A Fenestrated Tracheotomy Tube allows Voicing when there Is Stenosis
Tracheotomy (1 of 4)
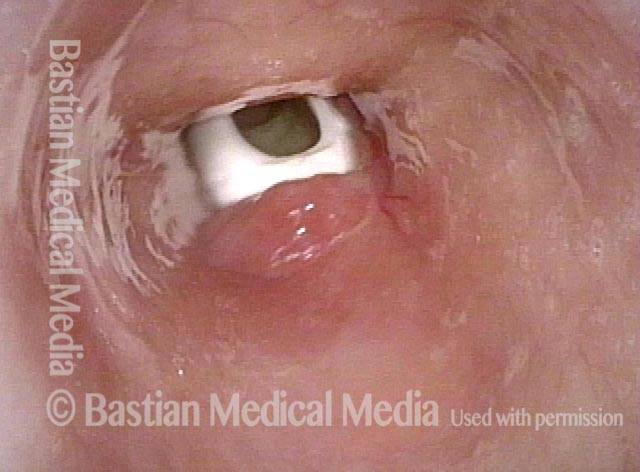
This woman was gravely ill and intubated longterm. A tracheotomy was required. Now she wants the tube removed.

View below vocal cords (2 of 4)
The tip of the scope has been taken below the vocal cords. Note the fenestrated tracheotomy tube within the high trachea.
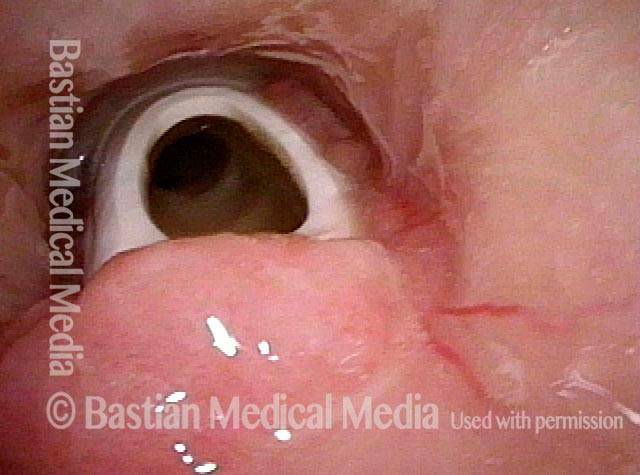
Fenestra (3 of 4)
When the patient plugs her trach tube with a finger, air comes into the distal tip of the tube (dark circle within the tube), passes up and out of the fenestra (window) and can power the vocal cords which are above our view. The trachea surrounds the tube as a whole without any “blow-by”. If there were no fenestra, the patient would be unable to speak.
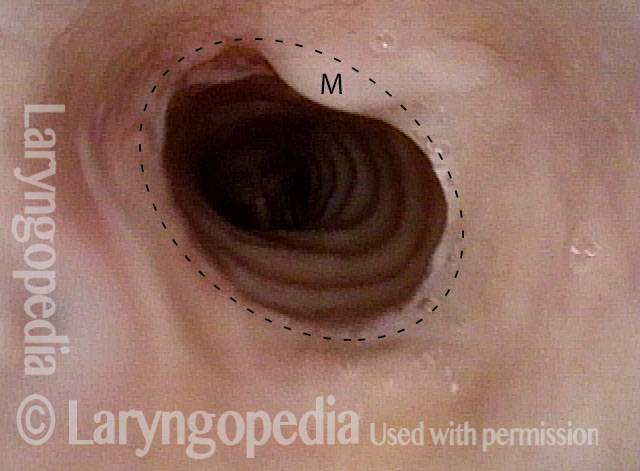
Patient post-trach (4 of 4)
After tracheal resection and re-anastomosis, the tracheotomy is no longer needed. The circular scar is at the dotted line. The M denotes overlying mucus. The patient now breathes normally.
Nuances of Endotracheal Tube Injury
This woman with high-risk comorbidities of diabetes and obesity, was in ventilated in ICU more than a month for pulmonary complications of Covid-19 infection. She had an orotracheal tube in place for 3.5 weeks, and then a tracheotomy tube was placed. Now at her first visit a year later, she remains tracheotomy-dependent, and is told she has bilateral vocal cord paralysis (disproven in the following photo series).
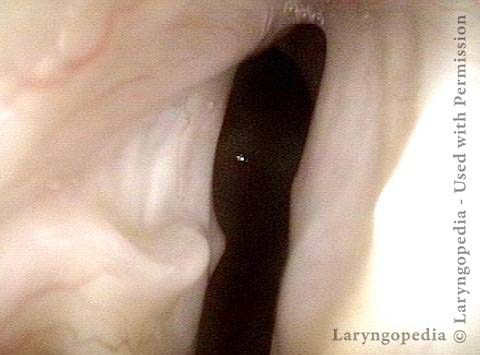
Maximum glottic opening (1 of 8)
Is it paralysis, as diagnosed elsewhere? At a fairly distant view, the maximum opening between the vocal cords at any phase of breathing appears to be approximately a 4mm glottic opening.

