PCA-only paresis is weakness or paralysis of the vocal cord’s posterior cricoarytenoid (PCA) muscle, but with normal function of the vocal cord’s other muscles. The PCA muscle abducts (lateralizes) the vocal cord for breathing. The following are indicators of PCA-only paresis:
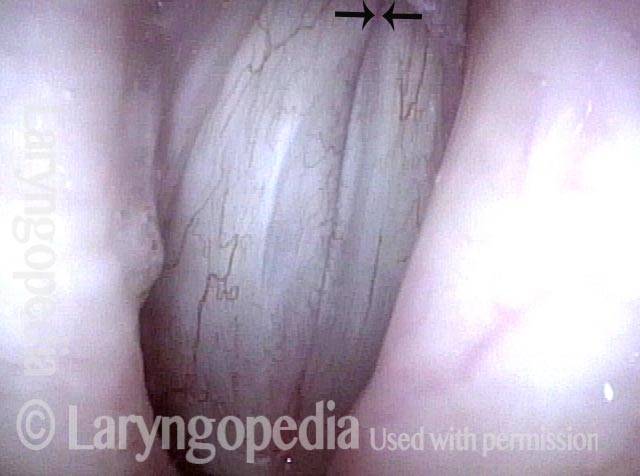
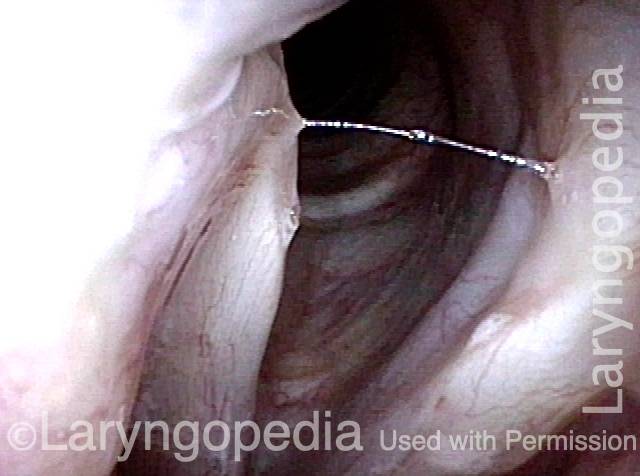
- Movement: The vocal cord closes normally for voicing, but it does not abduct for breathing. It remains motionless at the midline.
- Position and appearance: Position is normal during phonation, but the vocal cord does not open (lateralize) for breathing. Because the cord does not appear to move (it adducts or closes normally, but from an already-adducted position), PCA-only paresis is often mistaken for complete vocal cord paralysis—TA (thyroarytenoid), LCA (lateral cricoarytenoid), and PCA. Key points of difference between PCA-only paresis and