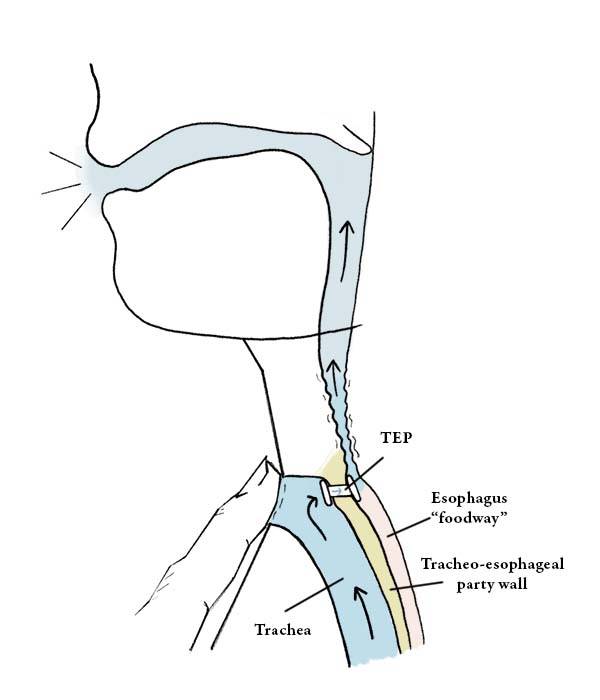

The Use of a TEP
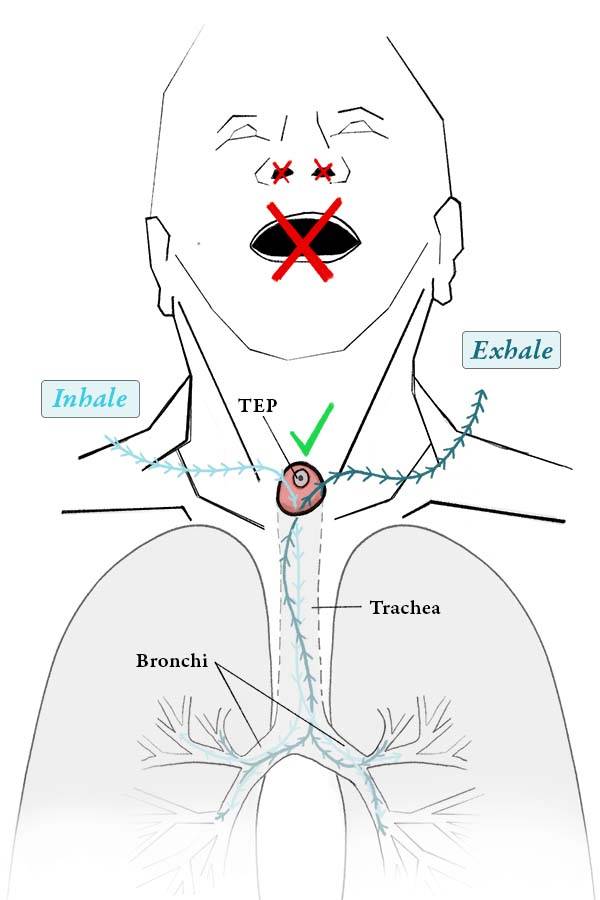
When a patient with a TEP device wants to speak, he or she must momentarily cover the stoma in the front of the neck, so that air coming up from the lungs is redirected through the TEP and into the esophagus to make voice. Some patients will simply cover the stoma as needed with their thumb, if their stoma is normally left entirely open, or is only concealed from view with a small, unobtrusive, breathable cloth.
More commonly, however, the patient’s stoma is fitted with a housing, into which is placed a heat and moisture exchanger (HME); in these cases, the HME, which looks like a flat, plastic button, can be pushed as needed to block the stoma and enable voicing. Whatever the case, speaking with a TEP device is a learned skill and requires training through speech therapy.
Tracheoesophageal voice prosthesis (1 of 4)
Tracheoesophageal voice prosthesis (2 of 4)

Tracheoesophageal voice prosthesis, corrected fitting (3 of 4)
Tracheoesophageal voice prosthesis, during voicing (4 of 4)
Hands-Free Tracheoesophageal Voice
After laryngectomy, most people prefer to glue a small voice button over the stoma that they push when they wish to speak. When not pushed, the button springs up and allows air into the trachea.
