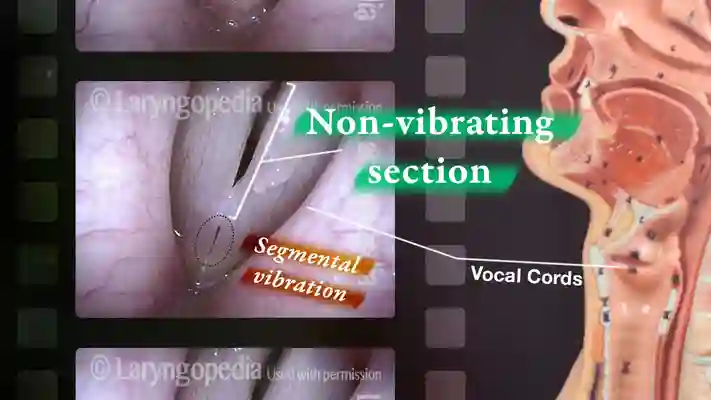
In the normal larynx, segmental vibration occurs when both chest and falsetto (head) registers are produced by vibration of the anterior 2/3 of the vocal cords. The posterior 1/3 is “inhabited” by the arytenoid cartilage and does not vibrate.
In certain pathological circumstances such as displayed in the photo sequences below, only a small part of the vocal cords vibrates.
Causes and Symptoms
This segmental vibratory phenomenon is typically seen in vocal cords that are damaged—such as by vocal nodules, polyps, cyst, scarring, etc. In such persons, upper voice is typically particularly impaired, until, as the person continues