complete paralysis are that, in the former case, the tip of the vocal process is in a normal medial position and the vocal cord has normal bulk and tone.
- Appearance during voicing (under strobe lighting): Completely normal, because the adductors of the cord (TA and LCA muscles) are intact. Hence, as with a normal cord, there is no flaccidity or asymmetry of vibration.
- Voice quality: Entirely normal. Many individuals are told this is due to “compensation” of the opposite cord, but actually it is because the muscles used for voicing (TA + LCA) are intact.
Other variants of vocal cord paresis include LCA-only, TA-only, TA + LCA, and IA-only (interarytenoid muscle).
Paresis, PCA-only
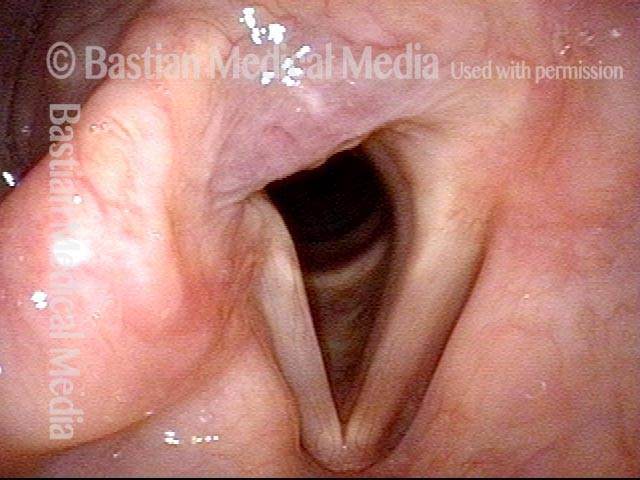
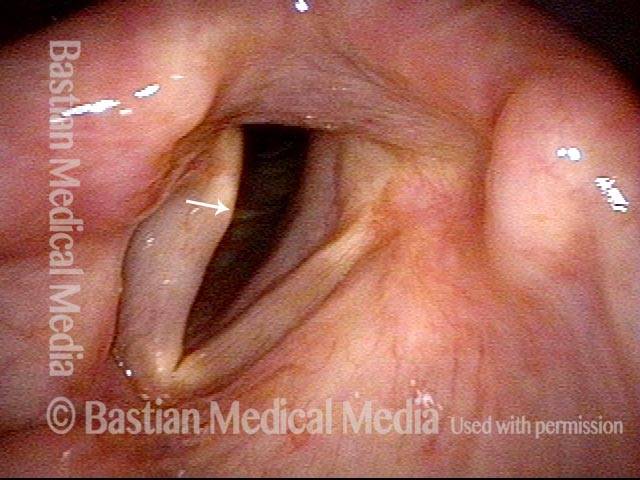
Paresis, PCA-only (1 of 4)
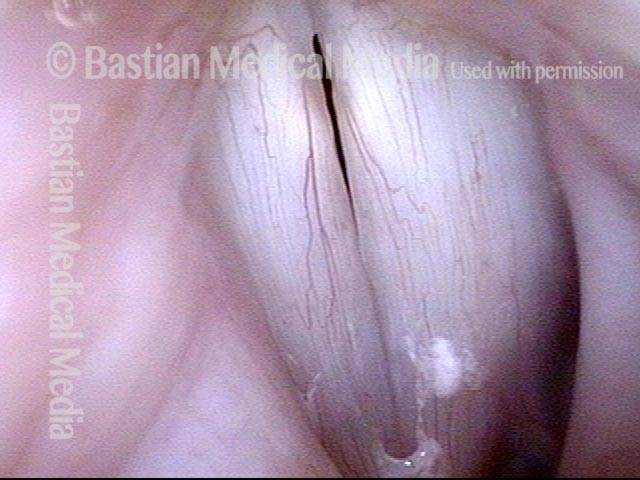
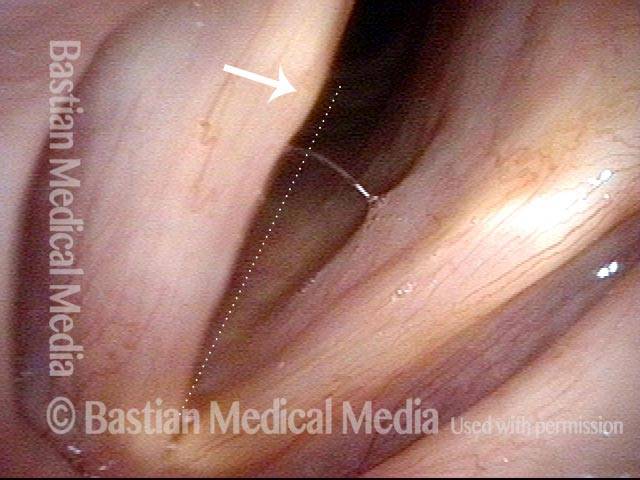
Paresis, PCA-only (2 of 4)

