Symptoms and Risks
RRP can be life-threatening in young children, if not carefully followed and treated, since a child’s airway is relatively narrow and can potentially be obstructed completely by the disease’s proliferative growths; moreover, RRP in children tends to grow and recur more aggressively.
In adults, RRP will usually only impair voice function (when the growths occur on the vocal cords), though it can also impair breathing in severe cases. Occasionally, RRP can also progress to cancer, and therefore patients found to be at high risk for this (see below) need to be monitored carefully.
Characteristics of RRP Growths
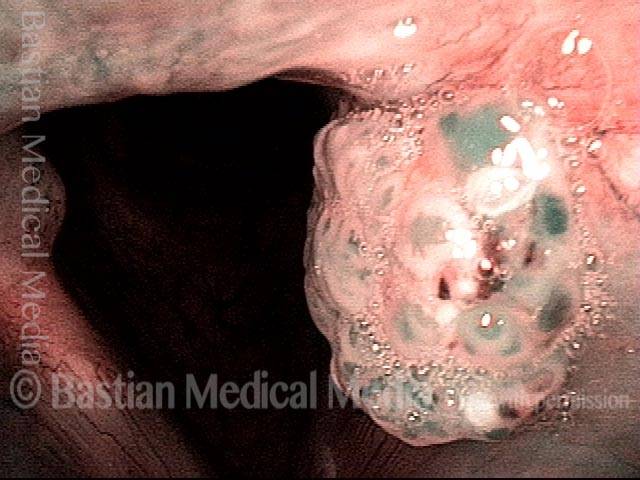
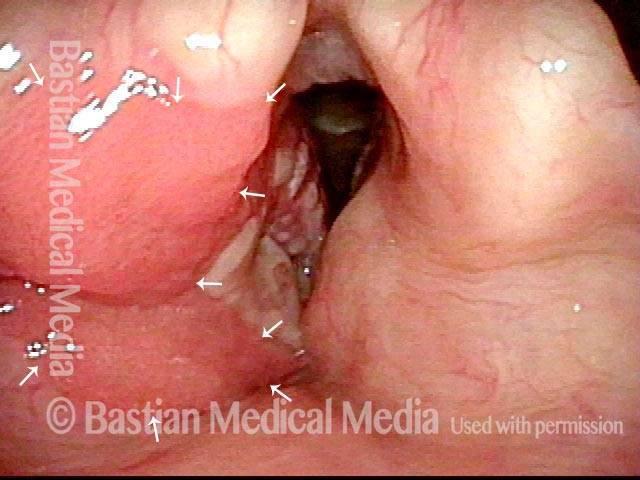
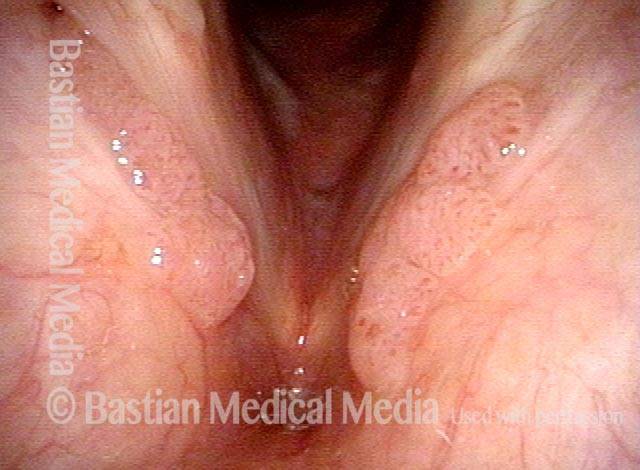
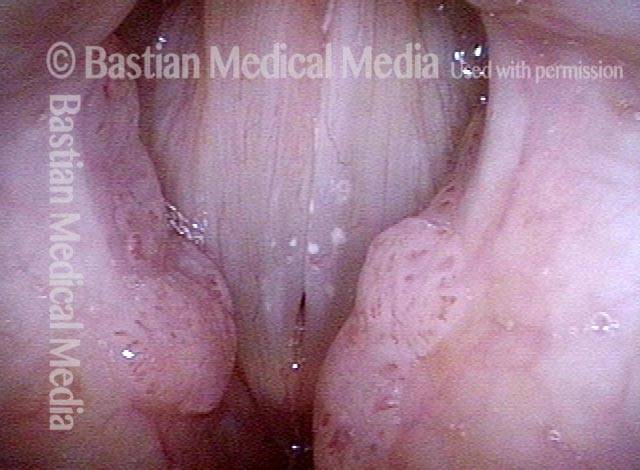
The growths usually associated with RRP are wart-like tumors, or papillomas, that protrude conspicuously from the surface on which they grow, often in grape-like clusters. These kinds of papillomas are usually seen in patients who have HPV subtypes 6 or 11, which are both lower-risk subtypes for incurring cancer.
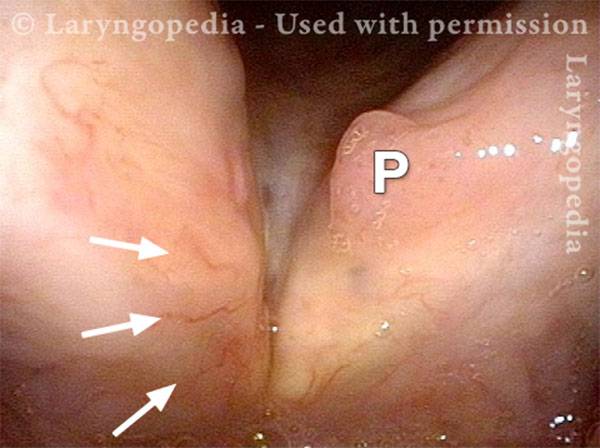
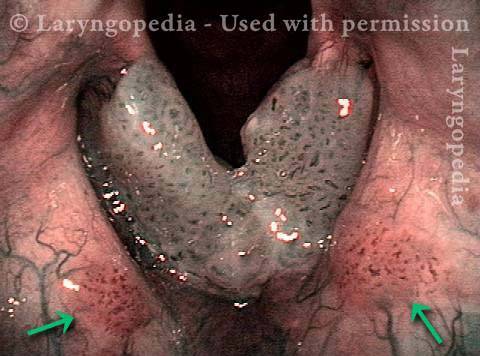
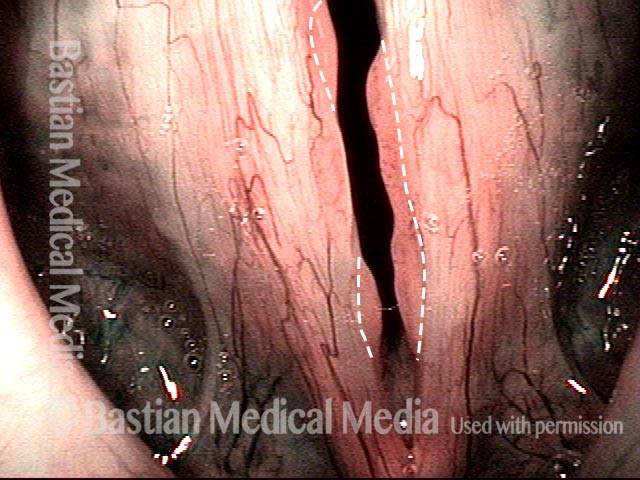
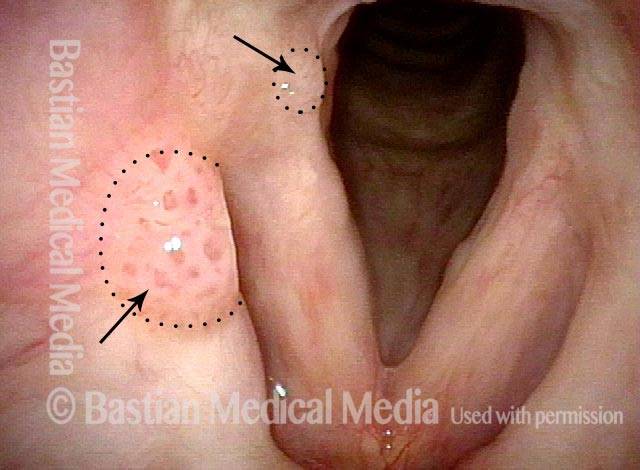
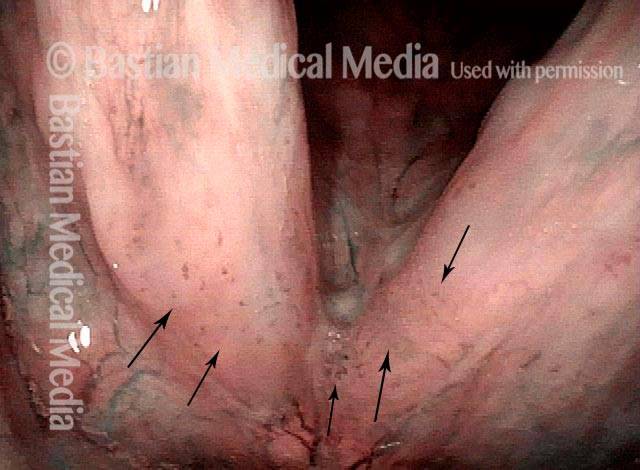
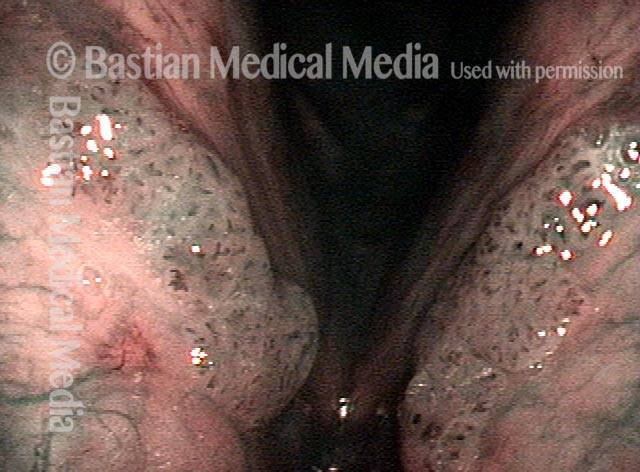
There are some HPV patients, however, who manifest their HPV infection with subtler, velvety growths within the airway—“carpet-variant” growths, so to speak. Although these “carpet-variant” growths do not have the wart-like appearance of the papillomas typically associated with RRP, there at least a few key points of similarity:
- Both the “carpet-variant” and wart-like growths are lesions that sometimes appear, either independently or together, in patients who have HPV;
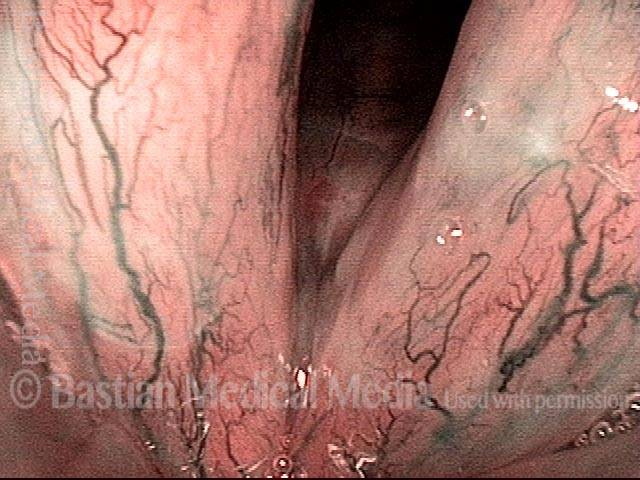
- Both the “carpet-variant” and wart-like growths are stippled with polka-dot vascular markings, because each “loop” in the “carpet” or each “grape” in the wart-like cluster has its own fibrovascular core, seen as a red dot;
- Both the “carpet-variant” and wart-like growths can disrupt voice function;
- Both the “carpet-variant” and wart-like growths usually recur if they are removed.
Because of these similarities, we consider these “carpet-variant” growths, even when the sole expression of the infection, to be at least a cousin to RRP, within the family of HPV-induced lesions. Many patients with this “carpet-variant” condition have HPV subtypes such as 16 or 18 that are higher-risk for cancer; such patients need to be monitored with particular care.
Treatment Methods
The primary treatment for RRP and other HPV-induced lesions is careful, conservative surgical removal of the growths. Because these growths almost always recur, surgery must usually be performed on a repeated basis, as frequently as every few weeks in children, but on average much less often in adults.
A common interval between surgeries for adult patients is between every six months and every two years, depending on how quickly the RRP or other HPV-related lesion recurs and impairs the patient’s voice function again.
There are also a few medical treatments that have been used in addition to surgery, including, among others, interferon, indole-3-carbinol, intralesional mumps or MMR (measles-mumps-rubella) vaccine, cidofovir, and bevacizumab.
“Curative” vs. “Management” Modes of Treatment
It is possible to approach the surgical management of RRP with two different strategies: either “curative” or management mode.
Often new patients, especially those who have required frequent surgery previously, choose to pursue the former (“curative”) strategy. They of course know that RRP is considered a chronic and recurring disease process. We stress that reality, but also tell them that we have seen a small subset of patients remit because of a “curative mode” trial, and such patients may have no visible disease for many years. This seems more possible for those with focal, or discrete multifocal papillomas.
Or, we explain, by following the “curative mode” we may “win territory but not the war.” That means that the recurring papillomas may involve a smaller area than before.
Or, we also explain, they may achieve longer intervals between procedures, because the disease is calmed down from aggressively-recurring to indolent (lazy).
We explain to these patients that the word “curative” is in quotes to signify we are pursuing “cure” as a strategy but cannot know in advance if that will be their outcome. And even when it appears that we have vanquished the disease, we continue to refer to it as “in remission” rather than cured, because of a few who re-developed papillomas years after appearing to be “cured.”
What Is the “Curative” Mode Strategy?
We suggest 3 operating room (O.R.) microlaryngoscopy procedures, 4 to 6 weeks apart, to remove papillomas using a “basement membrane peel” technique, with use of an adjuvant (either cidofovir or bevacizumab).
Even if disease is minimal and voice is excellent, we complete the series of three treatments and then pause to see what happens. If lesions recur fairly promptly, we may in highly motivated patients do another three treatments with the alternate adjuvant (cidofovir or bevacizumab). Otherwise, we will move to management mode.