to try to ascend the scale, suddenly a crystal-clear “tin whistle” kind of voice emerges and may continue upwards to very high pitches.
Some in the past have talked about flagelot, flute, bell, or whistle register. We suspect that this was in the days before videostroboscopy and at least in some cases may have been segmental vibration.
The best way to determine if what sounds like a “tin whistle” upper voice extension is due to segmental vibration is by videostroboscopic examination during that kind of phonation. The other way is for the individual to produce their “tin whistle” kind of voice very softly and then try to crescendo.
If full length vibration, smooth crescendo will be possible. If segmental, there will be a sudden “squawk” as the vocal cords try to go (unsuccessfully) from segmental to full-length vibration.
Segmental Vibration Compared to Full-length
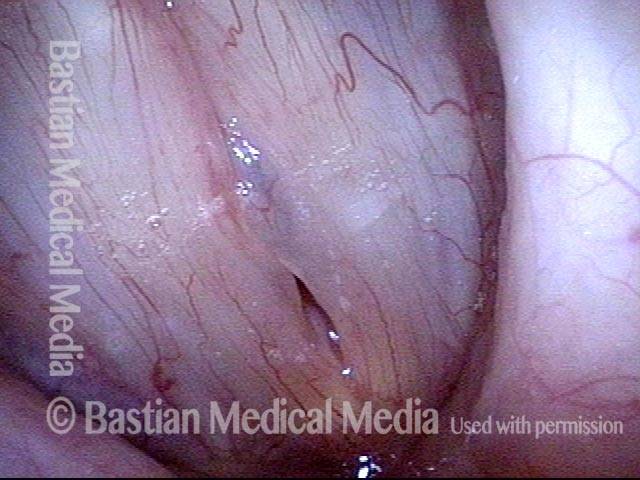
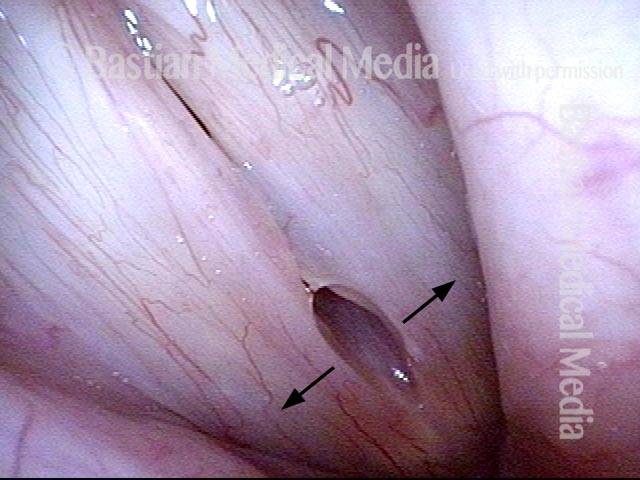
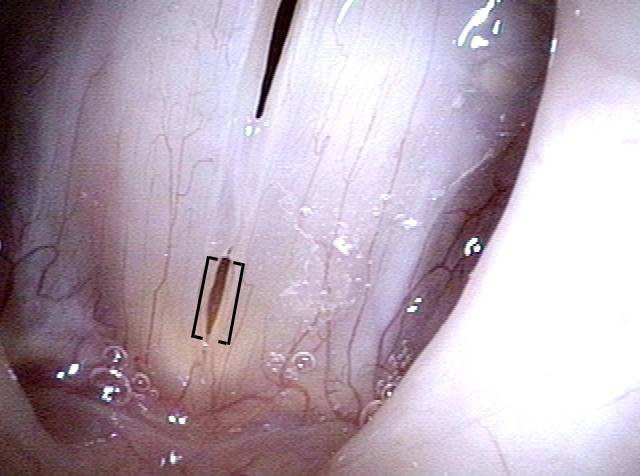
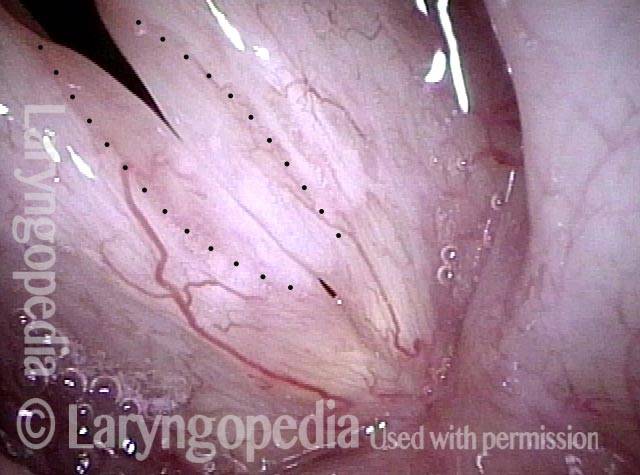
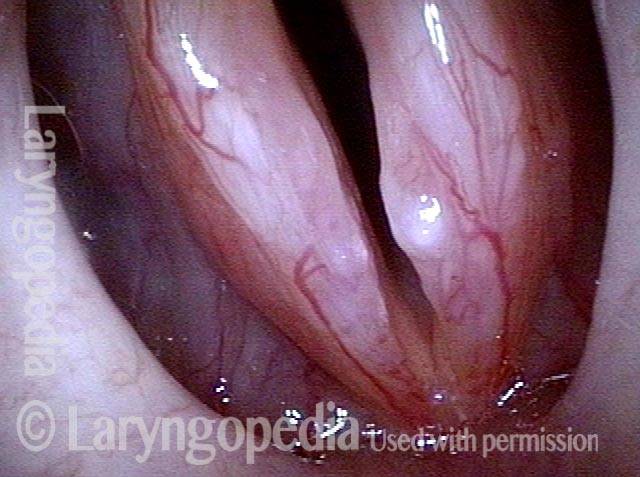
Translucent polypoid swellings (1 of 4)
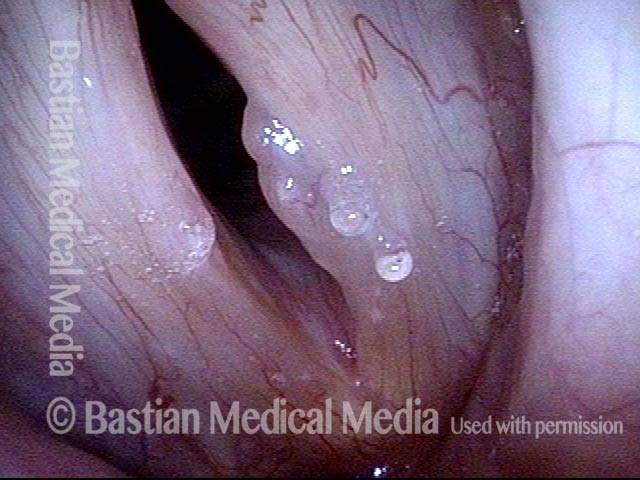
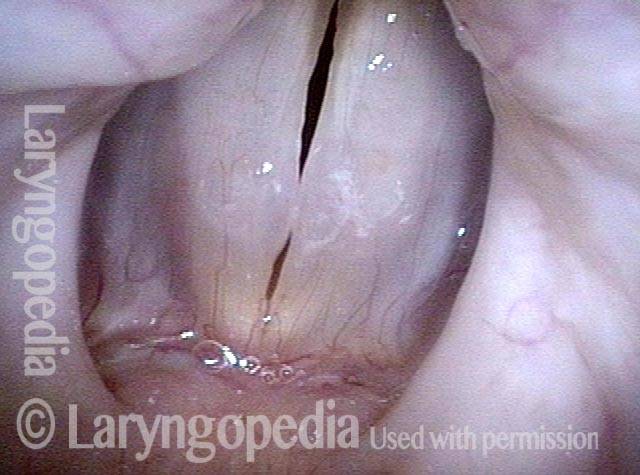
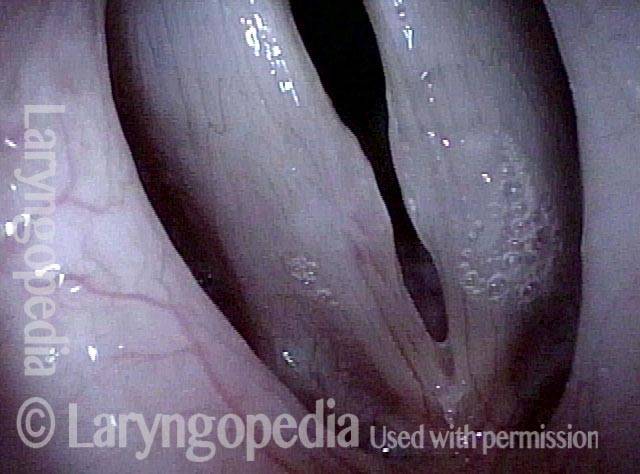
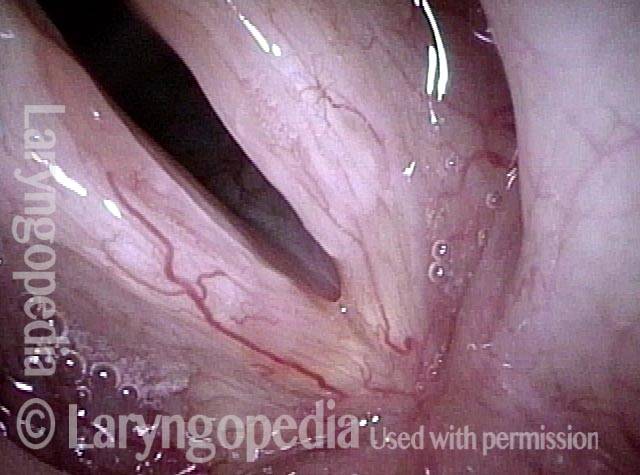
Open phase, E3 (2 of 4)
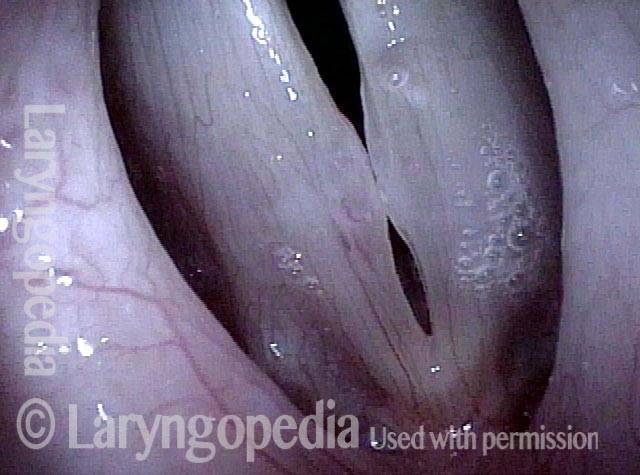