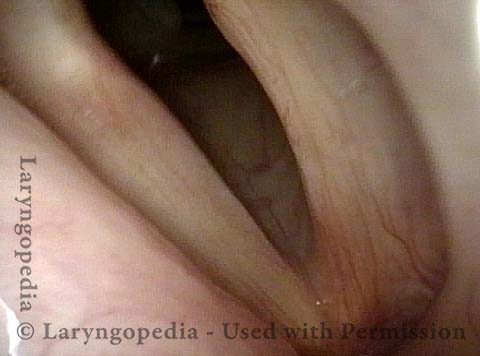
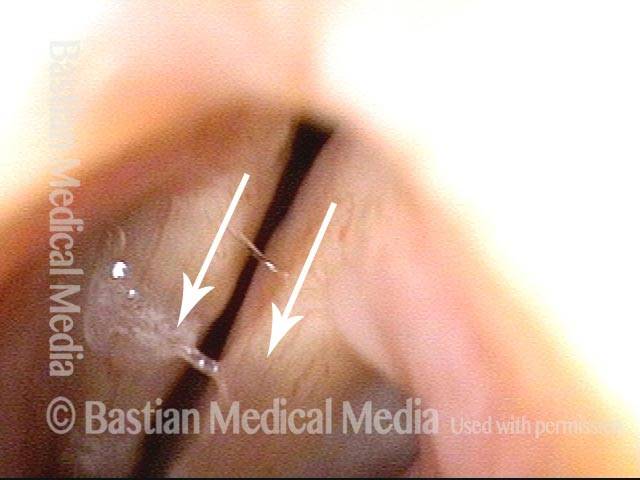
Paresis, PCA-only (3 of 4)
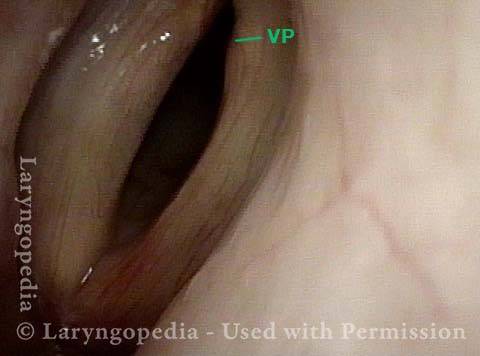
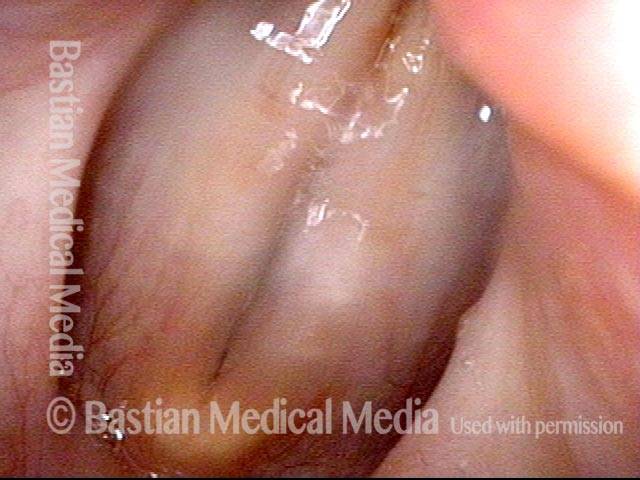
Paresis, PCA-only (4 of 4)

