Contact Granuloma
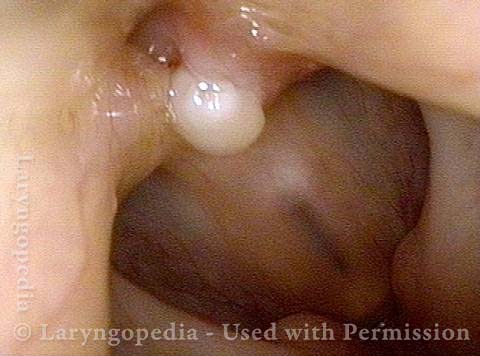
A contact granuloma is a benign tissue reaction or growth, typically on the posterior third of the vocal cord, that occurs in response to injury. They are also known as contact ulcers, intubation granulomas, or “proud flesh.” This kind of chronically irritated tissue may be viewed as an exuberant healing response that “didn’t know when to quit.”
Sources of Injury
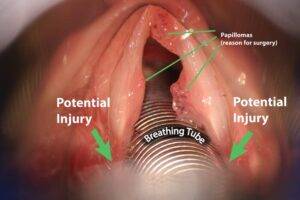
One type of injury that may lead to a contact granuloma is injury from an endotracheal tube, as the inserted tube presses and rubs against the posterior ends of the vocal cords.
Another potential source of injury is chronic, aggressive coughing or throat-clearing. Yet another potential source is undergoing surgical procedures such as laser excision of a cancer. Some also believe that irritation from acid reflux can lead to a contact granuloma. In many cases, there is no obvious cause for the original injury.
Typical Location
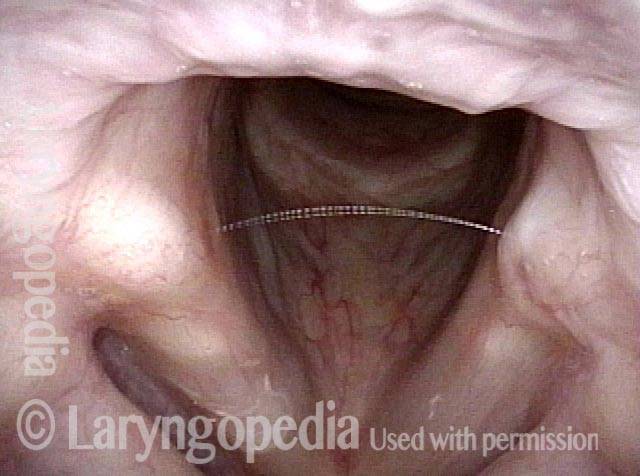
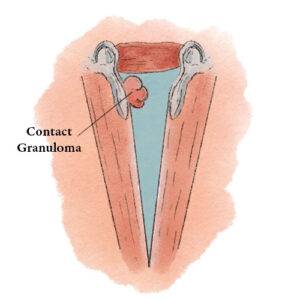 Contact granulomas typically occur on the posterior third of the vocal cord, also known as the cartilaginous glottis. Unlike the other two-thirds of the vocal cord, this segment is inhabited by cartilage (namely, the arytenoid cartilage), and that cartilage is covered only by a relatively thin layer of perichondrium and a layer of mucosa. This thinly cushioned cartilage or perichondrium interface is particularly prone to being irritated and then responding with the exaggerated healing that produces a contact granuloma. Hence, most granulomas occur in this location.
Contact granulomas typically occur on the posterior third of the vocal cord, also known as the cartilaginous glottis. Unlike the other two-thirds of the vocal cord, this segment is inhabited by cartilage (namely, the arytenoid cartilage), and that cartilage is covered only by a relatively thin layer of perichondrium and a layer of mucosa. This thinly cushioned cartilage or perichondrium interface is particularly prone to being irritated and then responding with the exaggerated healing that produces a contact granuloma. Hence, most granulomas occur in this location.
Symptoms
Some individuals with contact granulomas have no symptoms whatsoever and only discover they have a granuloma while being examined for some other reason. Others notice a sticking or pinprick sensation, or have some sense of vague discomfort in the area of the neck radiating upward towards the angle of the jaw.
Occasionally, a person may develop a “catch” in the voice, such that it takes a second to begin speaking clearly. Very occasionally, when a bit of the granuloma detaches (see below), a person may cough up blood or a tiny piece of tissue. In general, symptoms are mild.
Treatment
Some clinicians prefer to treat contact granulomas by removing them. However, the tiny injury or wound that results often produces a recurrent granuloma.
A better approach is simply to wait for the granuloma to detach of its own accord. This process of self-detachment, which may take several months, is like an apple maturing and then dropping from the tree: the granuloma continues to grow in size, and once it becomes big enough, the back-and-forth movement of air and the displacement caused by contact with the opposite arytenoid cartilage cause the granuloma to slowly pinch inward at its base and become more and more pedunculated. Eventually, the connecting stalk can no longer support the granuloma, and the granuloma breaks free. For an example, see the photos below.
If, however, a person’s symptoms are too troublesome to wait for months, then the granuloma can be surgically removed, but while still leaving part of the stalk or base projecting from the surface, so as to avoid re-injuring the cartilage and perichondrium, which would provoke the formation of another granuloma.

