
Leukoplakia as a Visual Red Herring
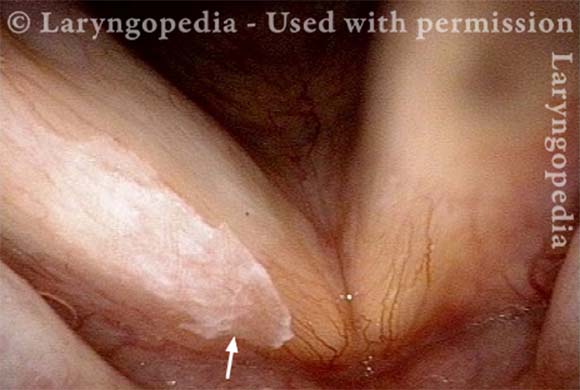
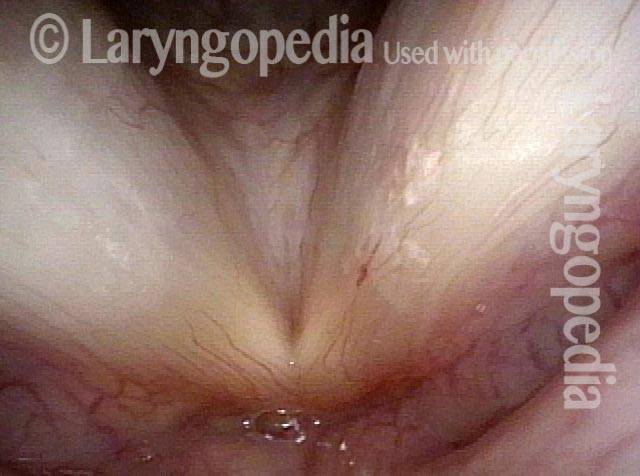
This middle-aged man came for evaluation and treatment of a “white lesion” that his doctors was seen elsewhere on a vocal cord, which they thought explained voice change. He had experienced that voice change suddenly a few months before (Red herring alert, as he was not a smoker, and white lesions do not usually appear and cause voice change abruptly).
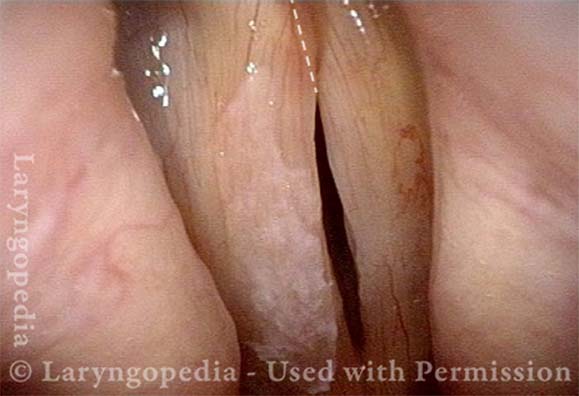
Furthermore, his main vocal issue was not so much hoarseness, as a tendency for the voice to fade with use across the day. This is not the usual phenomenology of leukoplakia, which would be expected to produce the same voice from morning to night. As it turns out, the leukoplakia was incidental to his voice change, which was instead due to scissoring / overlap of one cord on the other and bowing/flaccidity—possible TA-only paresis of the right cord.