Evolution of Vocal Cord Paralysis To End as PCA-only Paresis
For some voice doctors, measurement is accorded more respect than observation. Both are legitimate, of course, yet, visual (observational) understanding of paralysis and paresis remains far more useful than EMG, acoustic, or aerodynamic measurements. This case strongly illustrates that point.
This older man underwent thoracic surgery but due to complications was also intubated for much of two days. Immediately upon awakening, his voice was altered. He said it was whisper only.
At his original office visit a month later, he thought his voice had improved to “10%” and examination showed left vocal cord paralysis (TA, LCA, and PCA muscles all non-functional). Three months later, his voice was by his description to 40% and improving further week by week. By month 8 post-surgery, verified at 18 months, he felt his voice was “99%” recovered; examination showed recovery of TA and LCA, but not PCA muscle.
The final diagnosis: Left PCA-only paresis. Rather than being entirely “out,” the PCA seems only to be weak.
Left Cord Margin Bowing (TA weakness) (1 of 11)
LCA Paresis Identified (2 of 11)
Voice is Breathy! (3 of 11)

LCA Paresis Best View (4 of 11)
4 Months Later, Glottis Open For Breathing (5 of 11)

Gap during phonation less (6 of 11)

PCA Weakness Is All That remains (7 of 11)
LCA Recovered: The Vocal Process Now Turns Medially (8 of 11)
At 18M, Left Cord Does Not Abduct Due To Continuing PCA Weakness (9 of 11)

Left PCA Can Muster Some Lateralization (10 of 11)
Full Recovery for Voicing, Despite PCA-Only Paresis (11 of 11)

PCA-only Paresis Years after Thyroid Lobectomy
PCA-only paresis years after thyroid lobectomy (1 of 6)
PCA-only paresis years after thyroid lobectomy (2 of 6)
PCA-only paresis years after thyroid lobectomy (3 of 6)
PCA-only paresis years after thyroid lobectomy (4 of 6)
PCA-only paresis years after thyroid lobectomy (5 of 6)