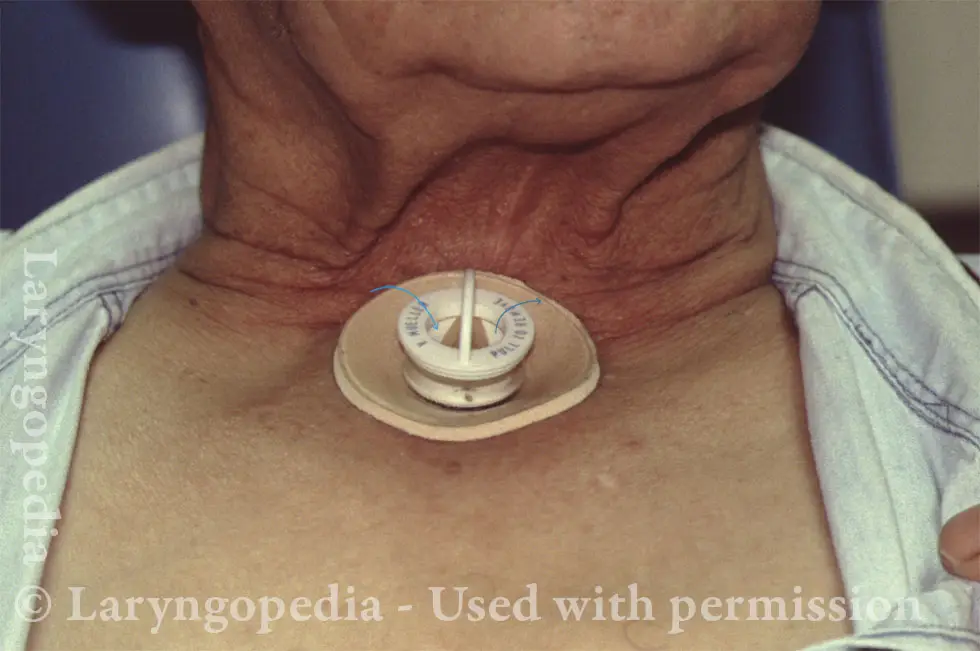
This person is instead using a hands-free valve. He can initiate voice by beginning each sentence with a little “kick” of exhaled air that closes a flexible diaphragm and diverts pulmonary air through the TEP device and into the pharyngoesophageal segment.
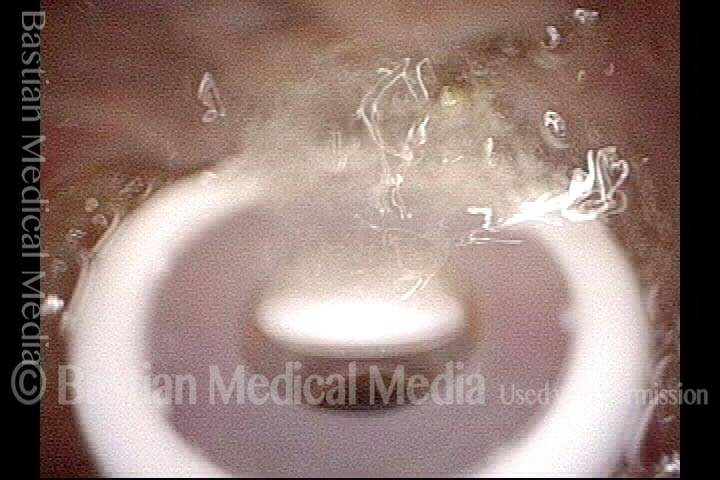
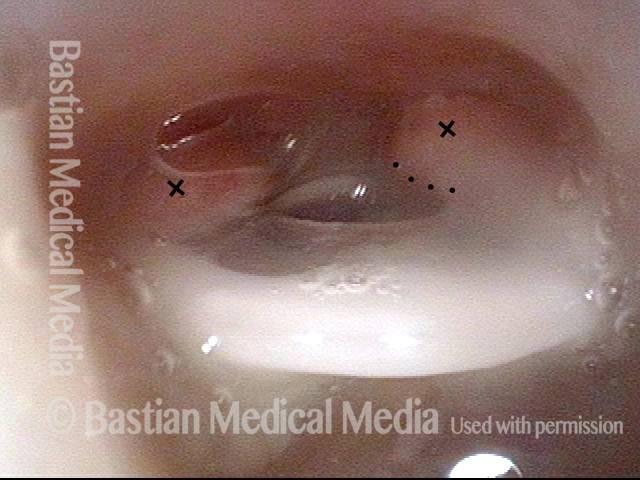
Hands-Free TEP when breathing
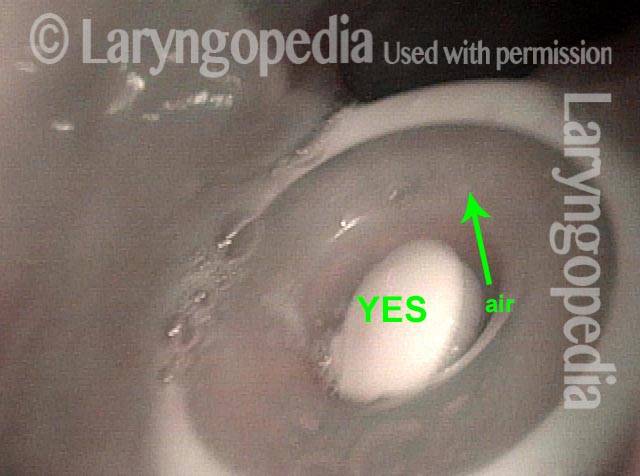
Here is the hands-free device during quiet breathing. It is attached with a biological glue to the skin that surrounds the stoma. When