What Is the Management Mode Strategy?
Here, we intervene with another microlaryngoscopy according to patient vocal needs. We don’t operate based upon visible lesions, but instead on degree of hoarseness. The patient might be examined every six months without necessarily undergoing surgery if they have a high-risk subtype such as 16, or 18, etc. But if they have type 6 or 11, we may see them yearly, or even only when they feel the need due to voice deterioration.
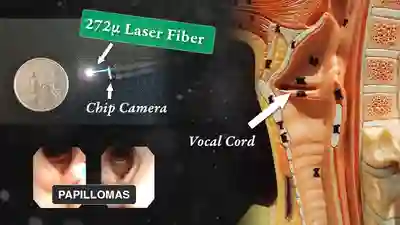
How does the Office Laser Option fit into the Modes of Treatment?
We don’t see office laser treatment as fitting into the “curative mode” because it is less definitive in its removal of papillomas. That is, while we can do a “99%” removal in the OR, we think more of an “80%” reduction in the office to diminish the disease and improve voice, without going to the O.R.

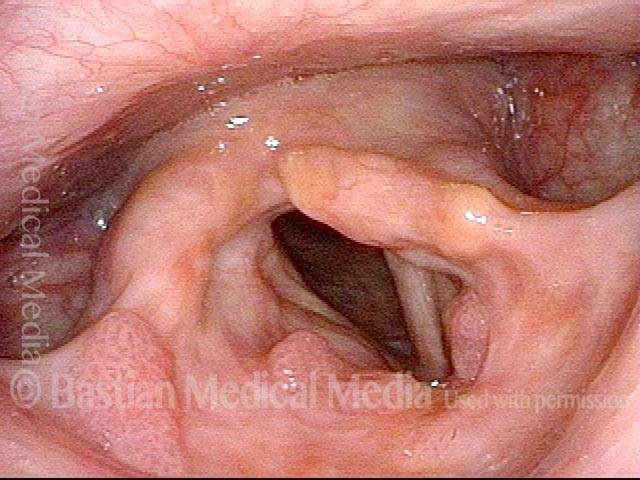
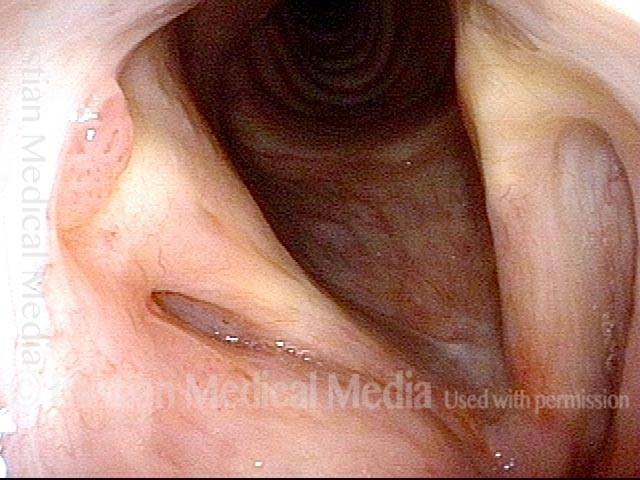
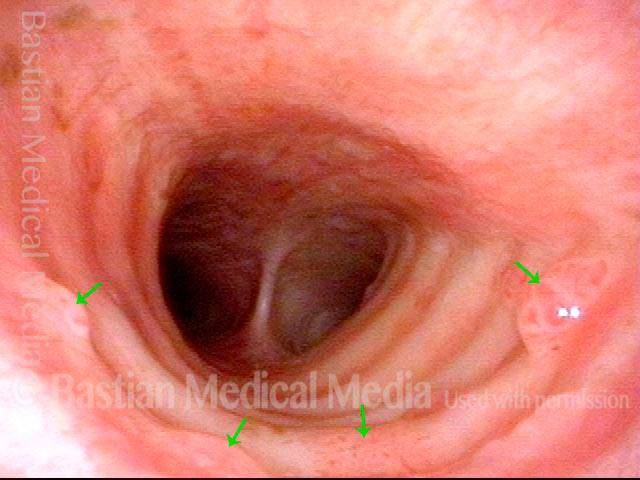
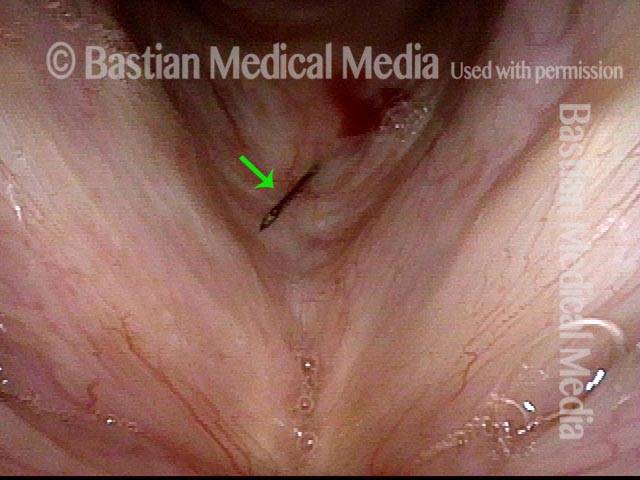
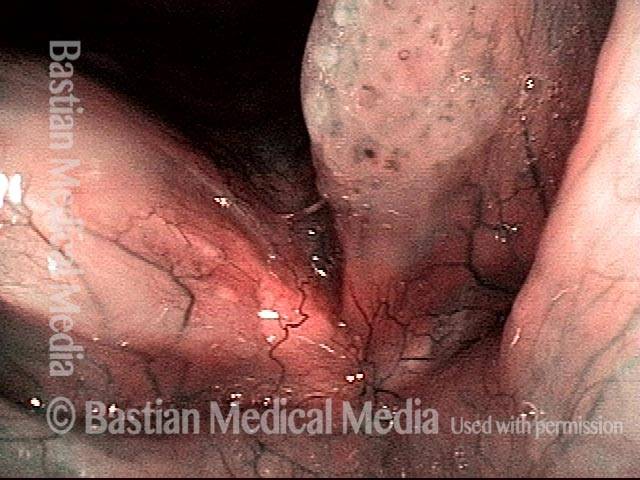
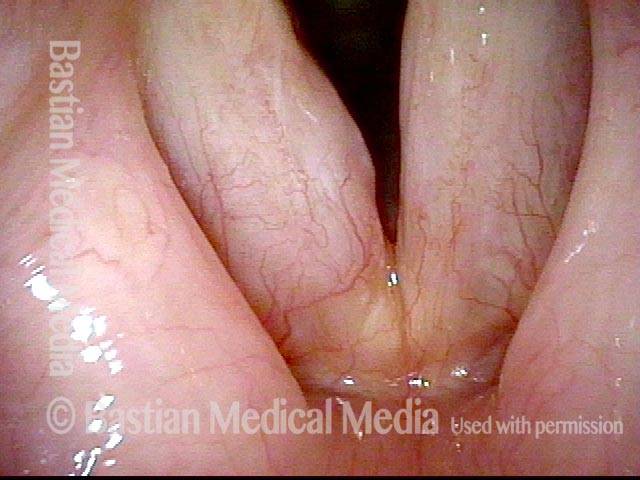
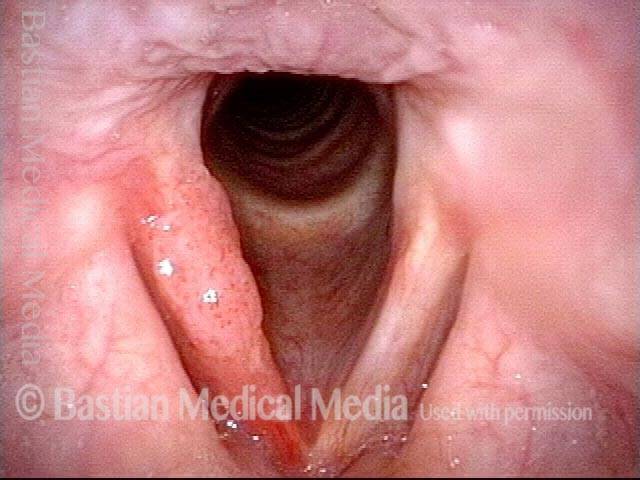
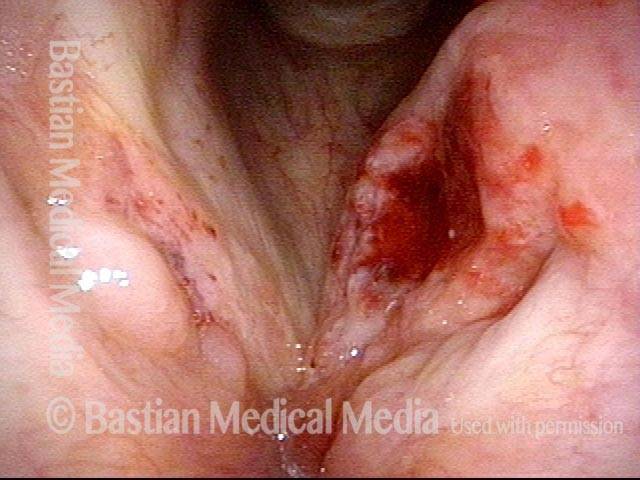
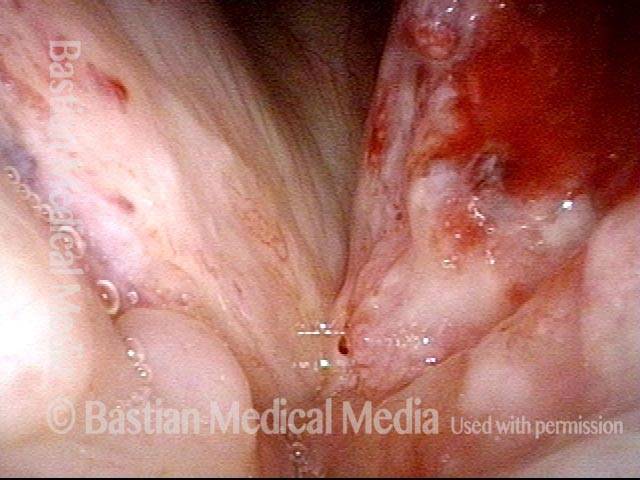
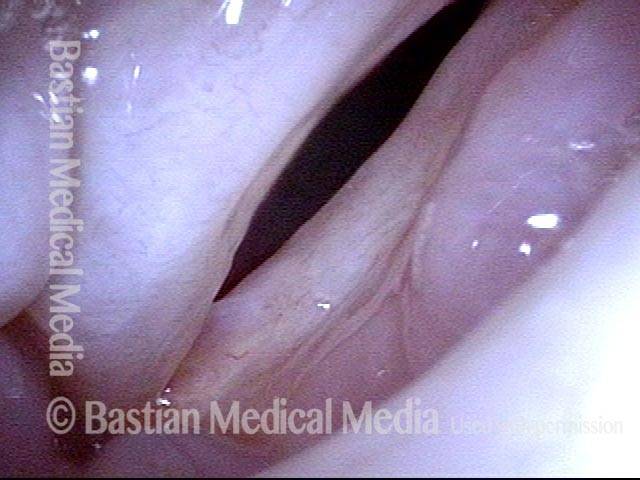
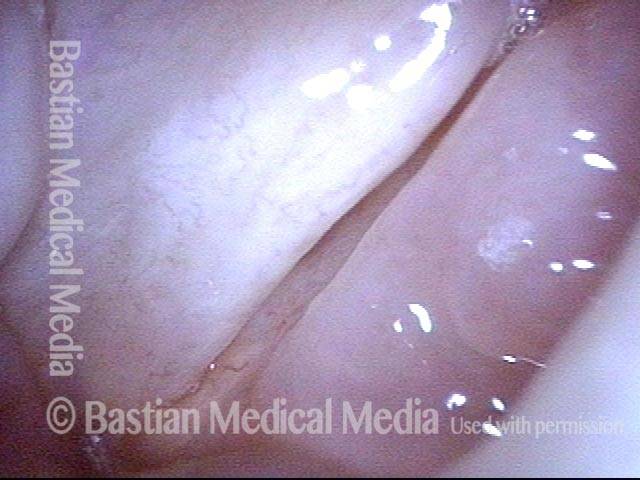
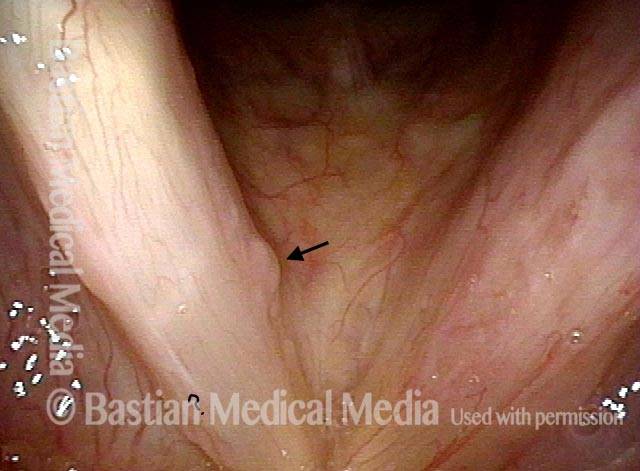
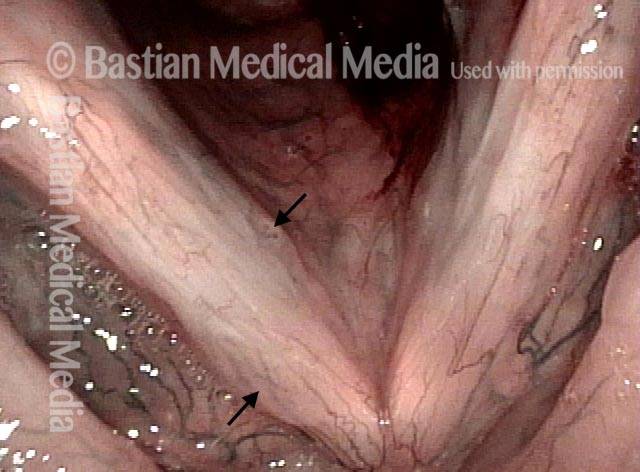
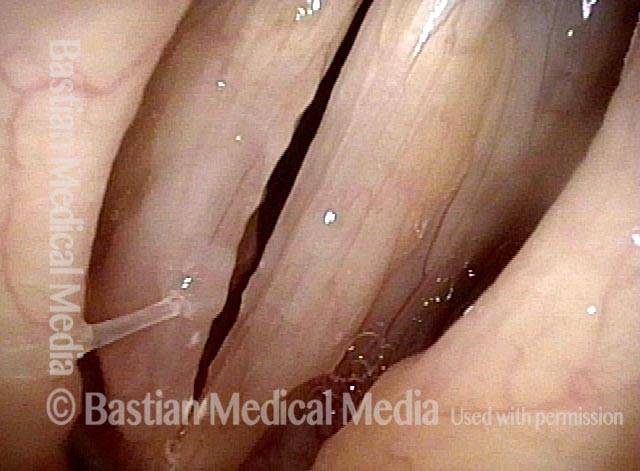
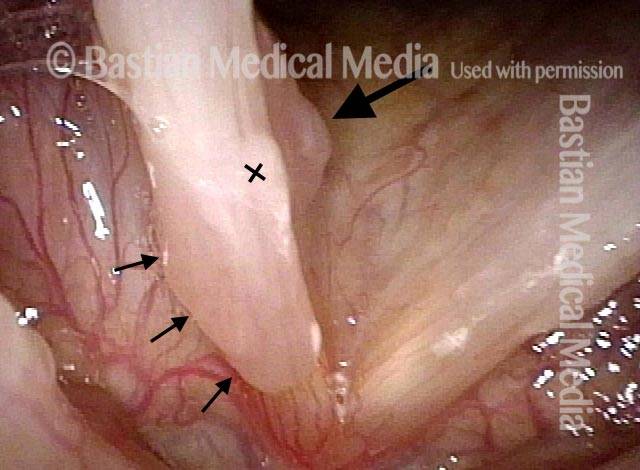
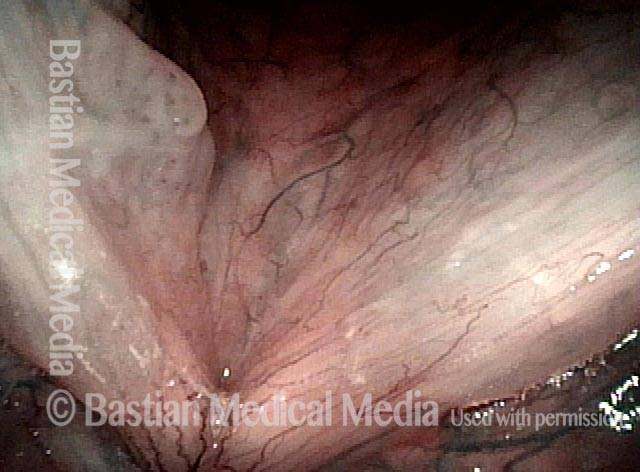