PCA-only paresis years after thyroid lobectomy (6 of 6)
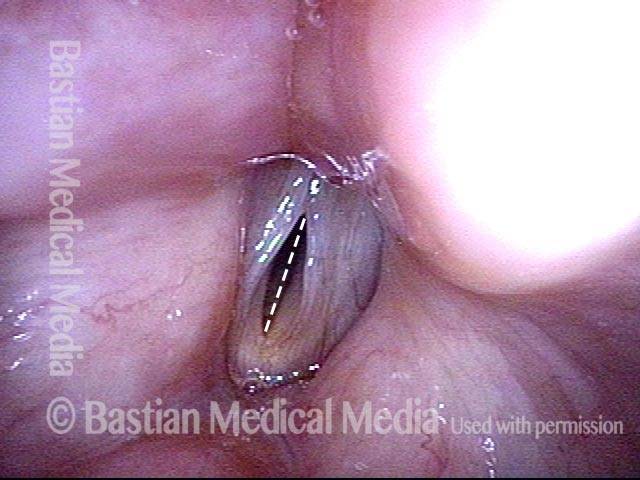
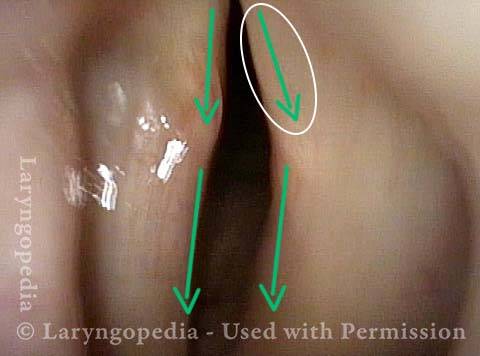
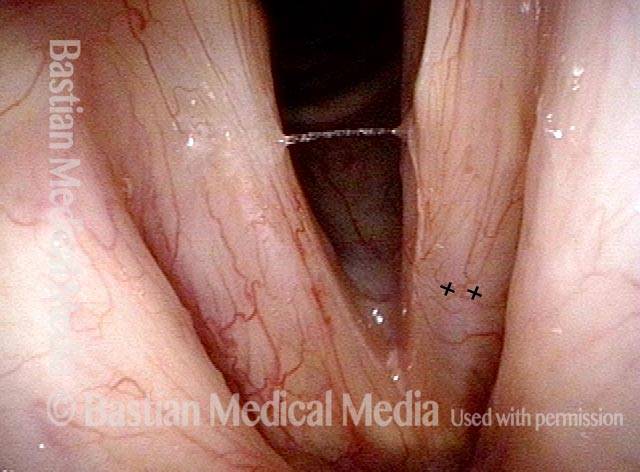
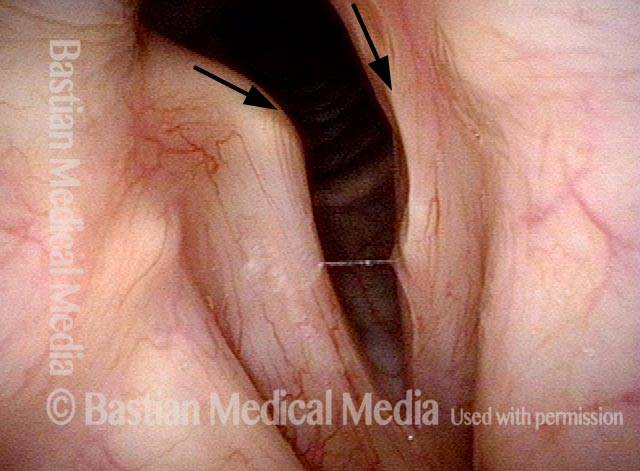
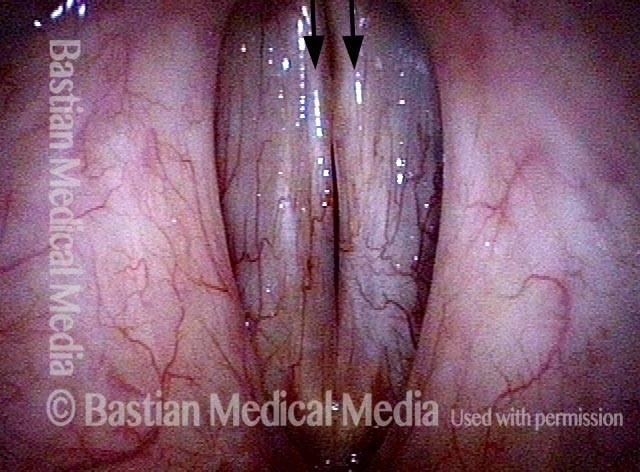
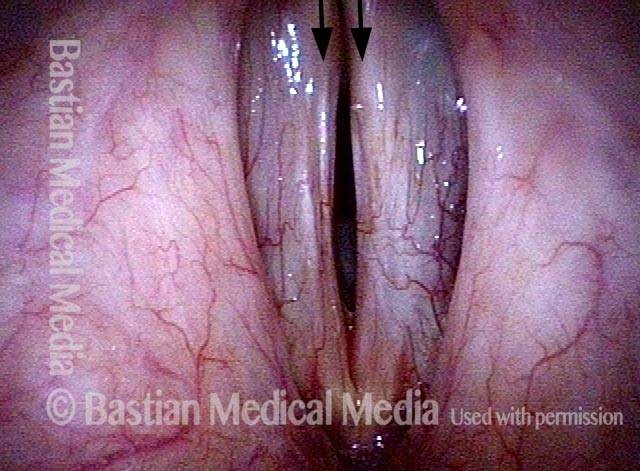