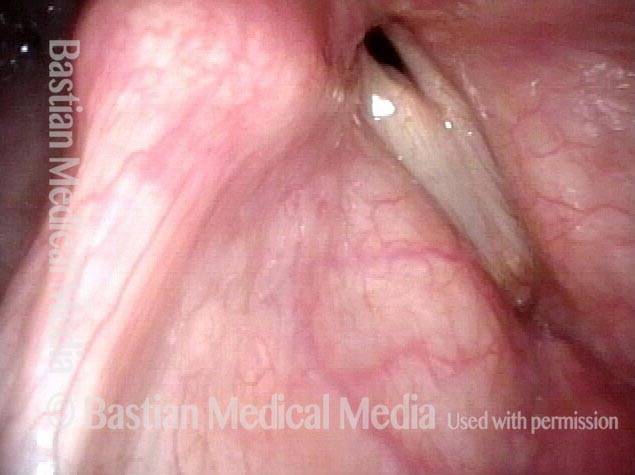
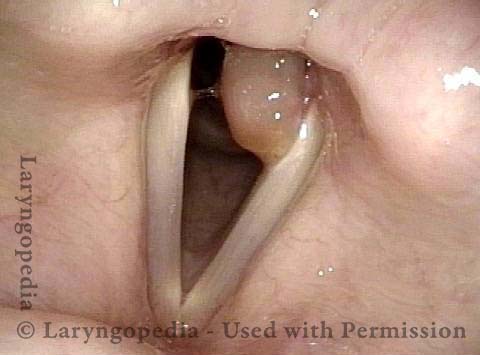
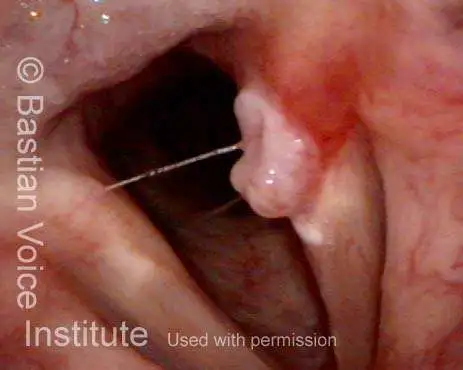
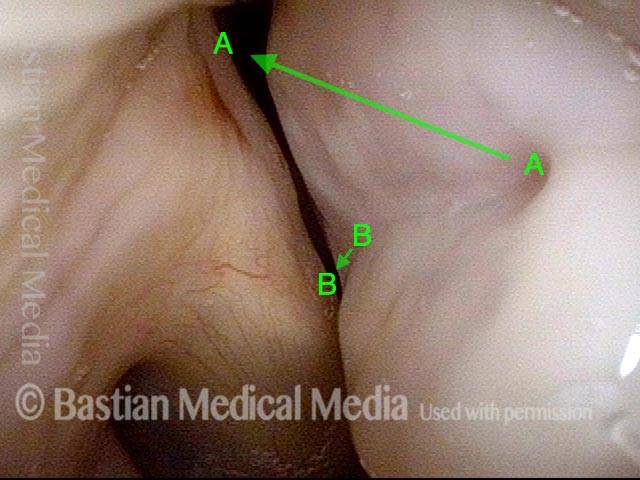
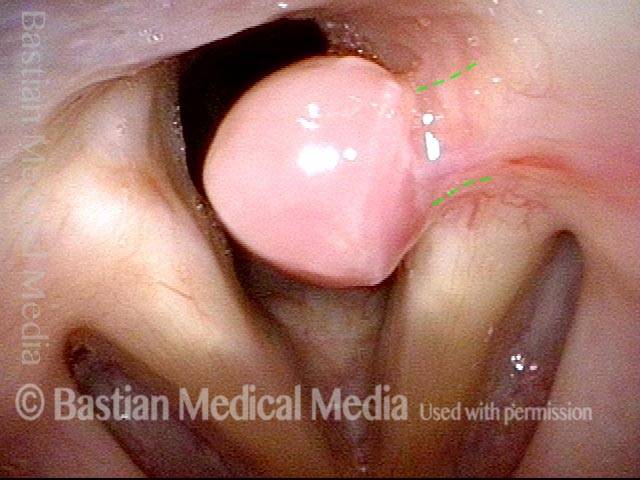
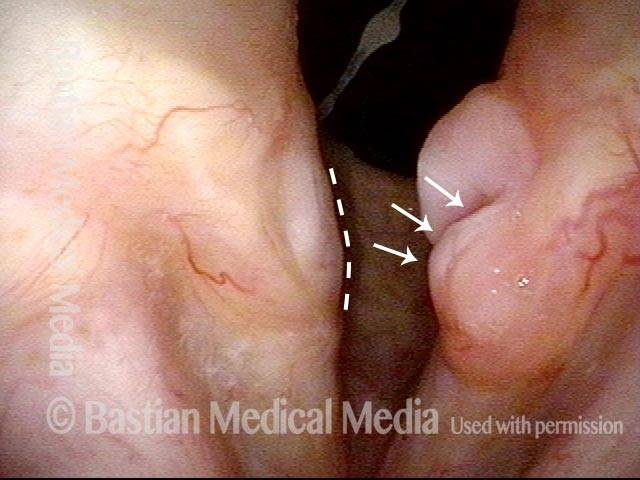
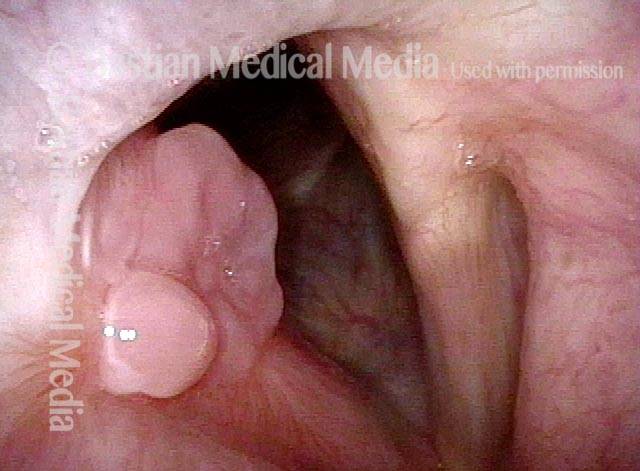
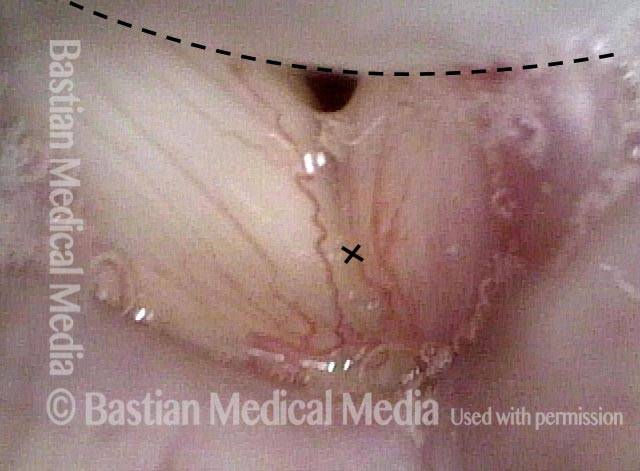
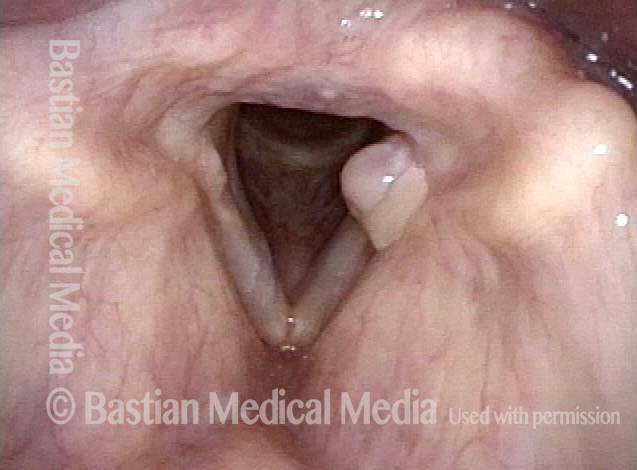
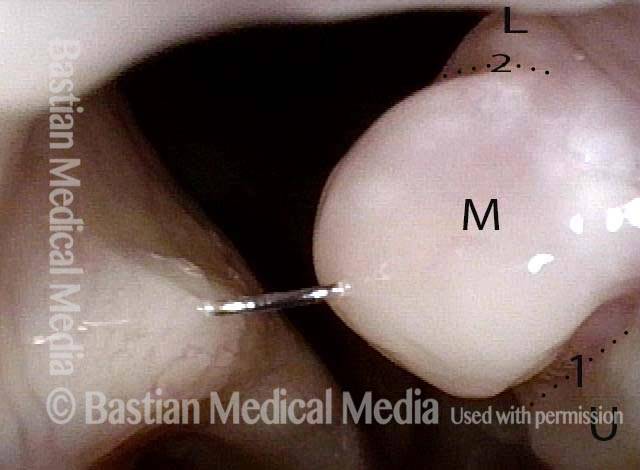
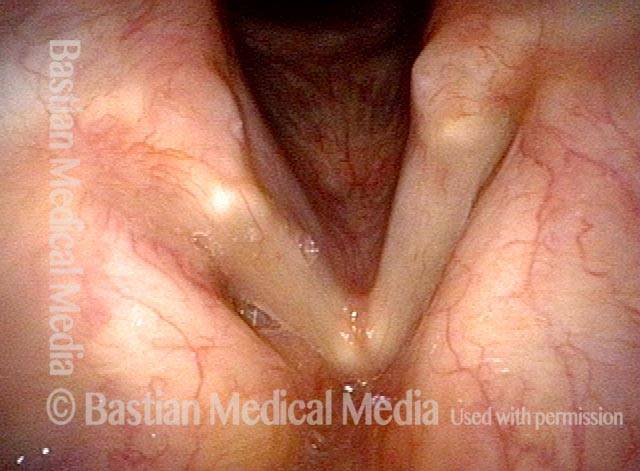
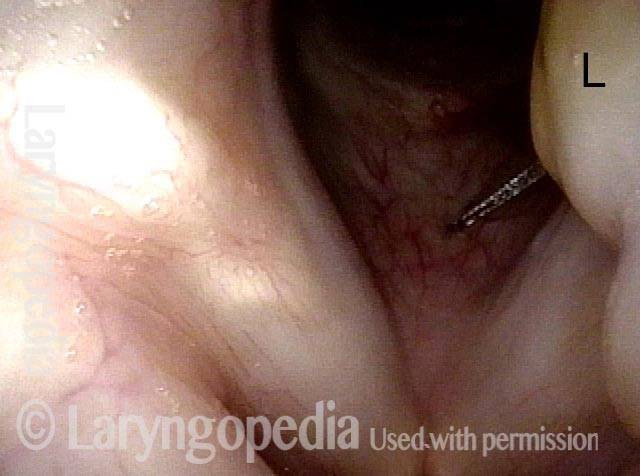
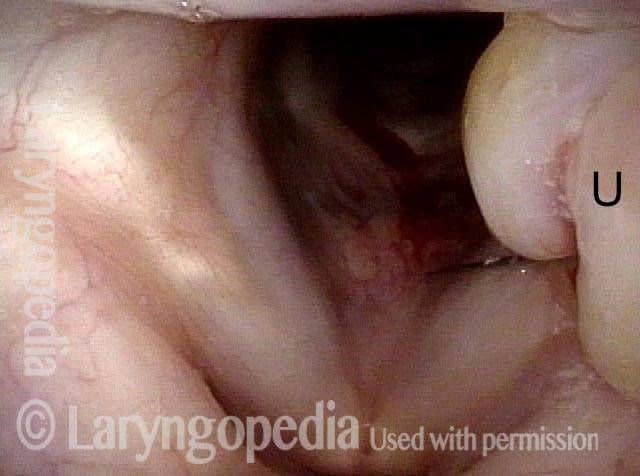
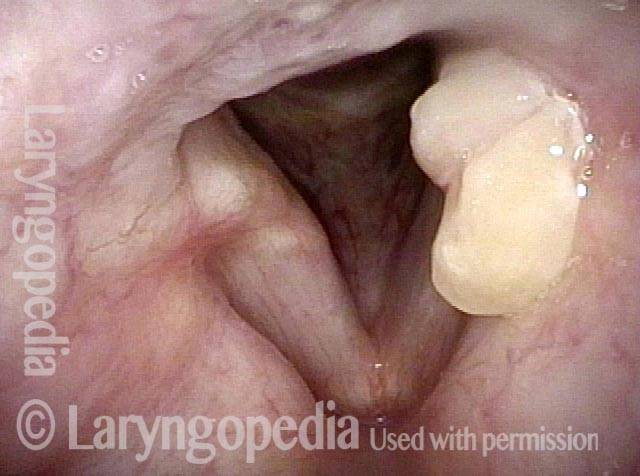
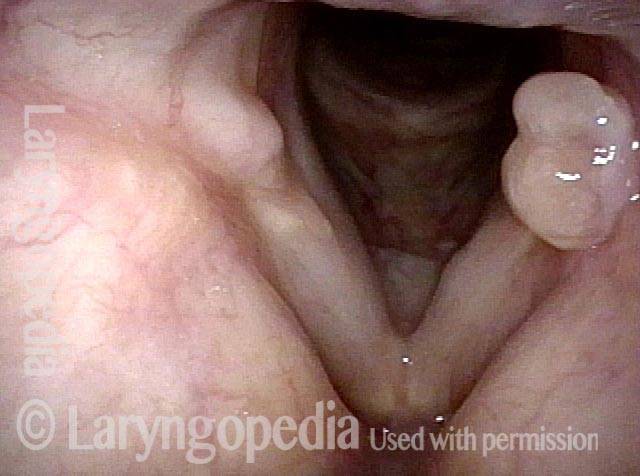
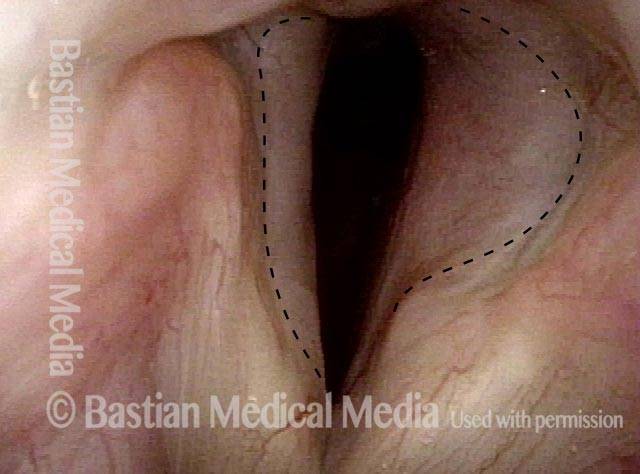