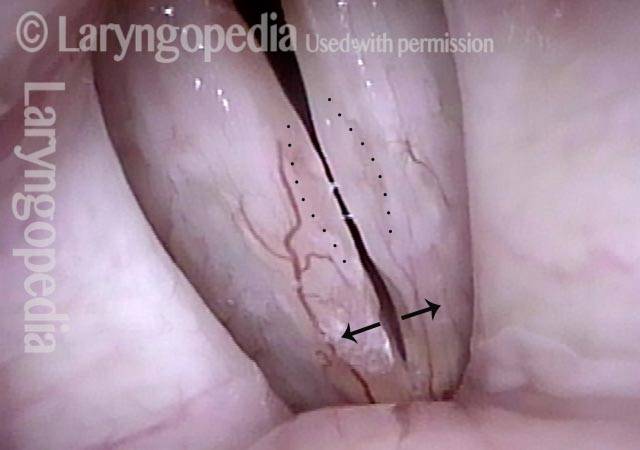
Closed phase, E4 (3 of 4)
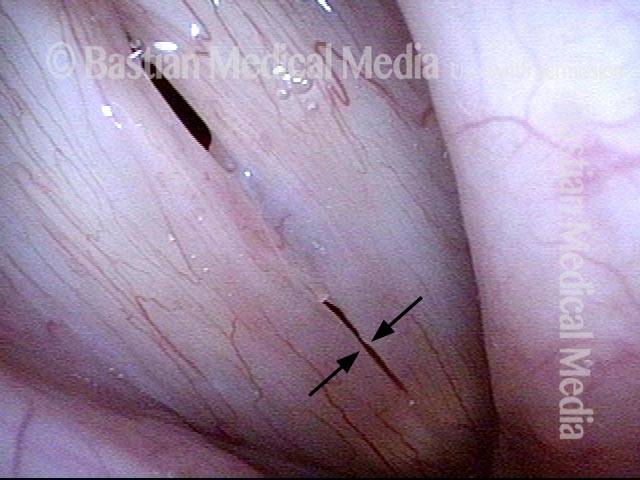
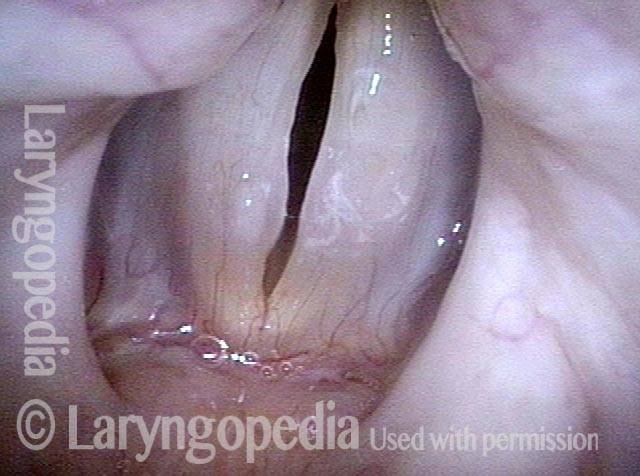
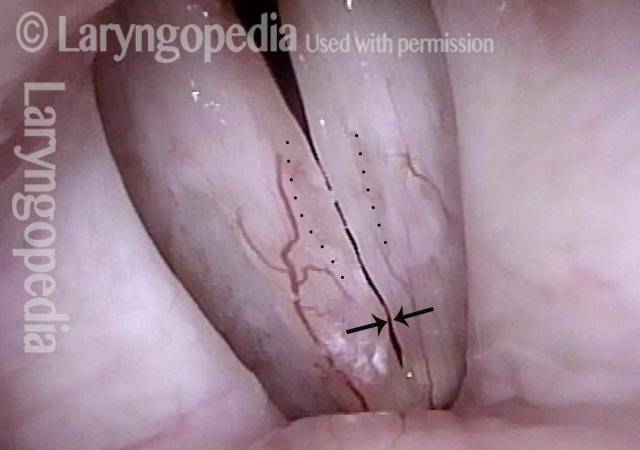
Open phase, E4 (4 of 4)
Whistle Register or Tin-whistle Segmental Vibration?
Closed phase (1 of 4)
Open phase (2 of 4)
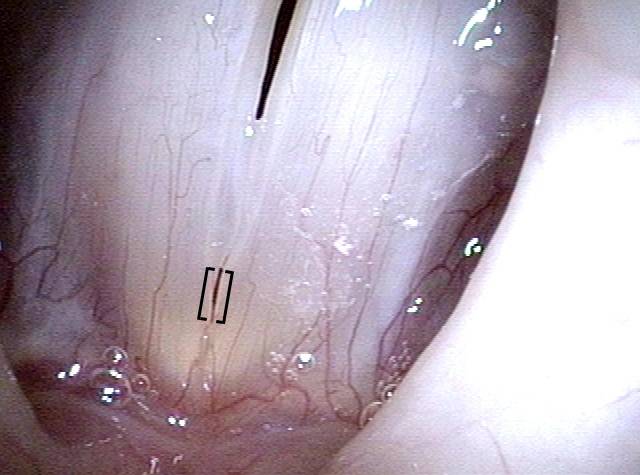
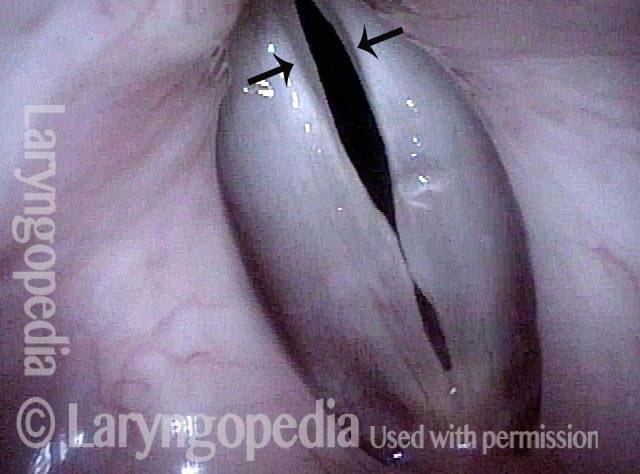
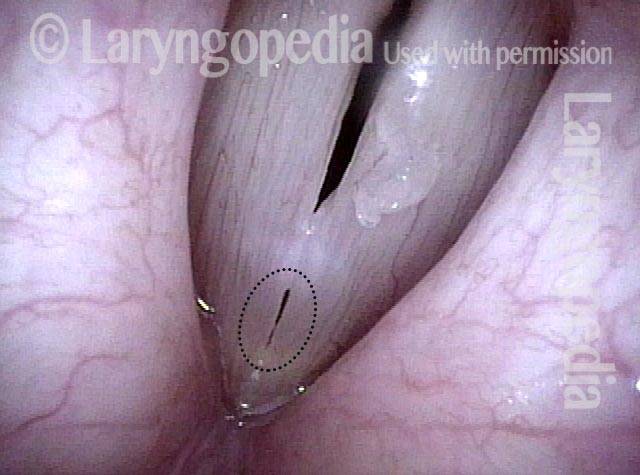
Segmental vibration (3 of 4)
Whistle register (4 of 4)
Search not Only for Nodules, but Also for Segmental Vibration and Look at the Posterior Commissure for MTD
Open phase (1 of 4)
Closed phase (2 of 4)
Segmental vibration (3 of 4)