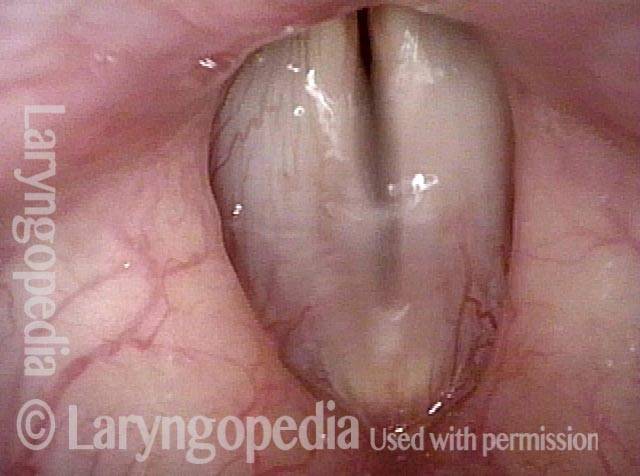
Left PCA-only Paresis
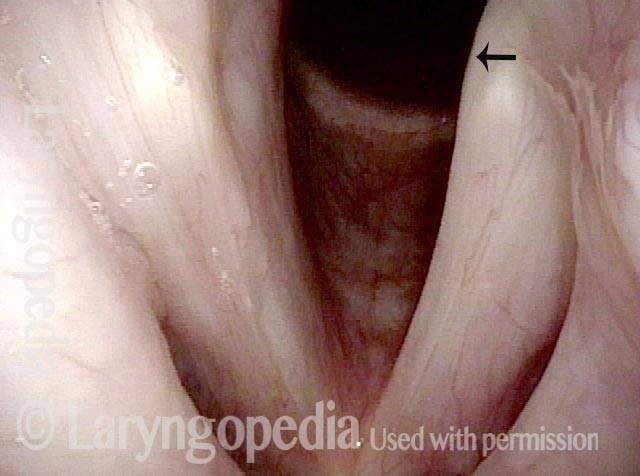
Abducted breathing position (1 of 4)
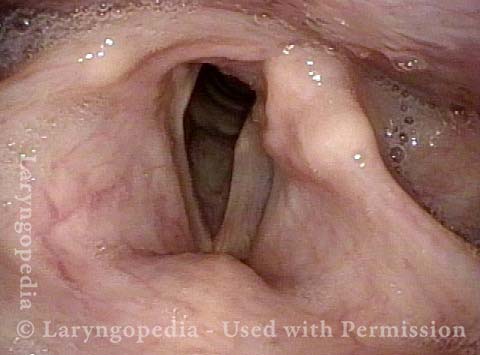
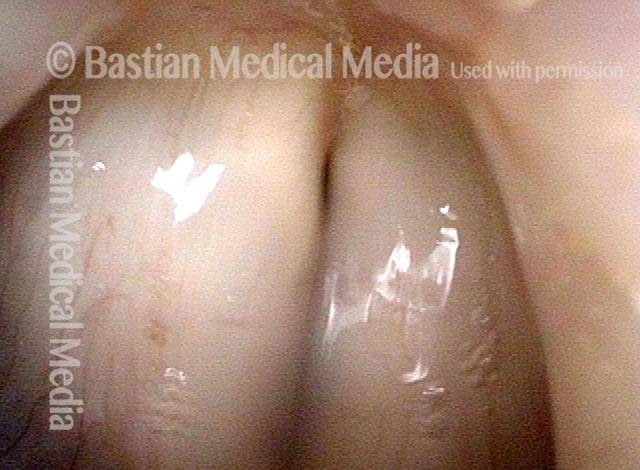
Full approximation of cords, TA is intact (2 of 4)