this man breathes in, the path of air follows the arrows into the “open white crescent” on either side of the tan flutter valve. When he breathes out normally, the air travels though the same space in the opposite direction.

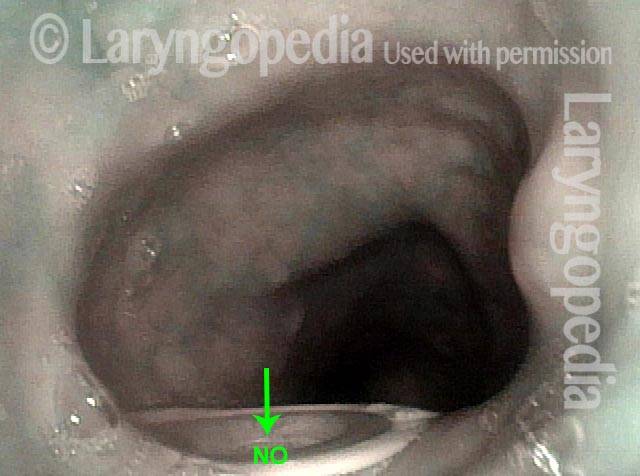
Hands-free TEP during voicing
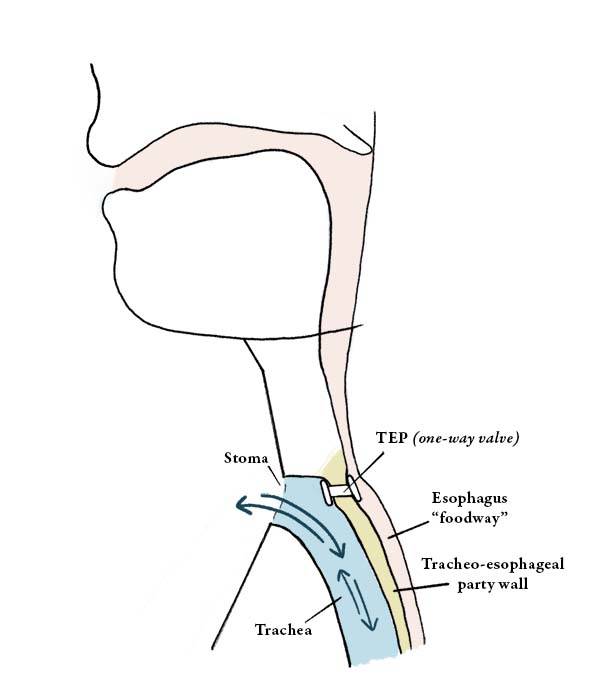
If he “kicks” the air out slightly, the curled diaphragm unfurls in an outward direction and plugs the passage, so that air is diverted through the tracheoesophageal prosthesis (not seen here). The result: hands-free tracheoesophageal voice.