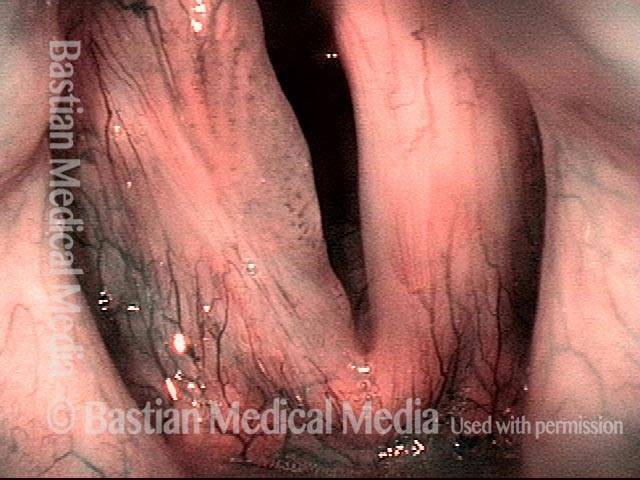
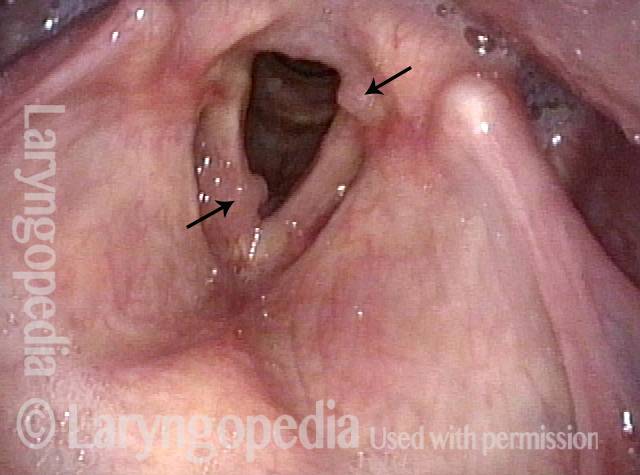
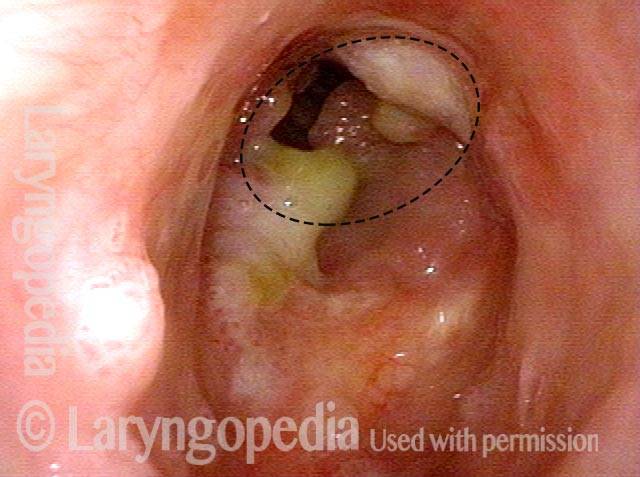
Removing Papilloma from Severely Scarred Vocal Cords
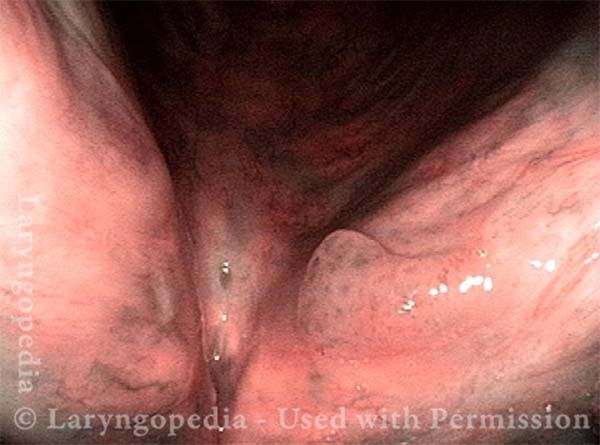
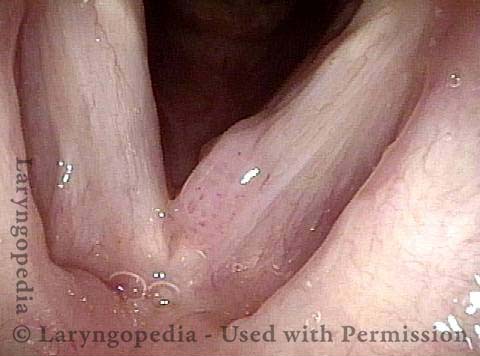
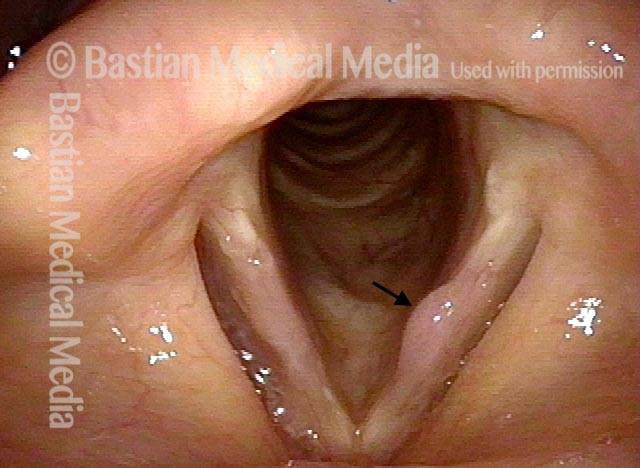
This older patient has undergone multiple procedures elsewhere for laryngeal papillomas (RRP). His voice remains hoarse and effortful, not only due to scarring from previous surgeries but also because of a projecting papilloma on the left vocal cord. In such cases, meticulous surgical technique is essential to prevent additional scarring and preserve vocal function.
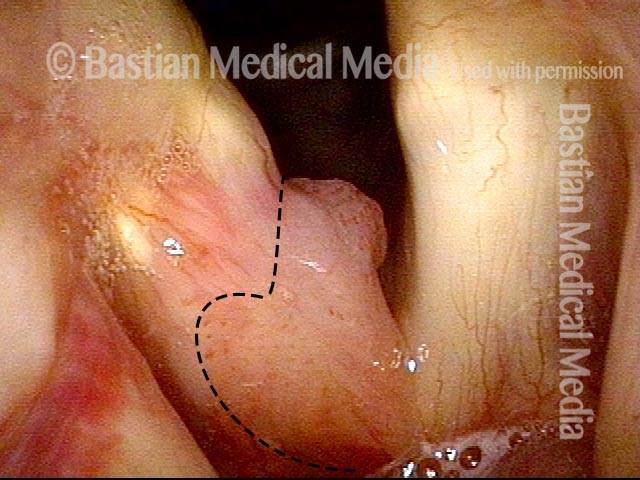
Projecting Papilloma (1 of 7)
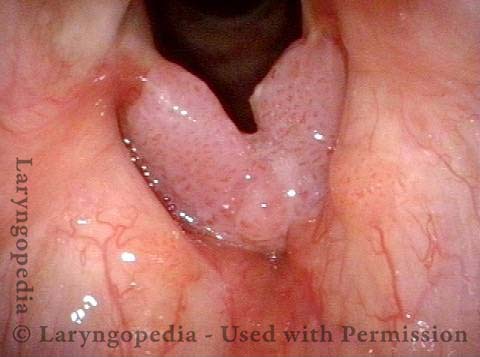