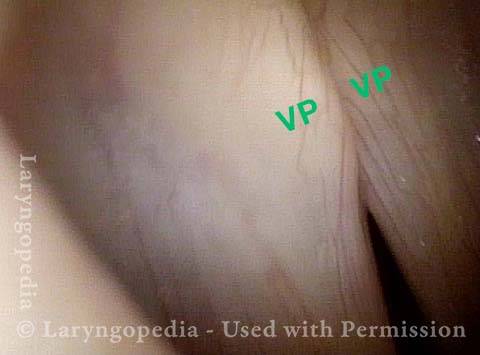
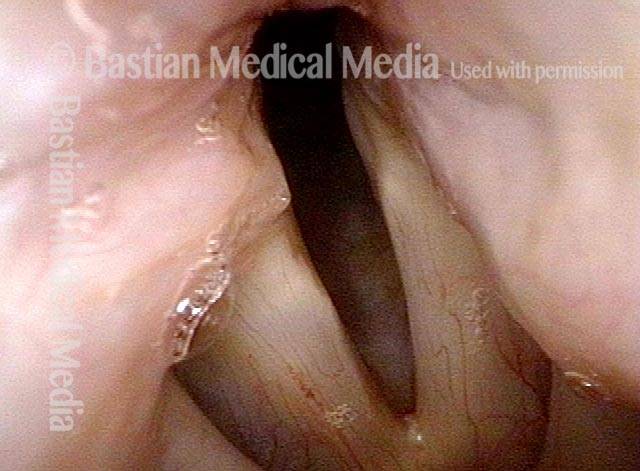
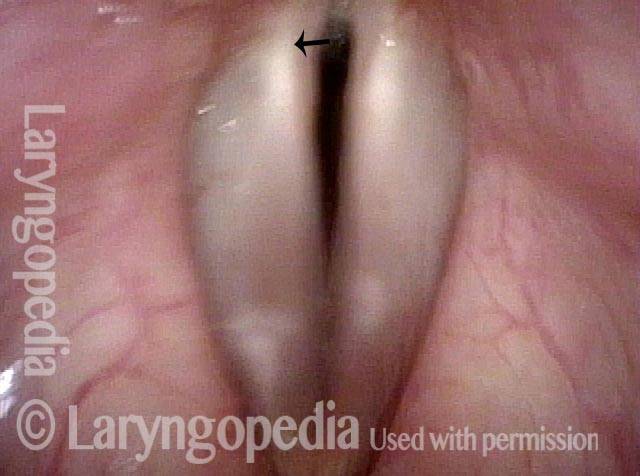
Phonation, LCA is intact (3 of 4)
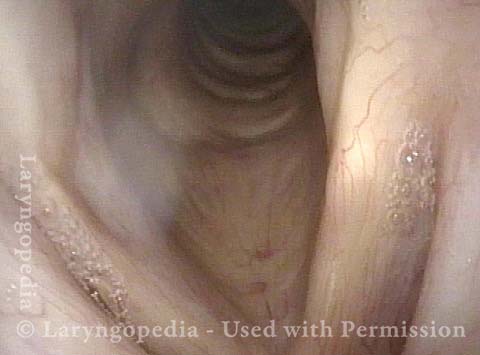
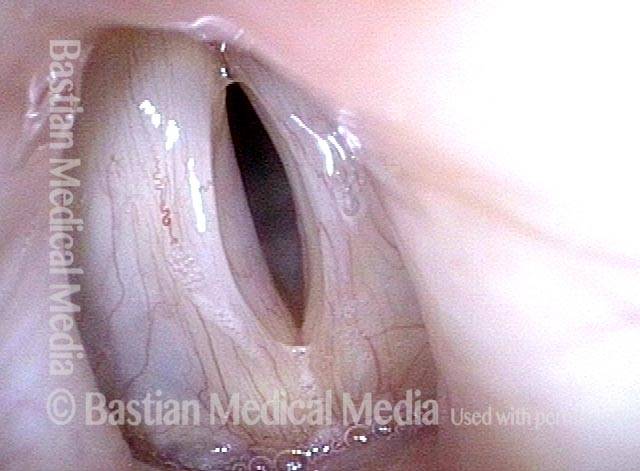
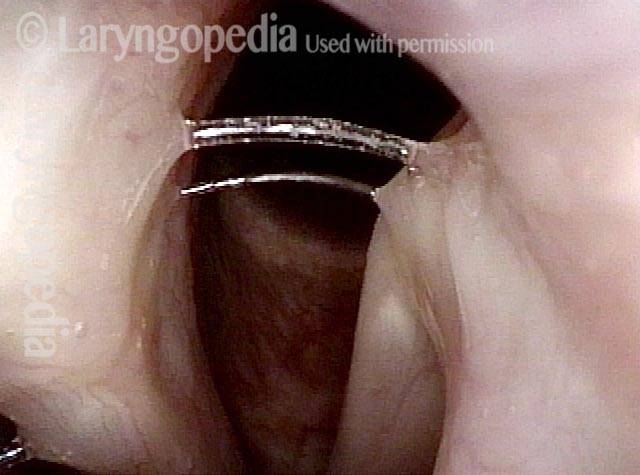
Phonation under strobe light, PCA-only paresis (4 of 4)
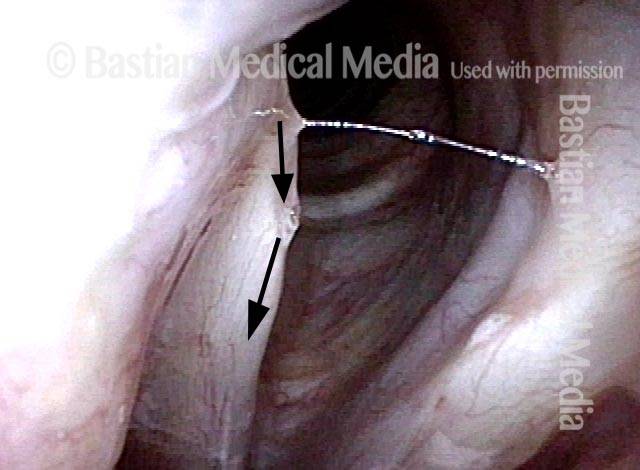
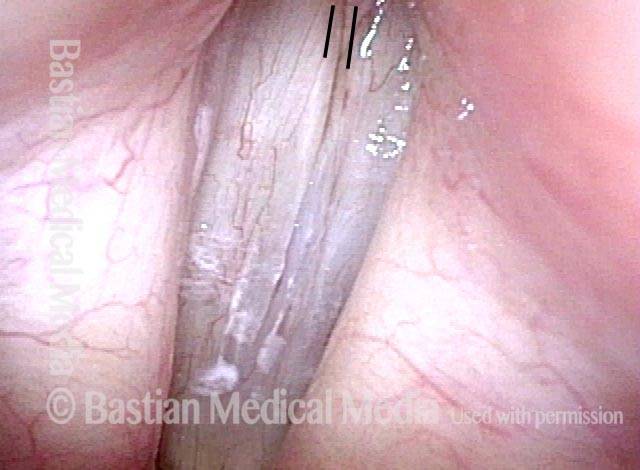
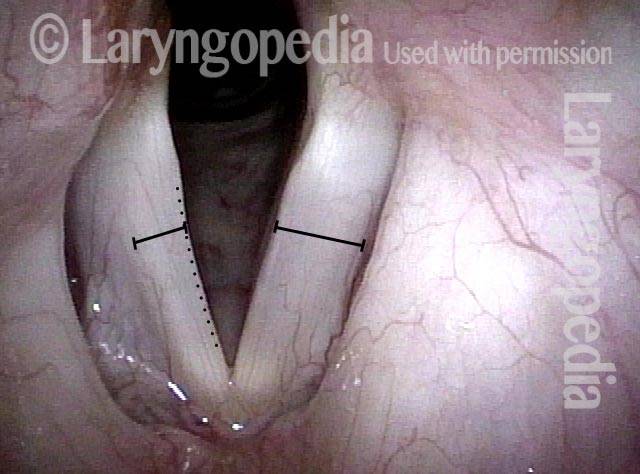
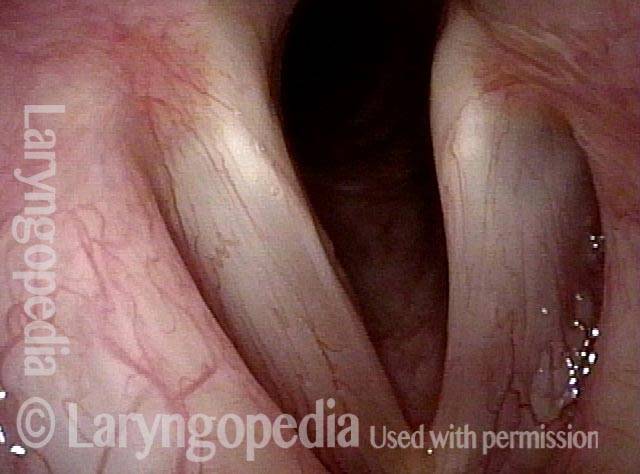
Sharp Observation Required to Sort out this PCA-only Paresis and Cancer Scar Combo
Unequal lateralization (1 of 4)
PCA not working (2 of 4)
Phonation, closed phase (3 of 4)
Phonation, open phase (4 of 4)
Classic Findings Again of PCA-only Paresis
Post thyroidectomy (1 of 4)
Phonatory view (2 of 4)

LCA and TA muscles working (3 of 4)
PCA-only paresis (4 of 4)

A Mediocre Examination for Paresis
PCA not working, TA is weak (1 of 3)
LCA recovered (2 of 3)

TA partially recovered (3 of 3)

Laryngology 401: PCA-only Paresis, but the Actual Voice Problem Is Spasmodic Dysphonia
Sense of instability (1 of 3)
Vibratory amplitude (2 of 3)
Spasm (3 of 3)
Test your Mastery of Visual Nuances of Paresis with this Case
LCA working, TA partially working (1 of 4)
Closer view (2 of 4)
Closed phase (3 of 4)
Open phase (4 of 4)

PCA-only Paresis of Right Vocal Cord and Normal Voice
Ineffective PCA Muscle (1 of 3)
Vocal muscles are recovered (2 of 3)

Signs of PCA-only paresis (3 of 3)