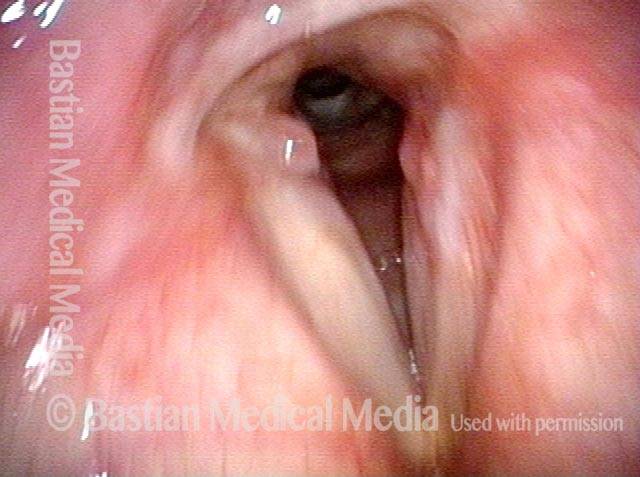
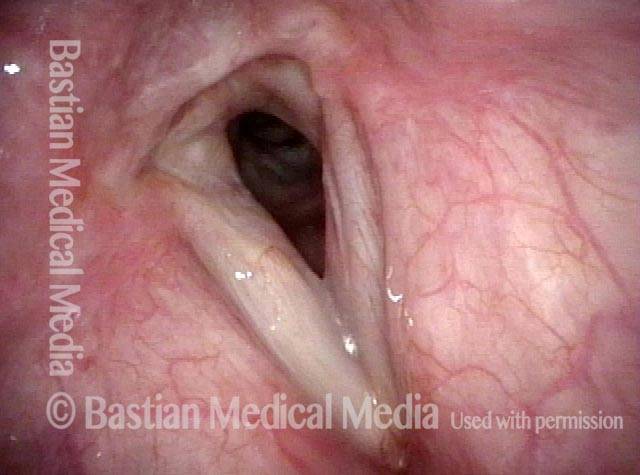
“Tongue and groove” Fit of a Bi-lobed Contact Granuloma
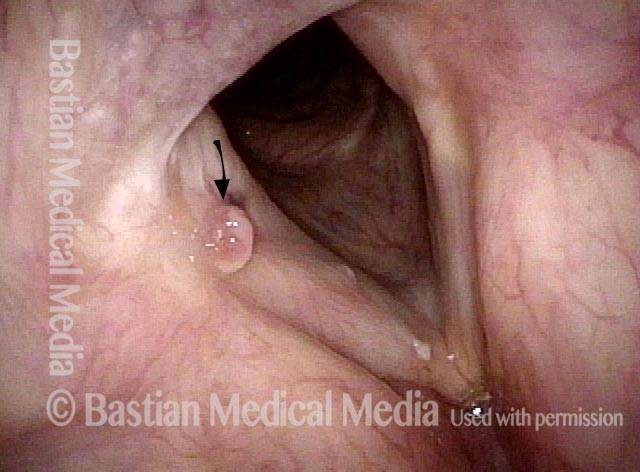
This man experiences momentary sharp pain when he first talks after an interval of silence. He has had a biopsy elsewhere but the lesion (a contact granuloma) has returned, as would be expected, due to re-injury of the arytenoid perichondrium.
As explained elsewhere, contact granulomas can be diagnosed by “certain” visual criteria, and be allowed to mature and detach spontaneously, with no need for removal except in unusual circumstances.
Tongue and groove (1 of 4)