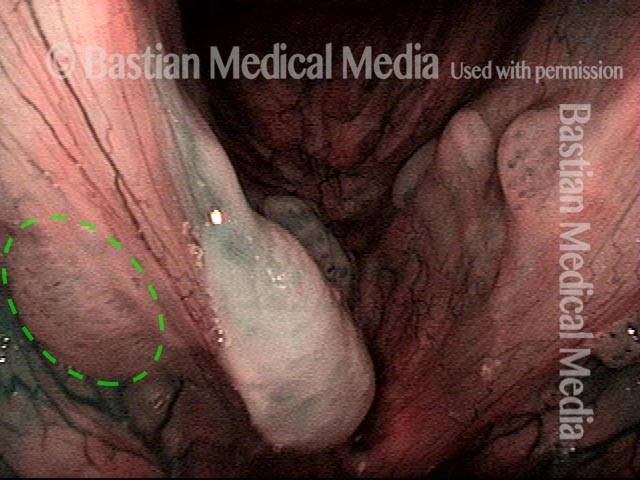
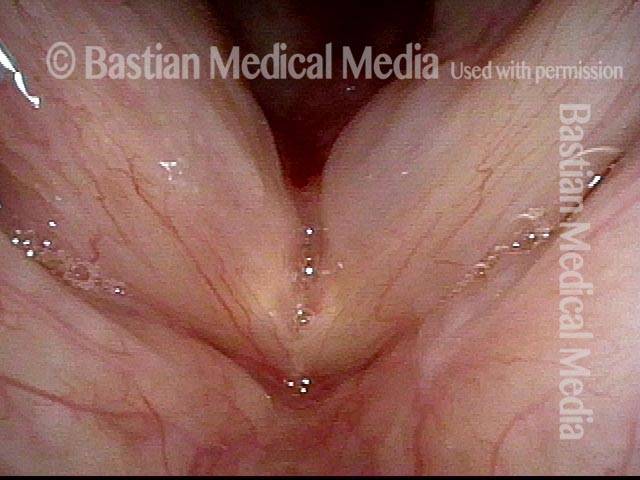
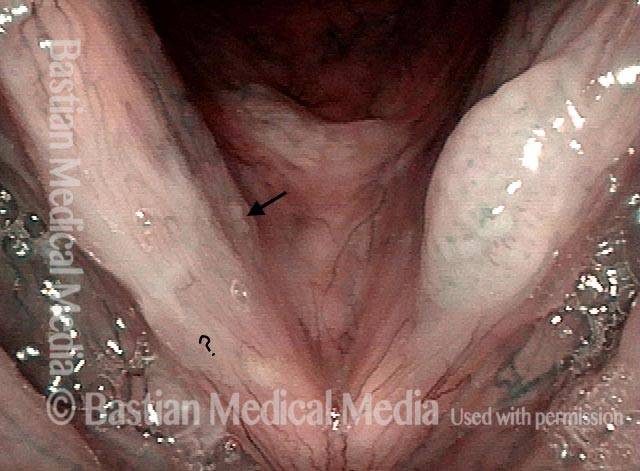
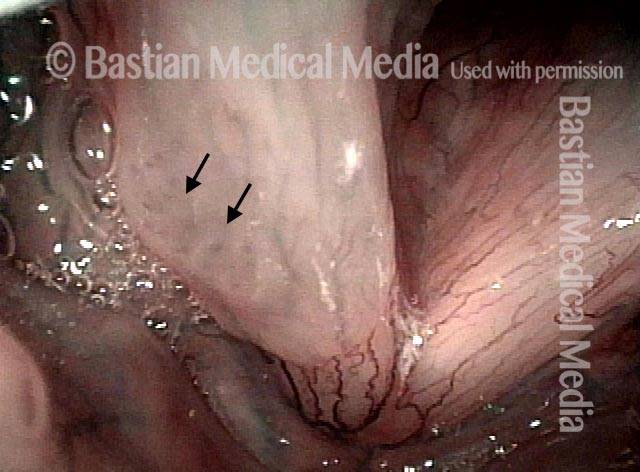
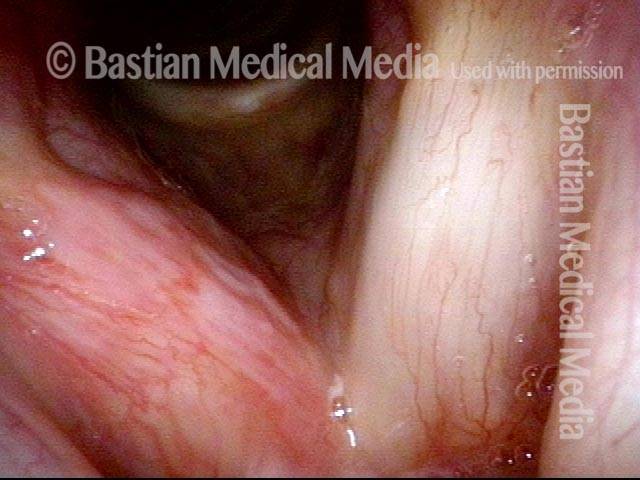
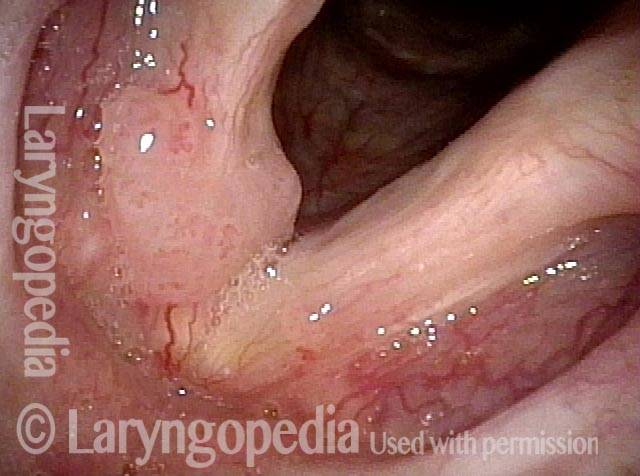
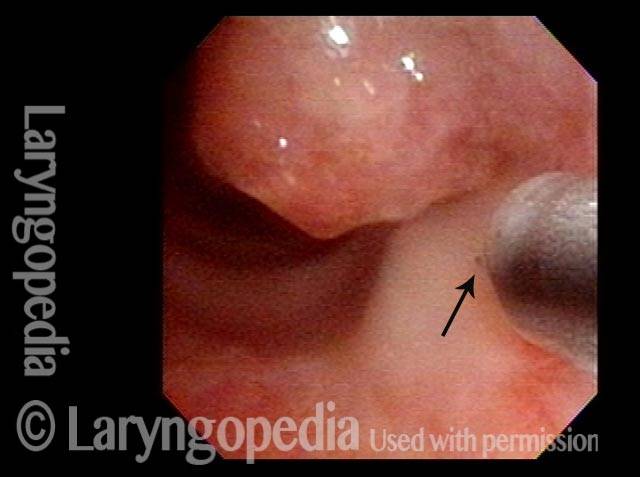
Stippled vascularity (2 of 7)
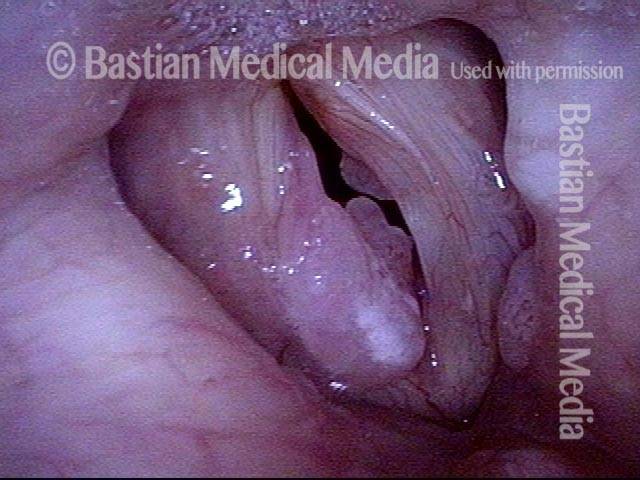
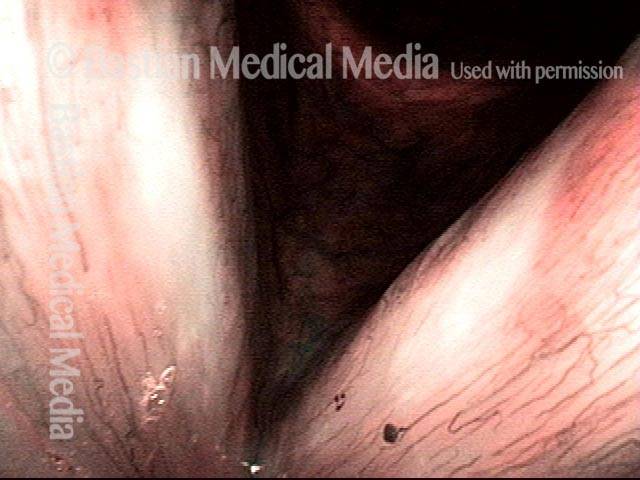
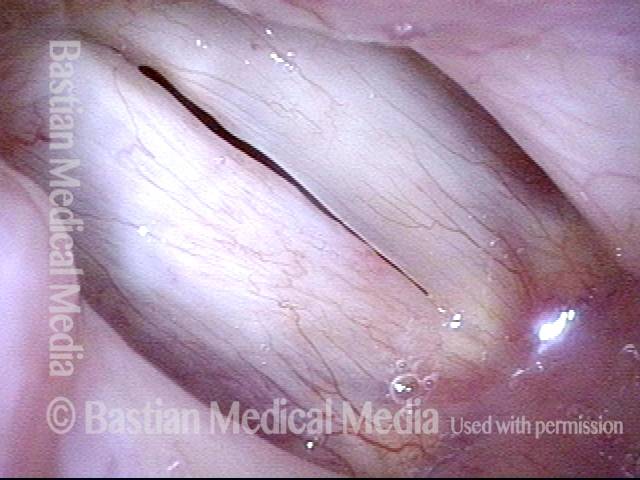
Bowing vocal cord (3 of 7)
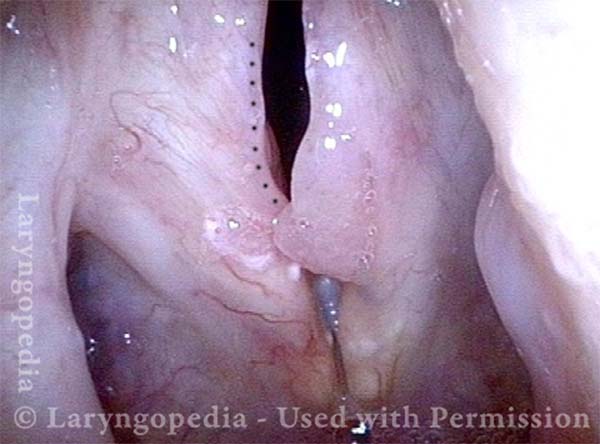
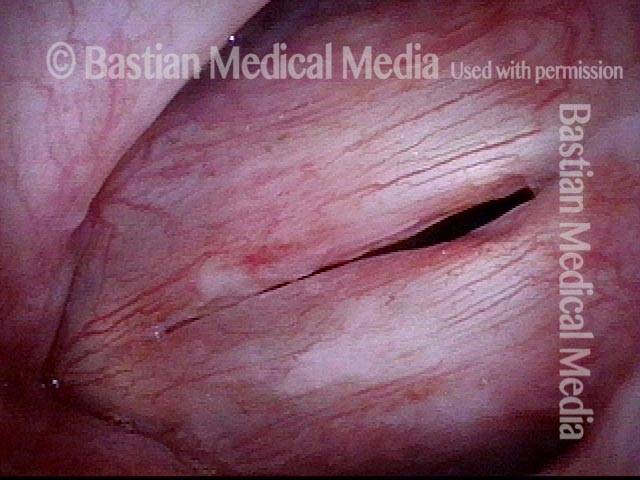
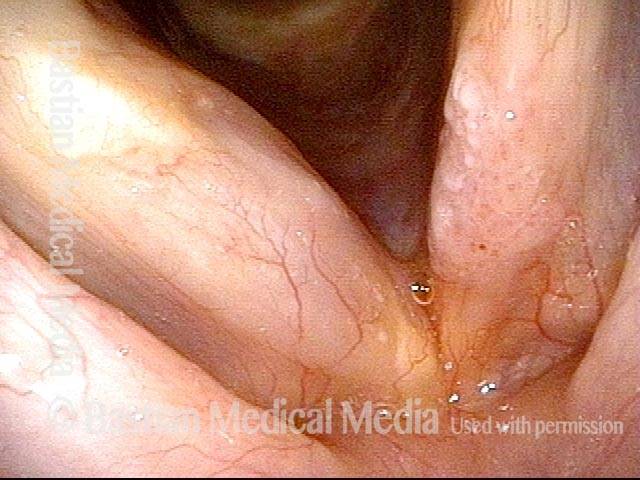
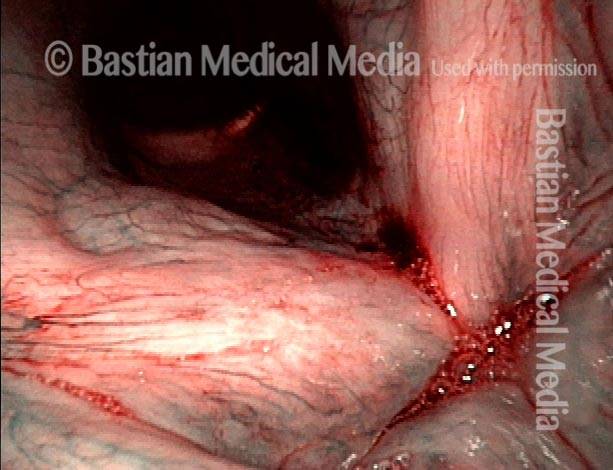
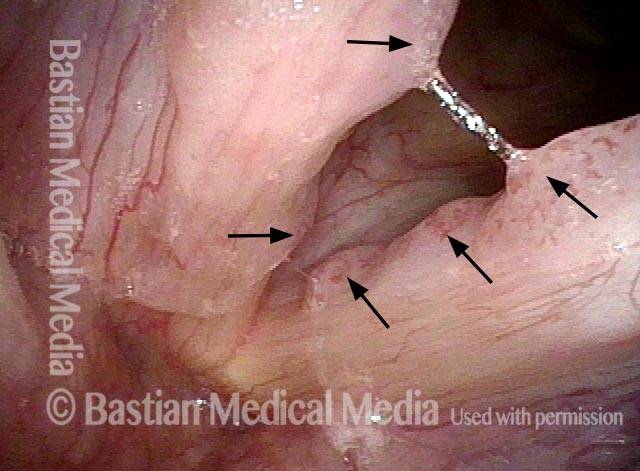
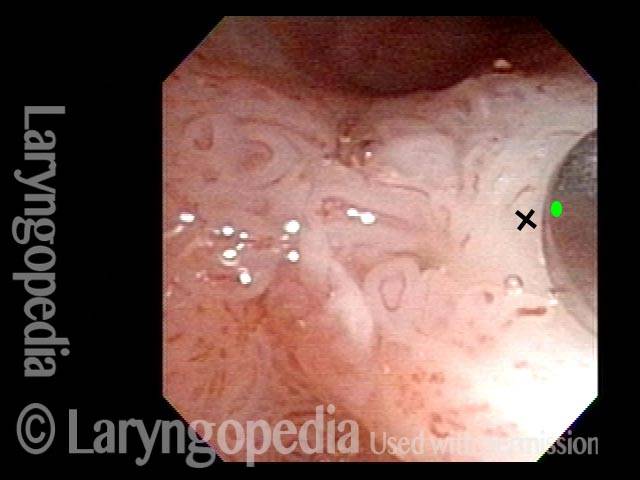
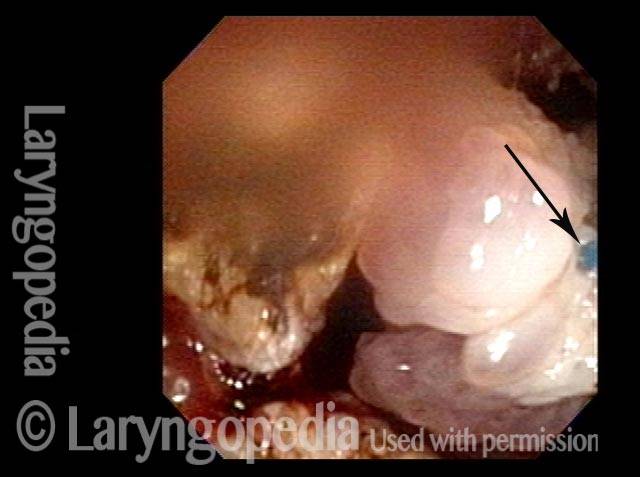
Surgical view (4 of 7)