TEP Voicing
Hypopharynx of a tracheoesophageal voice prosthesis patient (1 of 4)
Hypopharynx, as the tracheoesophageal voice prosthesis patient makes voice (2 of 4)

Tracheoesophageal voice prosthesis (3 of 4)

Tracheoesophageal voice prosthesis, as the patient makes voice (4 of 4)

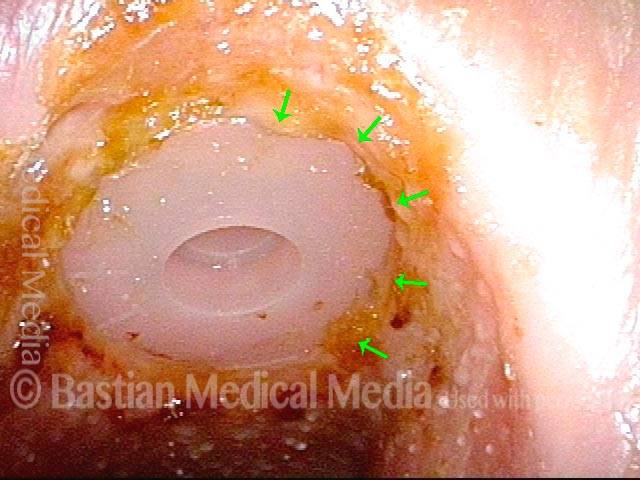
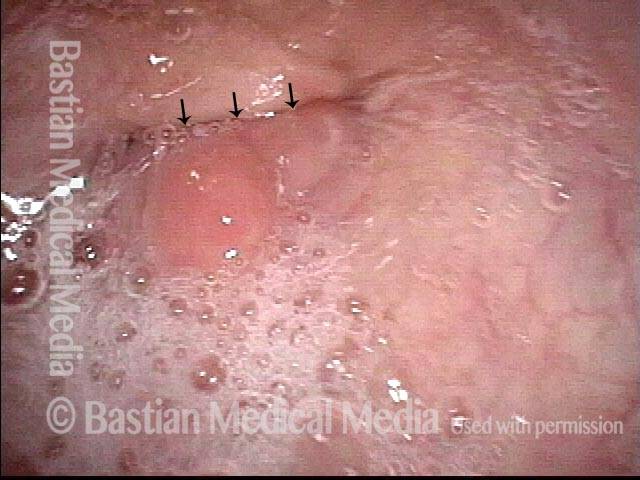
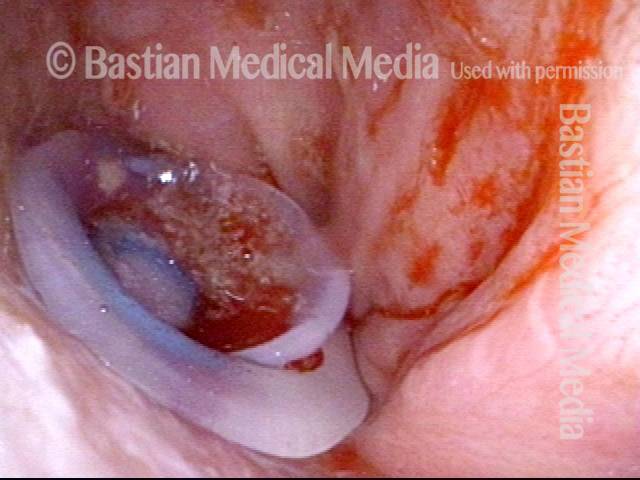
TEP’s that Want to Become Buried