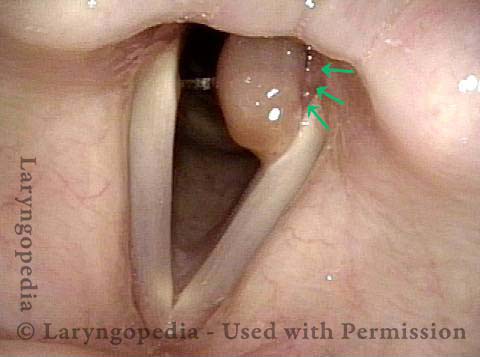
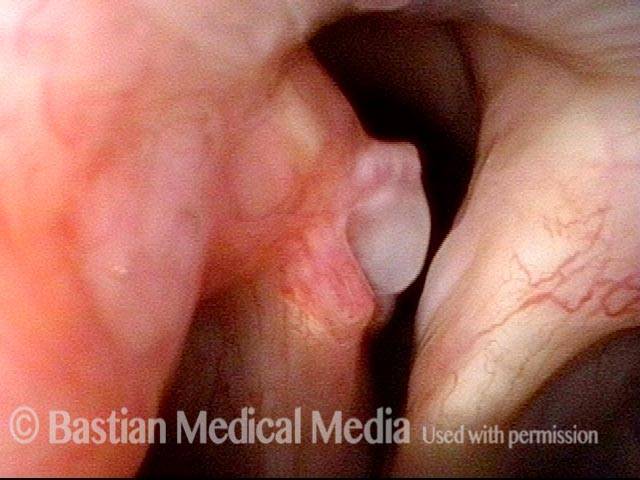
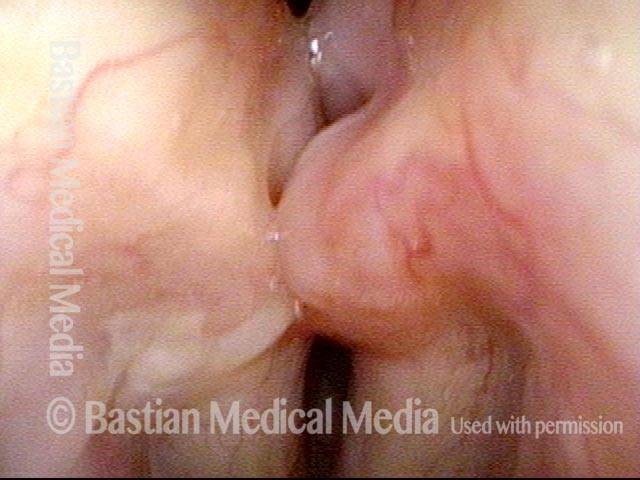
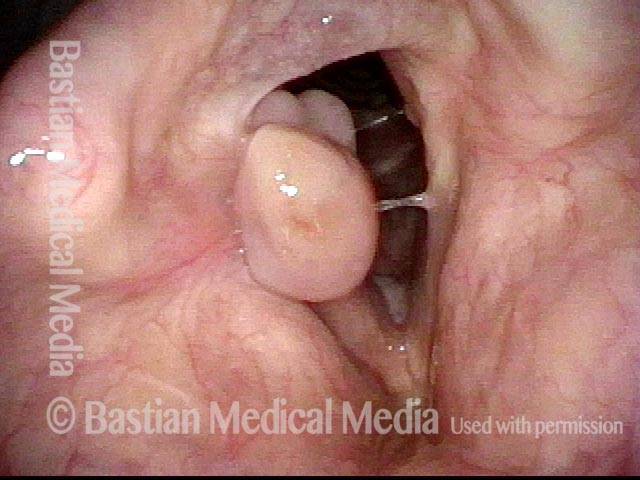
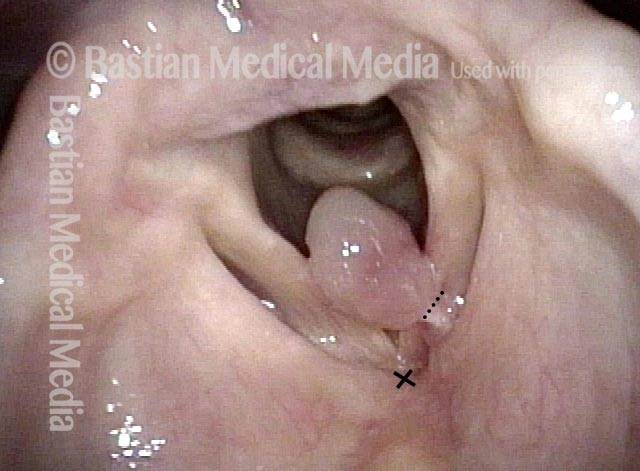
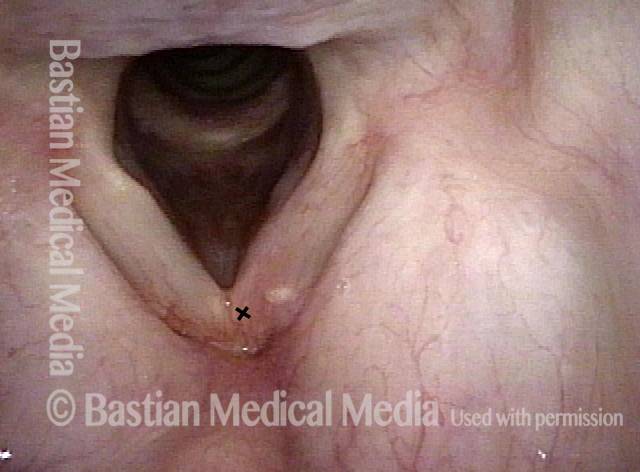
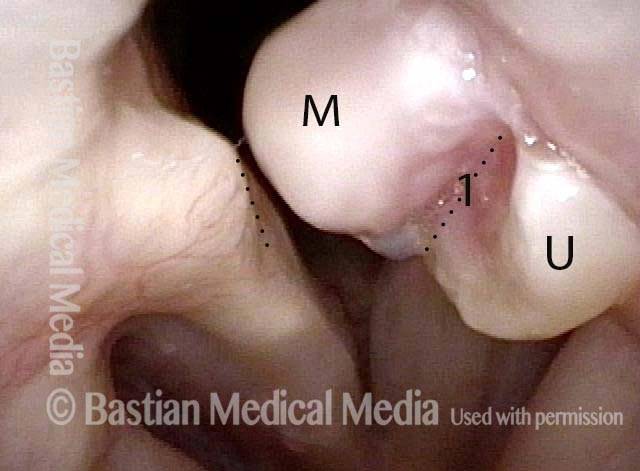
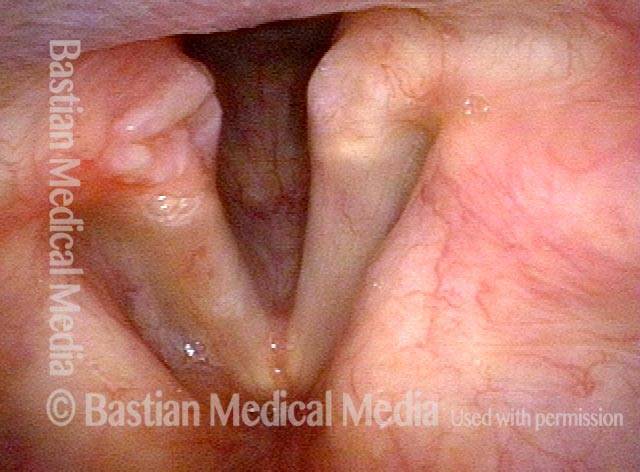
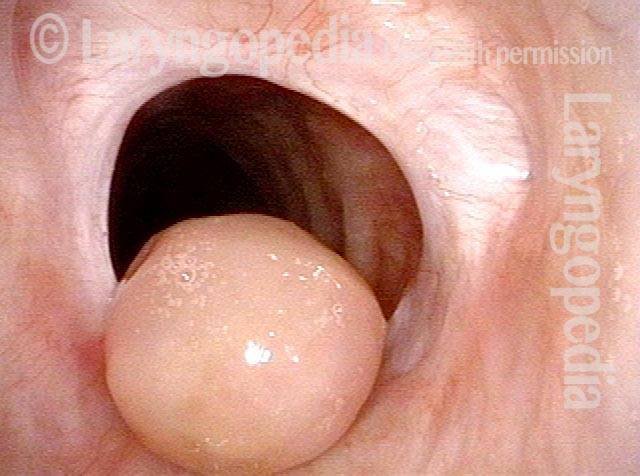
Bi-lobed lesion (2 of 4)

