
Go Straight to Total Laryngectomy, or Give Thulium Laser a Chance?
Lesion (1 of 5)
Nearly 80-year old man in whom CT for another reason shows this lesion just below the vocal cords, left upper trachea. Comparison with CT 18 months earlier shows the same lesion, and it is now only a few mm larger than then. Note that this man has had partial pharyngectomy and postoperative radiotherapy 40 years earlier for a pharyngeal wall cancer.
Decisions (2 of 5)
A week after attempted removal with the laser in the O.R. Removal was only partial due to difficult anatomy. The pathology result was “papilloma, with focus of invasive squamous cancer.” Radiotherapy is not an option. Tracheal distortion is from tracheotomy 40 years before.
Removal (3 of 5)
The dilemma: Do a total laryngectomy with no cartilage destruction, the papilloma component, and such minimal progression over 18 months? Thus, the decision to do this aggressive laser ablation in the videoendoscopy procedure room. Surveillance will be intense, and total laryngectomy may still be necessary.

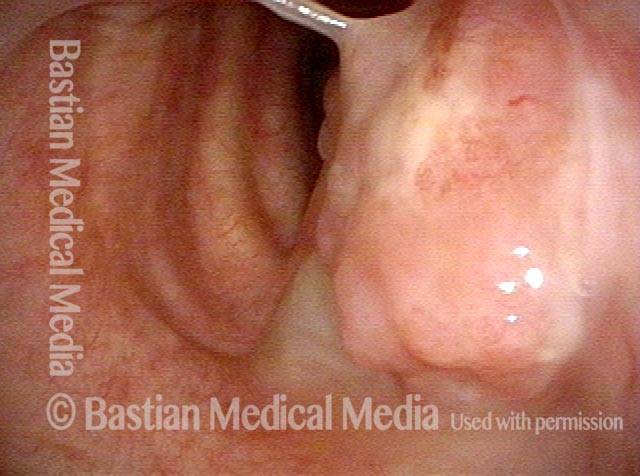
Bulk of tumor is gone (4 of 5)
After earlier thulium laser ablations and in preparation for another laser treatment on this day. The bulk of tumor is gone. The patient is cautioned each visit that we are taking a “non-traditional” approach given his strong aversion to total laryngectomy and the superficial nature of his lesion.

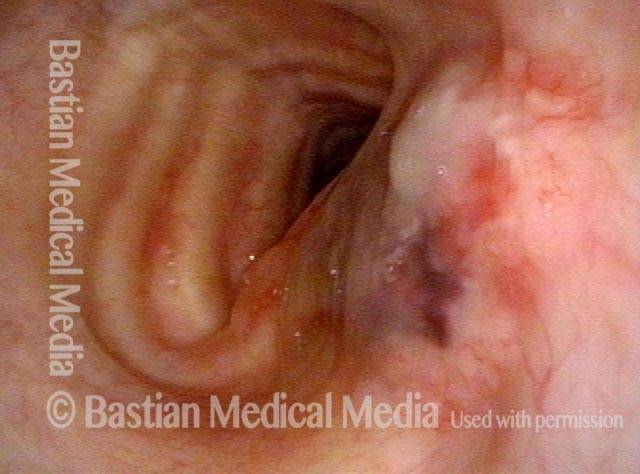
Complete healing? (5 of 5)
After several laser treatments across 8 months, the lesion appears to be gone, and the hope is that the lesion was superficial enough that this may suffice with careful surveillance.
Unfortunately, a CT scan showed some deeper invasion and laryngectomy was required about a year after the original laser treatment.

How a Sphincter Works
Open (1 of 2)
After total laryngectomy, the upper esophageal sphincter is open here for a brief moment, allowing one to see beyond into the esophagus.

Contracted (2 of 2)
A moment later, the sphincter contracts, as though the purse string of a velvet jewelry bag had been tightened.