The Red Herring Lesion (1 of 4)
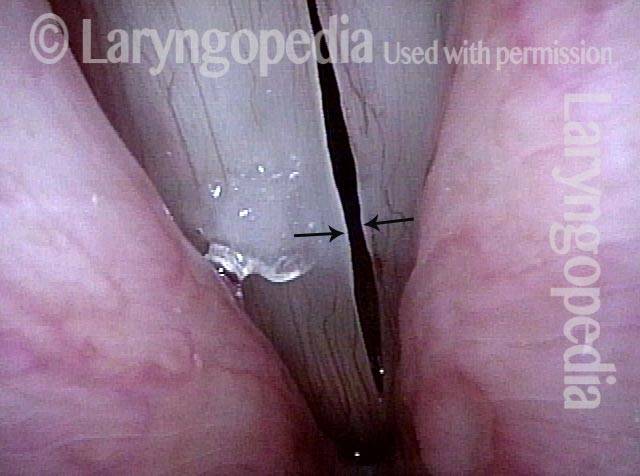
Bowing and scissoring (2 of 4)
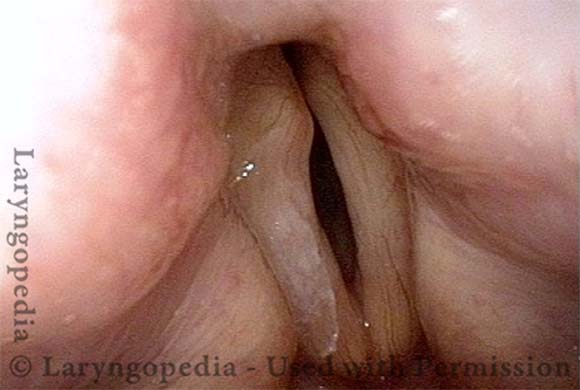
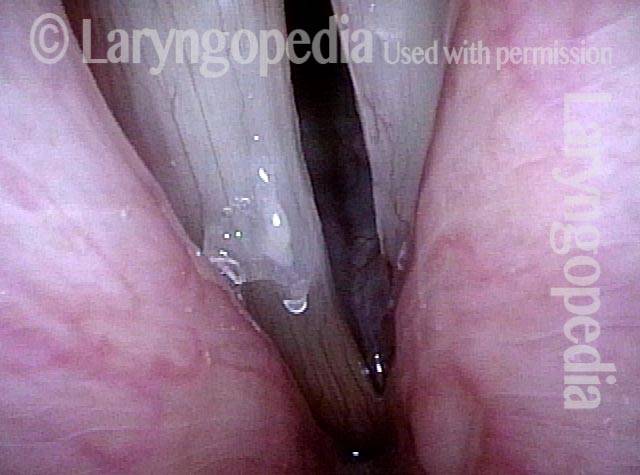
Strobe light, open phase of vibration (3 of 4)
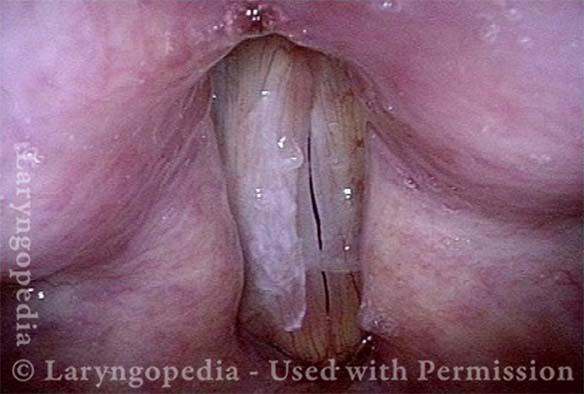
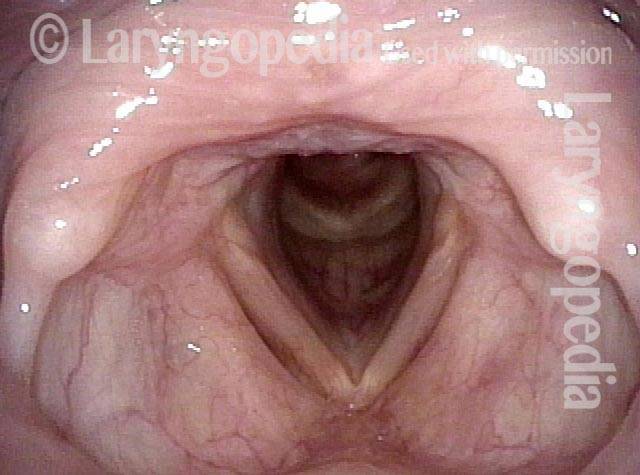
Closed phase of vibration (4 of 4)
Pushing Past Red Herrings to Find the Real Issue
Obvious lesion not important (1 of 3)

Granuloma (2 of 3)

Carpet-varient papilloma (3 of 3)

Red Herring Capillary Ectasia and Mucosal Injuries
Ectatic capillary (1 of 4)
Ectatic capillary, narrow band light (2 of 4)

Margin swelling (3 of 4)
Bowing, atrophy, and flaccidity (4 of 4)
Tracheal Stenosis Here Is A Red Herring; the Diagnosis Is Actually CPS
Tracheal stenosis? (1 of 4)
Narrowing at trachea (2 of 4)

Closer view (3 of 4)

No significant change in breathing (4 of 4)