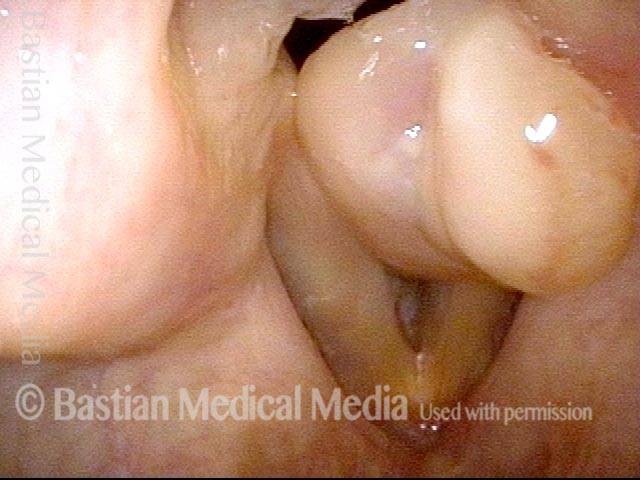
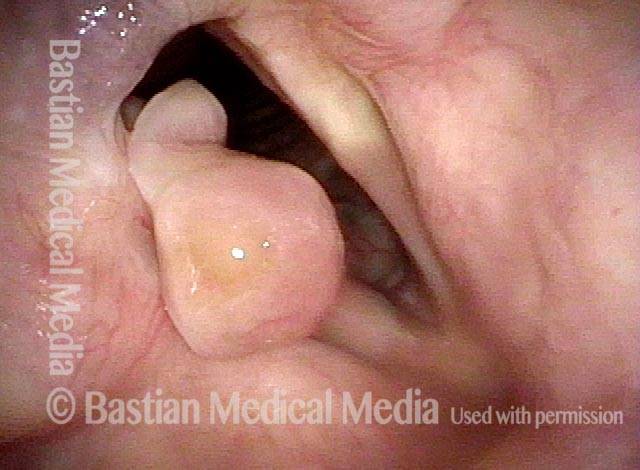
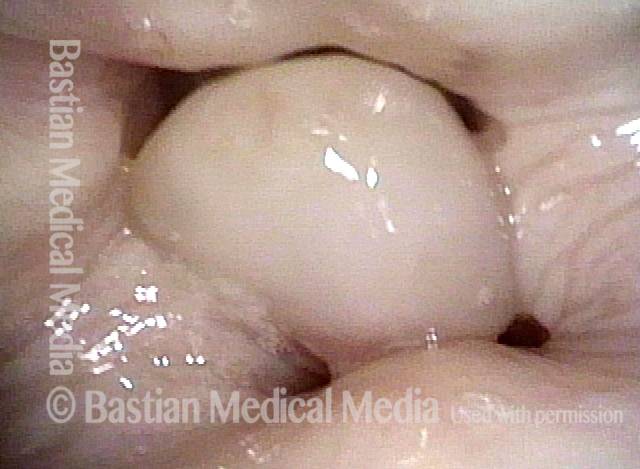
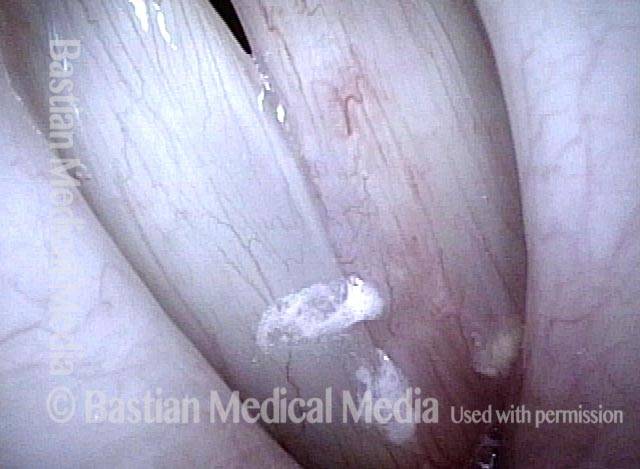
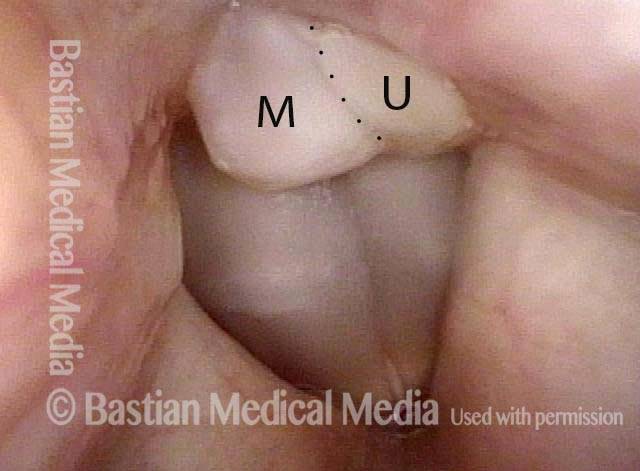
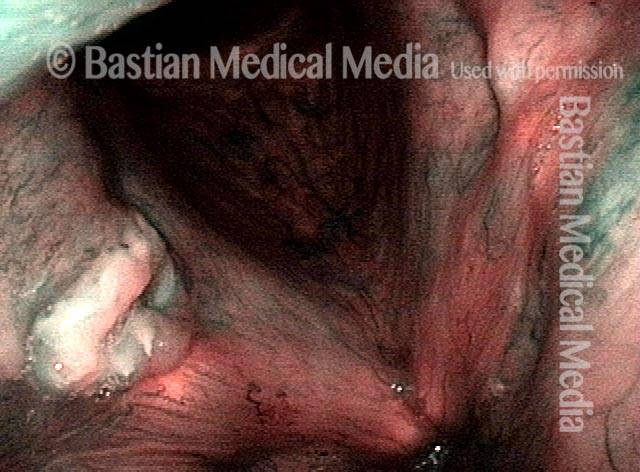
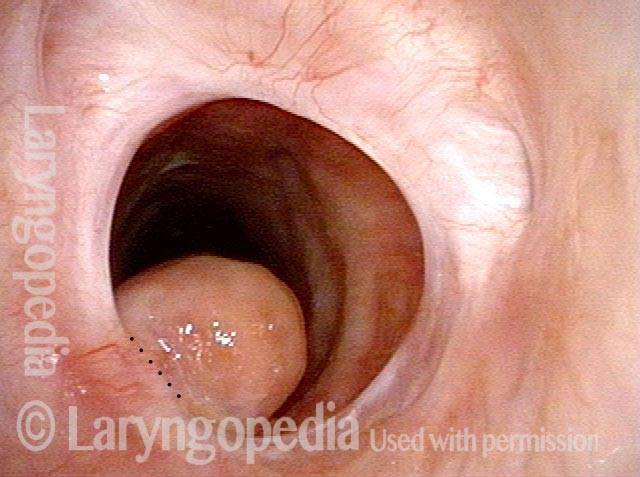
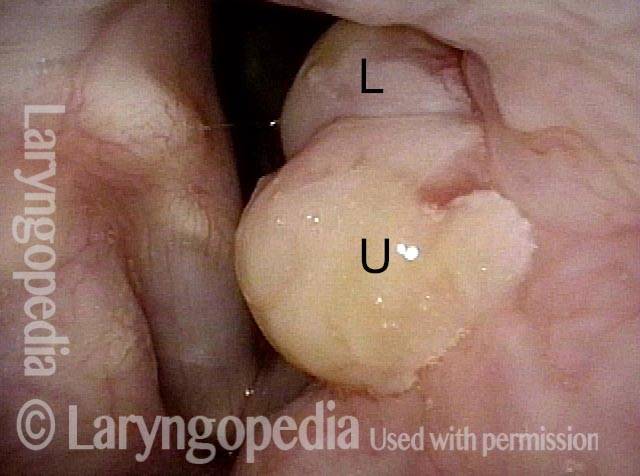
Bi-lobed morphology of granuloma (3 of 4)