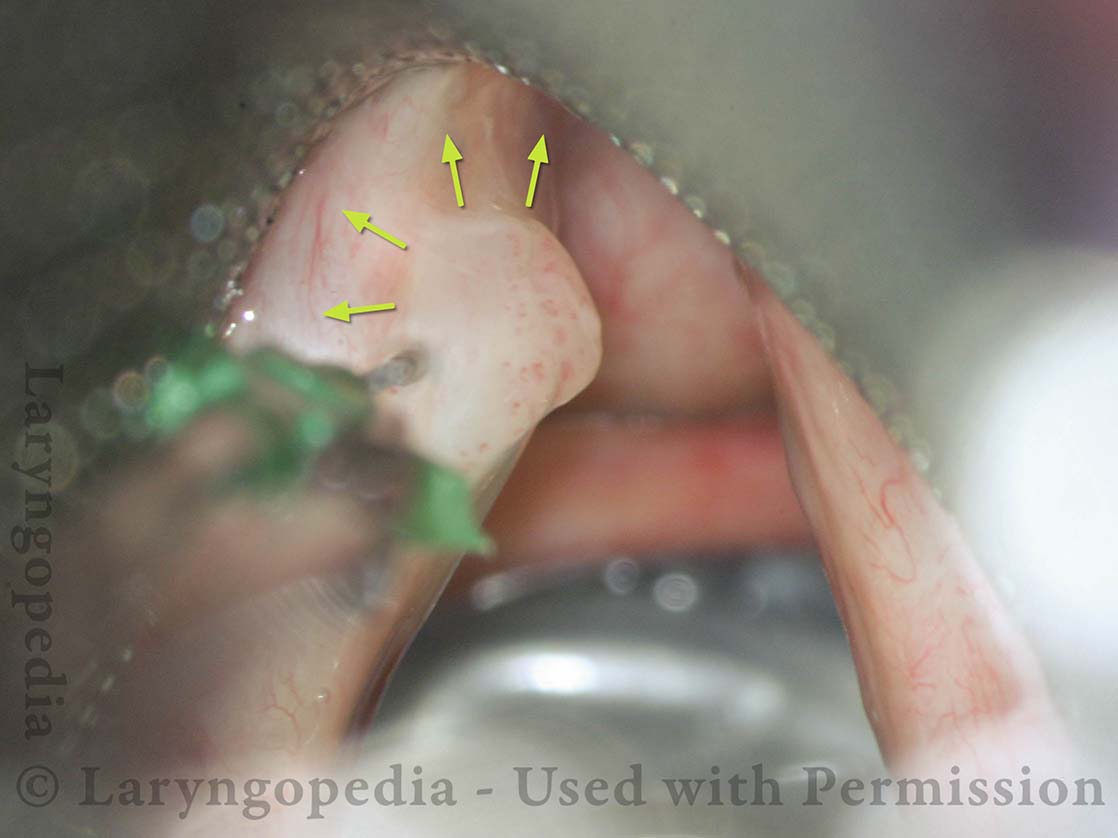
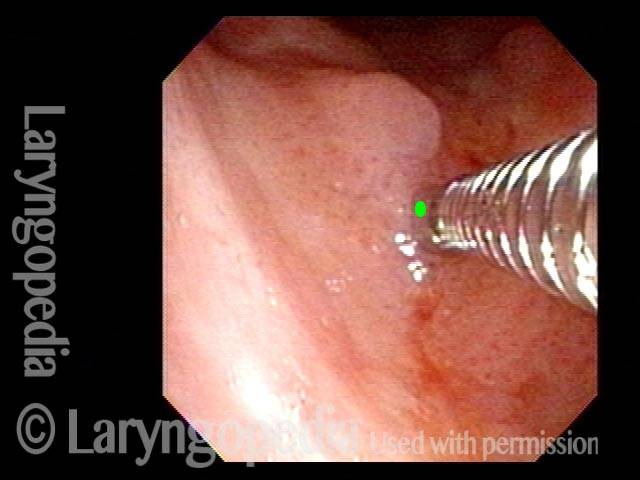
Cidofovir Injection (5 of 7)
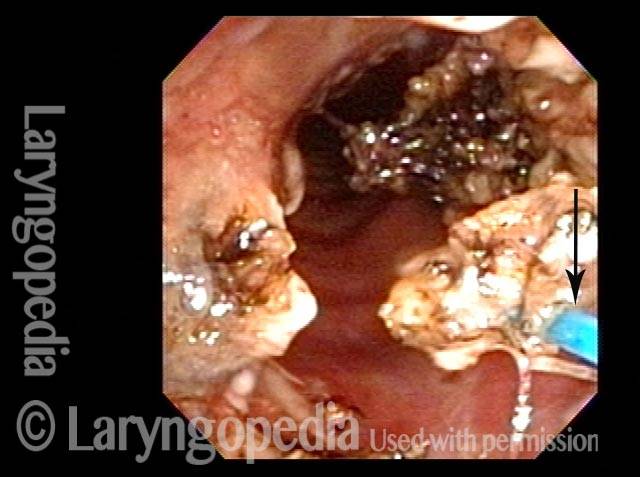
Papilloma removal (6 of 7)