How the One-Way Flapper Valve Works in A Tracheo-Esophageal Voice Prosthesis
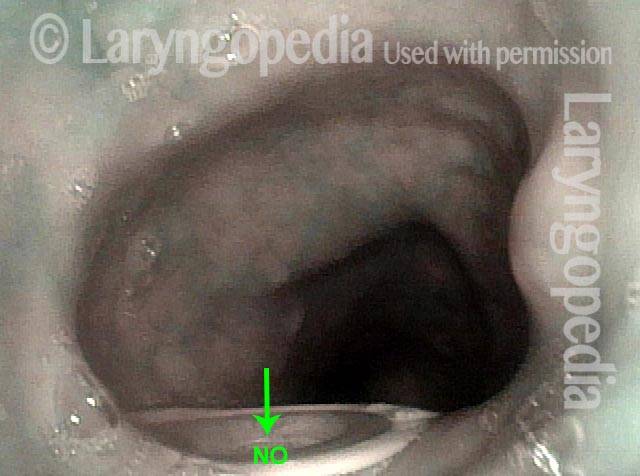
Food and liquid blocked from trachea (1 of 3)
This view is just inside the upper esophagus in a man who has undergone laryngectomy. The white-edged “disc” at the bottom of the photo is the inner flange of the TEP device. The arrow points towards the valve just inside the flange. This valve says “no” to any food or liquid that wants to pass in the direction of the arrow and into the trachea (not seen here).
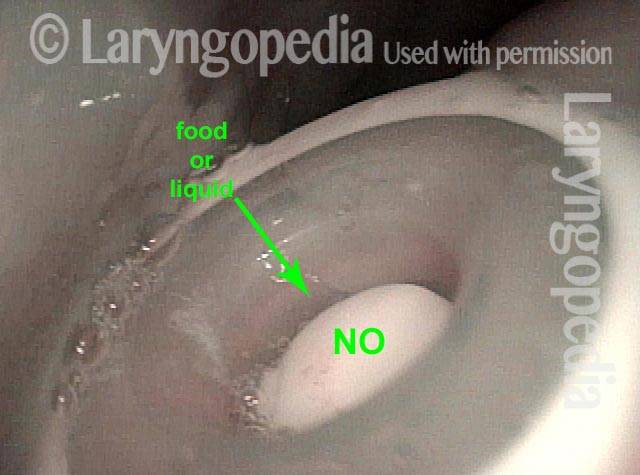
Closer look at closed valve (2 of 3)
Here, we see the flapper valve more clearly. Again in its “closed” position, it will not let food or liquid enter.
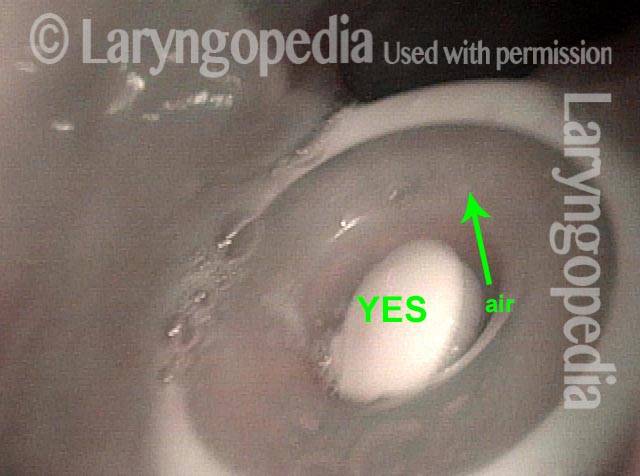
Opened valve (3 of 3)
Now we see the flapper valve lifted out of its housing. The patient is placing his thumb over the tracheostome (not seen here) and diverting air through the TEP device and into the esophagus. The esophageal walls are brought into vibration to produce continuous, pulmonary air-powered esophageal voice.
Endoscopic Laser Cricopharyngeal Myotomy to Salvage Tracheoesophageal Voice After Total Laryngectomy
Development of voice after tracheoesophageal puncture, following laryngectomy, is sometimes hampered by spasm of the cricopharyngeal muscle...