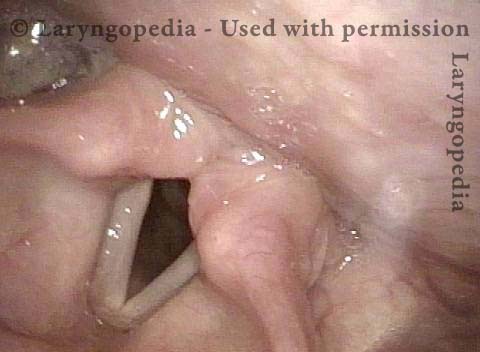
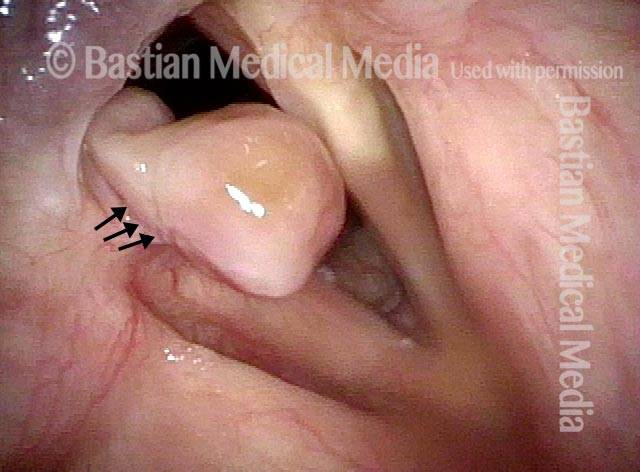
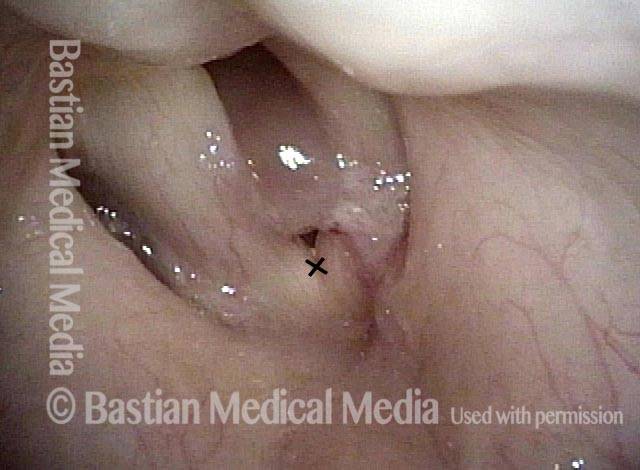
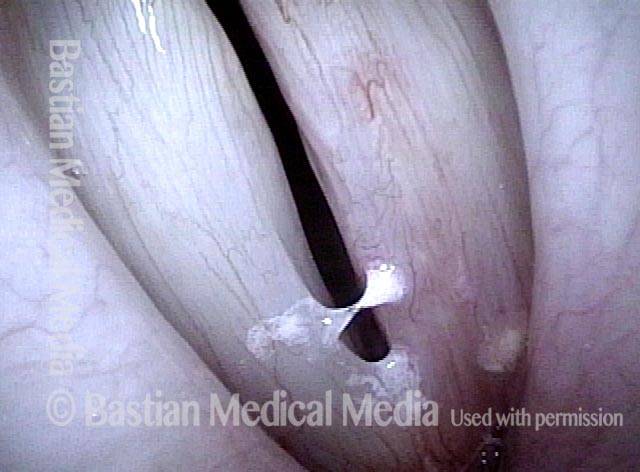
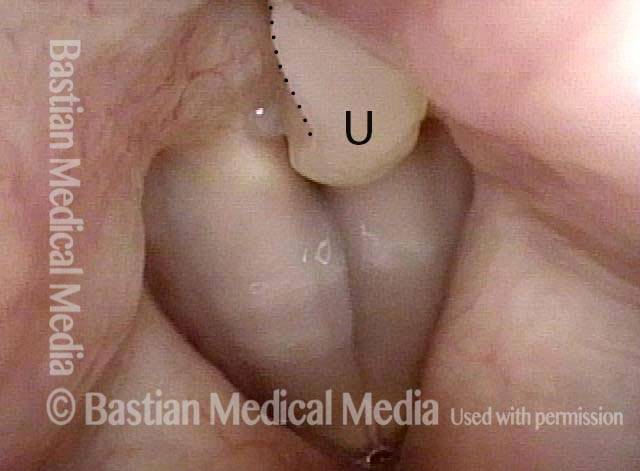
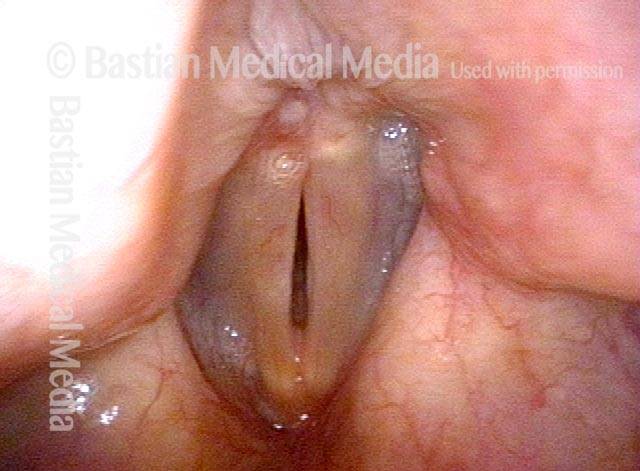
Tongue and groove fit between cords (4 of 4)
“Tattoo” of Blood after Detachment of Intubation Granuloma
Intubation granuloma (1 of 5)
Pedunculation in process (2 of 5)
Granuloma is gone (3 of 5)
Blood tattoo (4 of 5)
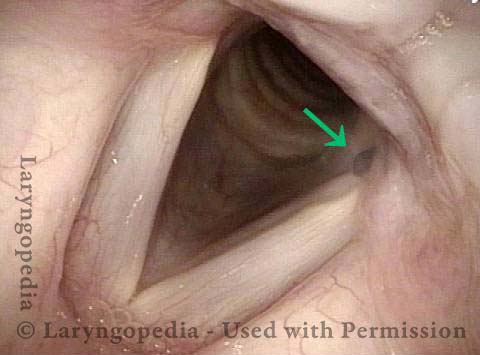
Blood Tattoo (5 of 5)
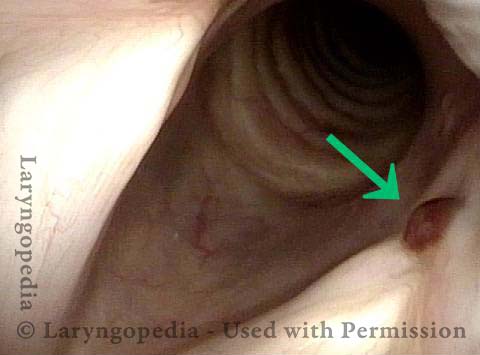
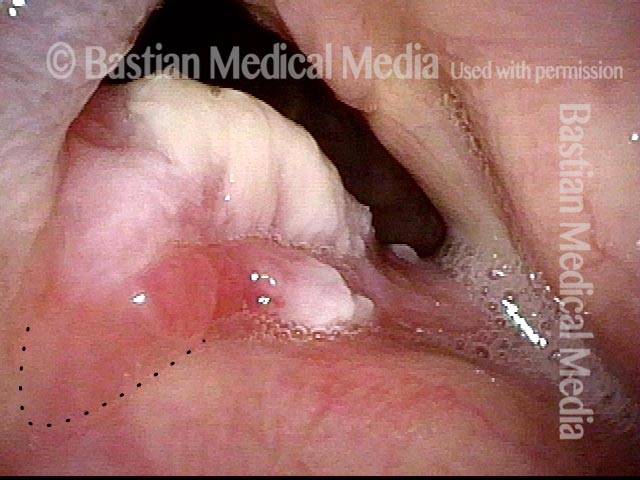
Photo Essay of Contact Granuloma
Residual haziness (1 of 2)
Bi-lobed granuloma (2 of 2)