Scarred tissue (7 of 7)

Humility Before the HPV Virus—A Recurrence of Papillomas at Ten Years
HPV infection is considered chronic, and causes recurrent growth of papillomas in the larynx. Still, we sometimes see what appear to be cures, or at least long-term remissions. That appears to be the case here.
After an 8 year interval of perfect voice, the patient had a sudden increase of hoarseness occurring in the few weeks prior to the last examination below. This is an illustration of why we often say to a patient who appears to be cured, “You may be cured, but we usually say “long term remission.” This patient’s scenario is not rare.
Was her longterm, 8-year remission due to meticulous surgery? Cidofovir? Her immune response? It is impossible to say if it was one or all of these factors.
Stippled Vascularity (1 of 8)
HPV infection (2 of 8)
Stippled vascularity (3 of 8)

HPV vascular effect (4 of 8)

16 months later (5 of 8)
Is it long-term remission? (6 of 8)

Recurrent Papilloma (7 of 8)
Stippled vascularity (8 of 8)

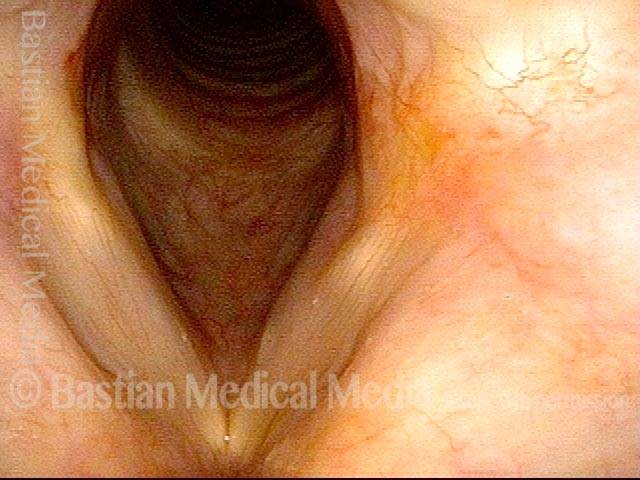
Papillomas, HPV Subtype 11, before and After Removal
Papillomas: HPV Subtype 11 (1 of 4)

Papillomas: HPV Subtype 11 (2 of 4)
Papillomas, removed: HPV Subtype 11 (3 of 4)
Papillomas, removed: HPV Subtype 11 (4 of 4)

Papillomas, HPV Subtype 6, Before and after Removal
Papillomas: HPV Subtype 6 (1 of 4)

Papillomas: HPV Subtype 6 (2 of 4)

Papillomas, removed: HPV Subtype 6 (3 of 4)

Papillomas, removed: HPV Subtype 6 (4 of 4)
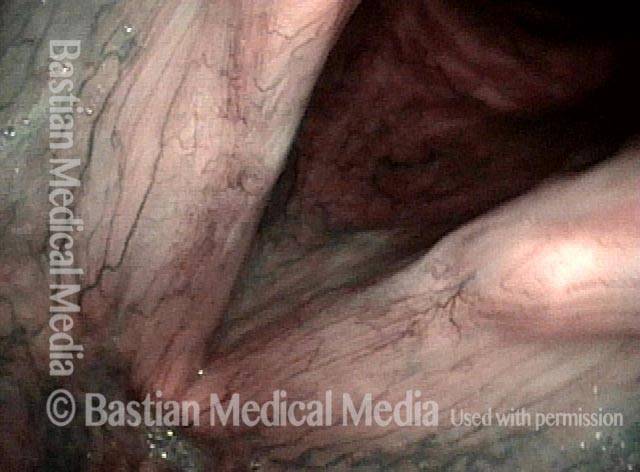
Papillomas, HPV Subtype 11
Papillomas: HPV Subtype 11 (1 of 3)
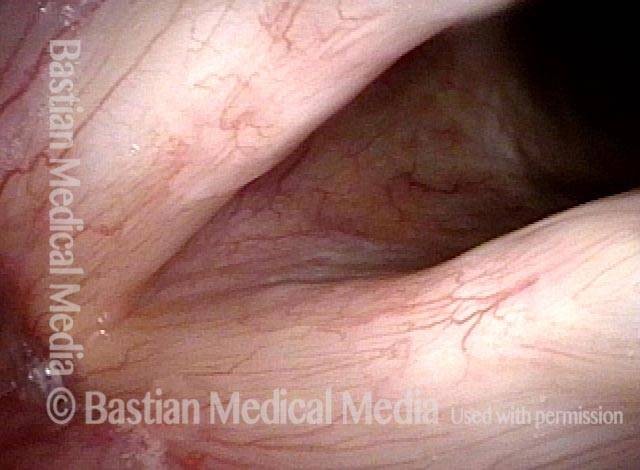
Papillomas: HPV Subtype 11 (2 of 3)
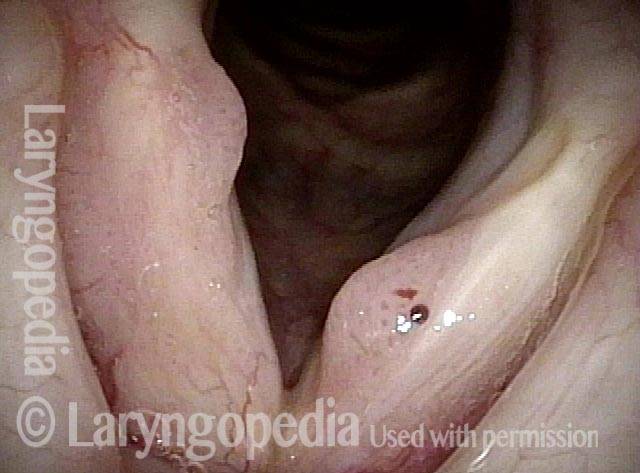
Papillomas: HPV Subtype 11 (3 of 3)