TEP buried (1 of 4)
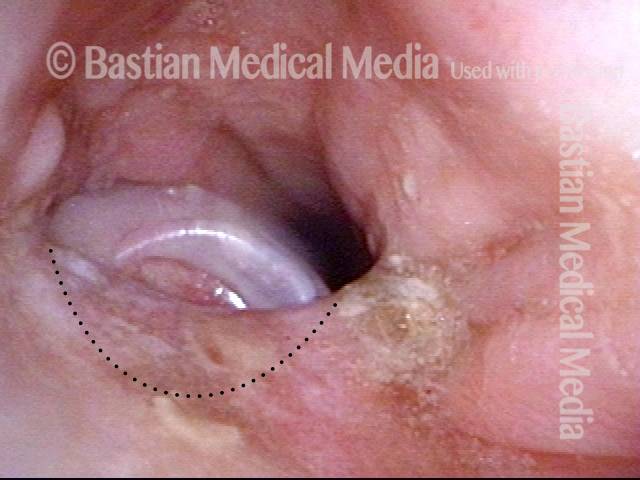
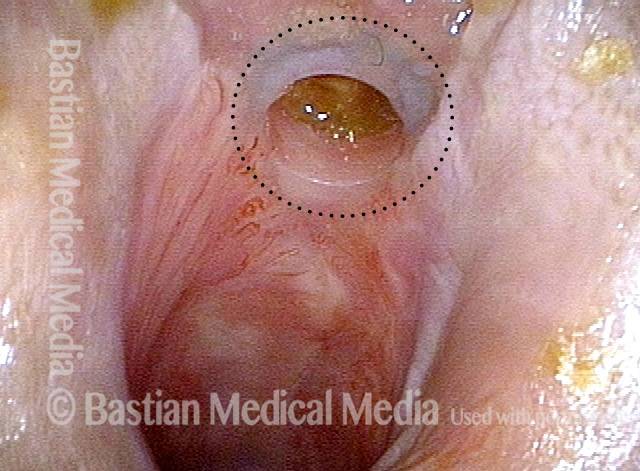
Re-inserted and re-positioned TEP (2 of 4)
Tissue overgrowing flange (3 of 4)
Flange partially buried (4 of 4)
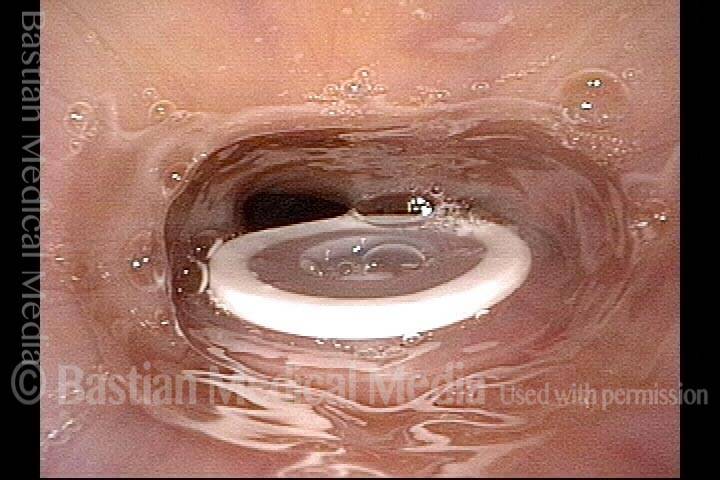
How the One-way Flapper Valve Works in a TEP Prosthesis
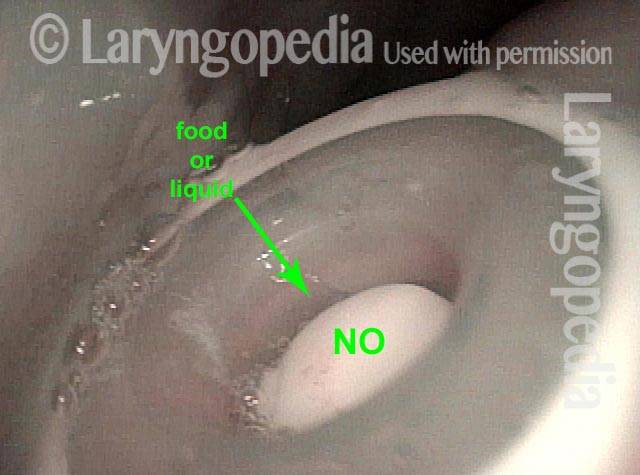
Food and liquid blocked from trachea (1 of 3)
Closer look at closed valve (2 of 3)
Opened valve (3 of 3)