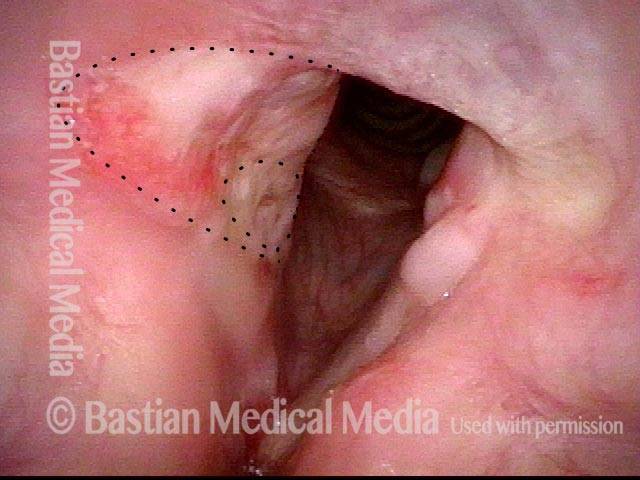
Example 2
Bi-lobular Granuloma (1 of 2)

Arytenoid cartilage fits into cleft (2 of 2)
Intubation Granulomas Can Be Left Alone to Mature and Spontaneously Detach
Intubation Granuloma (1 of 3)