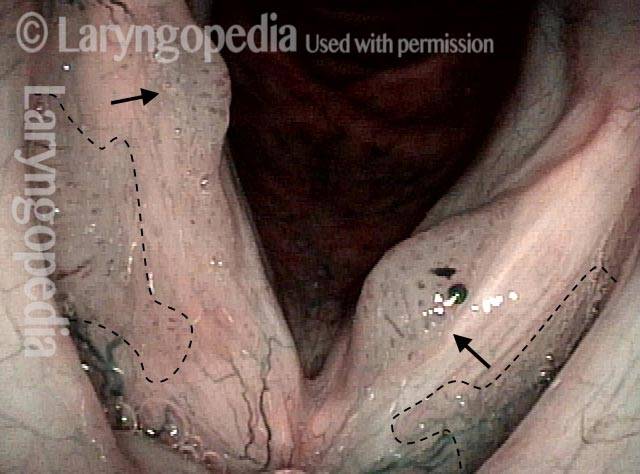
Example 2
Papillomas: HPV Subtype 11 (1 of 2)

Papillomas: HPV Subtype 11 (2 of 2)
HPV Lesions
Lesions of HPV Subtype? (1 of 2)

Lesions of HPV Subtype? (2 of 2)

Lesions and Papillomas of HPV, Before and After Removal and Adjuvant Injection
Lesions and papillomas of HPV subtype? (1 of 8)

Subtle lesion (2 of 8)
Open phase (3 of 8)
1 week after removal (4 of 8)

1 week after removal (5 of 8)
Injecting adjuvant (6 of 8)
After injecting adjuvant (7 of 8)
After final adjuvant injection (8 of 8)

Papillomas, HPV Subtype 55, Going Into Remission
Papillomas: HPV Subtype 55 (1 of 4)

Papillomas: HPV Subtype 55 (2 of 4)

Papillomas, in remission: HPV Subtype 55 (3 of 4)

Papillomas, in remission: HPV Subtype 55 (4 of 4)
Papillomas, HPV Subtype 31, Going Into Remission
Papillomas: HPV Subtype 31 (1 of 4)
Papillomas: HPV Subtype 31 (2 of 4)
Papillomas, in remission: HPV Subtype 31 (3 of 4)
Papillomas, in remission: HPV Subtype 31 (4 of 4)

Papillomas, HPV
Papillomas: HPV Subtype? (1 of 2)

Papillomas: HPV Subtype (2 of 2)

Pushing Past Red Herrings to Find the Real Issue
Obvious lesion not important (1 of 3)

Granuloma (2 of 3)

Carpet-varient papilloma (3 of 3)

Papillomas, HPV Subtype 18 or 45
Papillomas: HPV Subtype 18 or 45 (1 of 2)
Papillomas: HPV Subtype 18 or 45 (2 of 2)

Lesions of HPV Subtype 16
Lesions of HPV Subtype 16 (1 of 3)

Lesions of HPV Subtype 16 (2 of 3)

Lesions of HPV Subtype 16 (3 of 3)

Cancer, HPV Subtype 16, Before and After Radiation
Cancer: HPV Subtype 16 (1 of 5)
Cancer: HPV Subtype 16 (2 of 5)
Cancer: HPV Subtype 16, after radiation therapy (3 of 5)

Cancer: HPV Subtype 16, after radiation therapy (4 of 5)
Cancer: HPV Subtype 16, after radiation therapy (5 of 5)
Papillomas, HPV Subtype 45
Papillomas: HPV Subtype 45 (1 of 2)
Papillomas: HPV Subtype 45 (2 of 2)

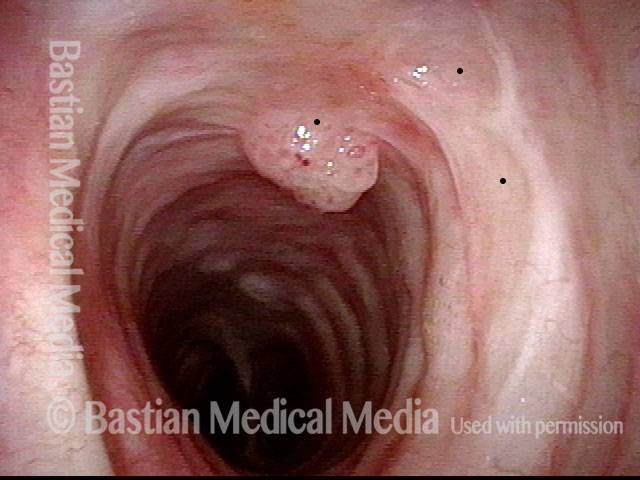
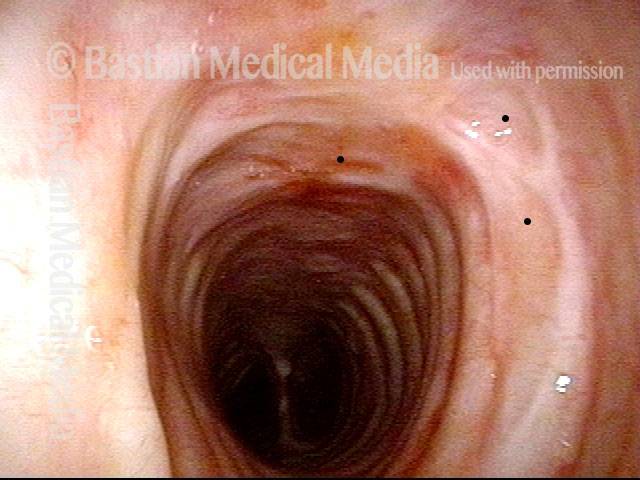
Mid-Tracheal Papilloma, Treated By Thulium Laser
Mid-tracheal papilloma, being treated by thulium laser (1 of 5)
Months after treatment: no papilloma (5 of 5)
Mid-tracheal papilloma, being treated by thulium laser (2 of 5)
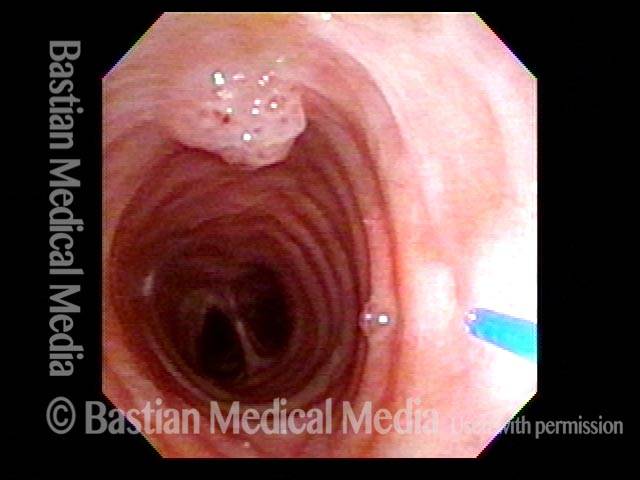
Mid-tracheal papilloma, being treated by thulium laser (3 of 5)

Mid-tracheal papilloma, being treated by thulium laser (4 of 5)

Subtle Papillomas, HPV Subtype 6
Subtle papillomas, HPV subtype 6 (1 of 3)
Subtle papillomas, HPV subtype 6 (2 of 3)

Subtle papillomas, HPV subtype 6 (3 of 3)
HPV Vascular Effect
Two papillomas (1 of 3)
Stippled vascularity (2 of 3)

HPV vascular effect (3 of 3)
Laryngeal Papillomas Rarely Can be Found by … Accident
Papilloma finding (1 of 4)
Narrow band light (2 of 4)
Closed phase (3 of 4)
Open phase (4 of 4)

Winning Papilloma Battles, but not Winning the War….Yet
Left vocal cord lesion (1 of 8)
Narrow band light (2 of 8)
One week after removal (3 of 8)
2 months after removal (4 of 8)
7 months after removal (5 of 8)
Papilloma and mucus (6 of 8)
Stippled vascularity (7 of 8)
HPV disease (8 of 8)
What “Cured” this Case of RRP? Surgery? Cidofovir? The Patient’s Immune System? All Three?
Papilloma (1 of 8)
Stippling (2 of 8)

One week after surgical removal (3 of 8)

Cidofovir injection (4 of 8)
Six months after surgical removal (5 of 8)
One week after second removal (6 of 8)
4 months later, healed (7 of 8)

3 years later, no sign of papilloma (8 of 8)
RRP Cure? Or Just Long Term Remission?
Chronic hoarseness (1 of 4)
4 months later (2 of 4)
8 months from start of treatment (3 of 4)
Narrow band lighting (4 of 4)

Polyps Need A Close Look: Here’s One Reason Why
“Polyps” diagnosis (1 of 4)

Papillomas (2 of 4)
Vascular stippling (3 of 4)
Prephonatory instant (4 of 4)

Long-term Remission or even “cure” of RRP/Laryngeal Papilloma
Chronic hoarseness (1 of 6)
Narrow band light (2 of 6)

Higher magnification (3 of 6)
Higher magnification, narrow band lighting (4 of 6)

Post-operation (5 of 6)

Post-operation, narrow band lighting (6 of 6)

Injected Local Anesthetic Causes Blanching
Infiltrating anesthetic (1 of 3)

Blanching (2 of 3)
Subglottis being injected (3 of 3)
Local Rather than Topical Anesthesia can Permit Fairly Major Tracheal Surgery
Obstructive papillomas (1 of 4)
Local injections (2 of 4)
Removal of papilloma (3 of 4)
Improved breathing with papilloma removal (4 of 4)


Curative vs Management Mode for RRP