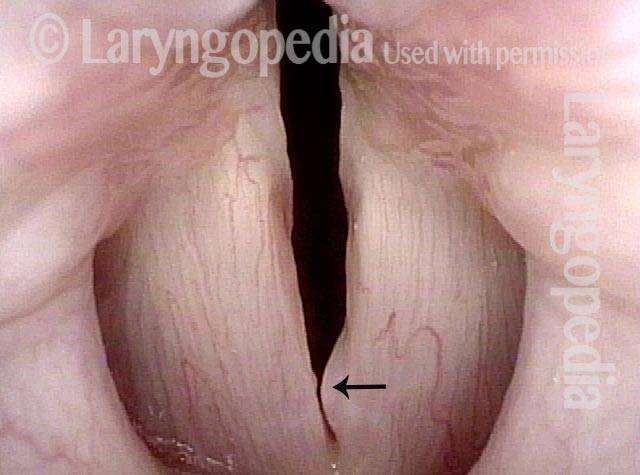
Posterior commissure (4 of 4)
Sulcus and Segmental Vibration
Glottic sulci (1 of 4)
Open phase (2 of 4)
Closed phase (3 of 4)
Segmental vibration (4 of 4)
Open Cyst and Sulcus; Normal and Segmental Vibration
Margin swelling (1 of 6)

Narrow band light (2 of 6)

Open phase, strobe light (3 of 6)
Closed phase, same pitch (4 of 6)

Segmental vibration (5 of 6)

Closed phase (6 of 6)

Tiny Vibrating Segment Gives Tiny Tin Whistle Voice
Prephonatory instant (1 of 6)
Phonation (2 of 6)

Gaps due to nodules (3 of 6)

Open phase (4 of 6)

“Tin whistle” sound (5 of 6)
“Tin whistle” at open vibration (6 of 6)