Pedunculated Granuloma (2 of 3)

Pedunculation in process (3 of 3)
{kind=link}
Contact Granuloma, Gradually Pedunculating and then Detaching
Bi-lobed granuloma (1 of 11)

Granuloma displaces upwards (2 of 11)
Vocal process fits in granuloma cleft (3 of 11)
Granuloma doesn’t affect voice (4 of 11)

2 months later (5 of 11)
Granuloma slowly penduculates (6 of 11)

2 months later (7 of 11)

Granuloma detached (8 of 11)
5 months later (9 of 11)

One year later (10 of 11)

One year later (11 of 11)

Contact Granuloma, “Key-in-lock Fit”
Bi-lobed granuloma (1 of 3)
Key-in-lock granuloma (2 of 3)
Cleft and bi-lobularity (3 of 3)
The Healing Sequence of Granulation
Large tumor, before removal (1 of 8)
After tumor removal (2 of 8)
2 months after surgery (3 of 8)
5 Months after surgery, a granuloma is seen (4 of 8)
7 months after surgery (5 of 8)
Pedunculation (6 of 8)
One year after surgery (7 of 8)
15 months after surgery (8 of 8)

Vocal Cord “Tear” and Granuloma
Intubation injury (1 of 8)
Granuloma drawn into glottis (2 of 8)
Phonation (3 of 8)
Anterior commissure (4 of 8)
Granuloma detached (5 of 8)
Vocal cord blurring (6 of 8)

Closed phase (7 of 8)
Open phase (8 of 8)
TRI-Lobed Contact Granuloma
Panoramic view (1 of 6)
Upper and middle lobule, cleft 1 (2 of 6)
Phonation (3 of 6)
Lower lobule (4 of 6)

Upper and middle lobule, Cleft 2 (5 of 6)
Tri-lobed (6 of 6)
Contact Granuloma—Ulcer Type With Rolled Border
Persistent granuloma (1 of 4)
Narrow band light (2 of 4)
Phonation (3 of 4)
One year later (4 of 4)
Evolution of Circular Tracheal Scar Including Granuloma
Two weeks post-op (1 of 4)

Six weeks post-op (2 of 4)
Inhaling (3 of 4)
Rapid inhalation (4 of 4)

Granulomas Mature and Fall Off by Themselves, But Steroid Injection Can Help…
“Third” granuloma (1 of 6)
Injection into lower lobe (2 of 6)
Injection into upper lobe (3 of 6)
Five weeks later (4 of 6)
Six months post-injection (5 of 6)
One year post-injection (6 of 6)
Sometimes you DO Remove Granulation to Avoid Tracheotomy
Granulation (1 of 8)

Closer view (2 of 8)

Post microlaryngoscopies (3 of 8)

Scarring (4 of 8)
Post posterior commissuroplasty (5 of 8)
Breathing improved (6 of 8)
Closer view (7 of 8)

Phonatory view (8 of 8)