Undersurface mucosa indraws (2 of 8)
When the patient inspires rapidly with tracheotomy tube plugged, the vocal cord undersurface mucosa indraws (grey bands at dotted lines), further narrowing the glottic chink. One sees a faint suggestion of breathing tube injury (divot) at the arrow. Notably, there is a very low pitched rumbling sound heard that does not come from the glottis.

Phonation (3 of 8)
During phonation, the cords approximate fully, and in fact the voice is remarkably normal-sounding and she even has an excellent upper range.

Posterior commissure divot (4 of 8)
At close range while breathing with trach plugged, the posterior commissure divot subtly visible in Photo 2 is confirmed. A divot in the right posterior cord “always” indicates that the tube was taped to the left corner of the mouth. The patient’s mother confirmed that this was so.
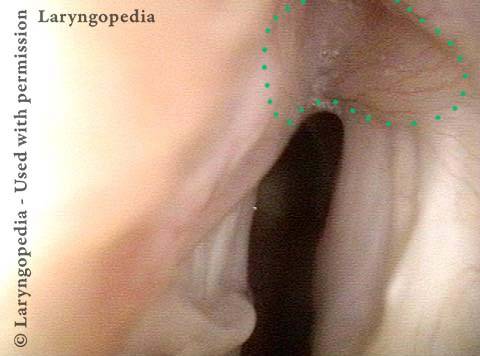
Further evidence of scarring (5 of 8)
Angling farther posteriorly, additional evidence of inter-arytenoid and possible joint capsule injury is seen. Faint dotted lines outline this area. The problem is not bilateral vocal cord paralysis but posterior commissure scarring, tethering the arytenoids together.
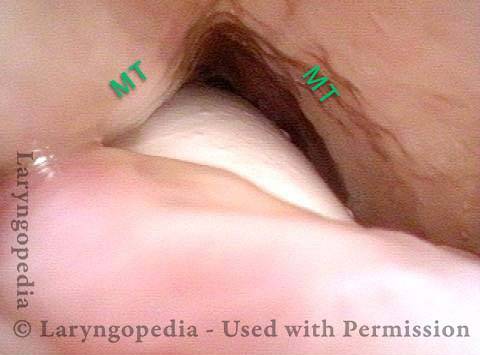
View into trachea (6 of 8)
Looking now into the subglottis and trachea, there is narrowing only at trach entry site, accentuated functionally because the membranous trachea (MT) moves in and out with respiratory phase.
Vibration of trachea (7 of 8)
When the patient plugs the trach tube and inspires rapidly, the deep rumbling sound is again heard, and comes from vibration of the membranous trachea indrawing (arrows) and vibrating (zigzag line).

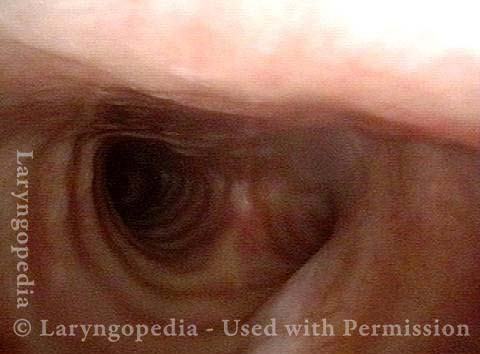
Open trachea beyond the tube (8 of 8)
A view past the tip of the trach tube shows no secondary area of tracheal stenosis.
The plan here is posterior commissuroplasty, followed by placement of a smaller trach tube and a trial of plugging. If plugging is tolerated during the day, she will need a sleep study with it plugged at night, given the tracheomalacia and her obesity.
Trachea, with Tracheotomy Tube
Trachea, with tracheotomy tube (1 of 2)
Upper trachea, with tracheotomy tube in view.

Trachea, with tracheotomy tube (2 of 2)
When the patient exhales fully, the posterior (back-side) tracheoesophageal party wall flexes anteriorly (frontward) to obstruct the trachea just above tracheotomy tube entry.
