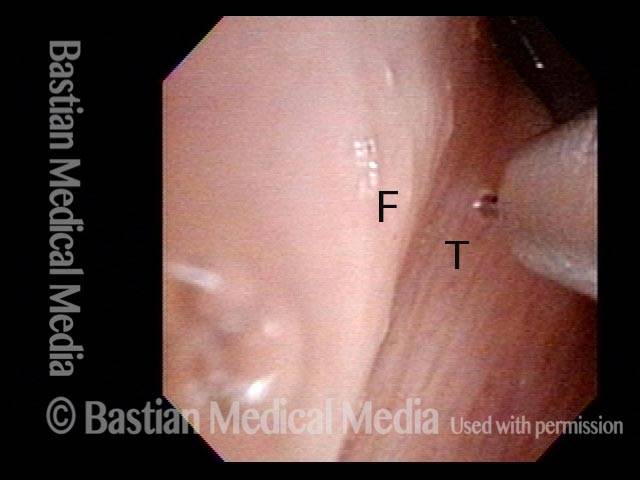
Capillary Ectasia and Hemorrhagic Polyp, Treated by Thulium Laser
Capillary ectasia and hemorrhagic polyp (1 of 7)
Capillary ectasia and hemorrhagic polyp (2 of 7)
Capillary ectasia and hemorrhagic polyp, thulium laser treatment (3 of 7)

Capillary ectasia and hemorrhagic polyp, thulium laser treatment (4 of 7)

Capillary ectasia and hemorrhagic polyp, after treatment (5 of 7)
Vocal cord margin (6 of 7)

Capillary ectasia and hemorrhagic polyp, after treatment (7 of 7)
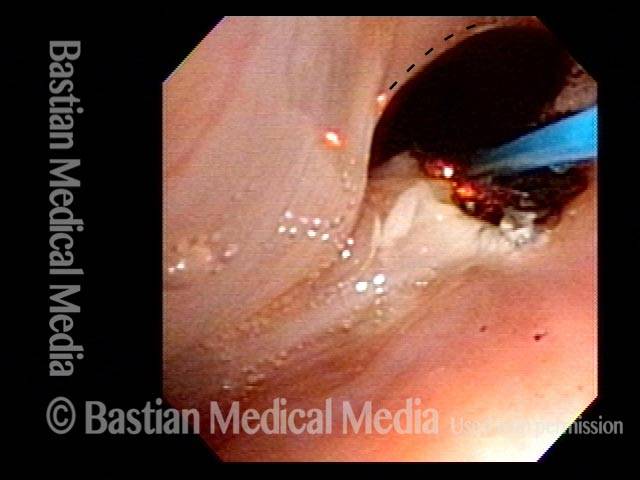
Thulium Laser Surgery, With Local Anesthetic Injection, to Treat Leukoplakia
Leukoplakia, about to be treated with laser (1 of 4)

Injection of local anesthetic (2 of 4)
Injection of local anesthetic (3 of 4)
Right after thulium laser treatment (4 of 4)

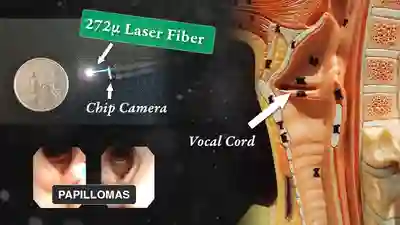
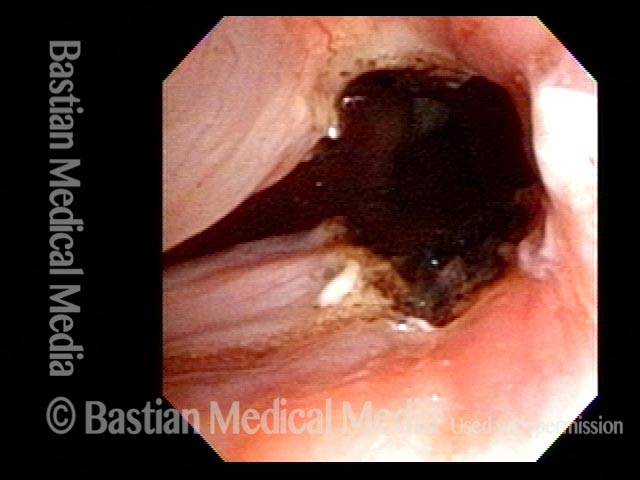
Tracheal Papillomas and the Thulium Laser
HPV 11 (1 of 2)

Post laser coagulation (2 of 2)

Office-Based Surgery When General Anesthesia Is too Risky
Involuntary inspiratory voice (1 of 6)

Laser posterior commissuroplasty (2 of 6)
During the commissuroplasty (3 of 6)
Deepening divot (4 of 6)
Inspiratory indrawing decreased (5 of 6)
Phonation (6 of 6)