Photo Examples
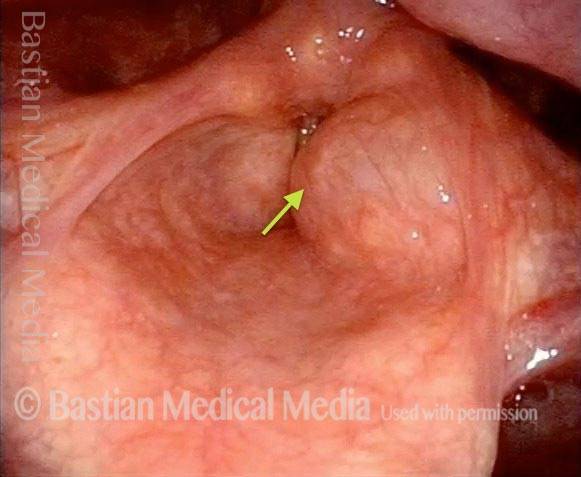
Laryngocele (1 of 5)
Before phonation begins: the laryngocele is not visible.
Saccule (2 of 5)
Phonation begins: the saccule suddenly begins to inflate.
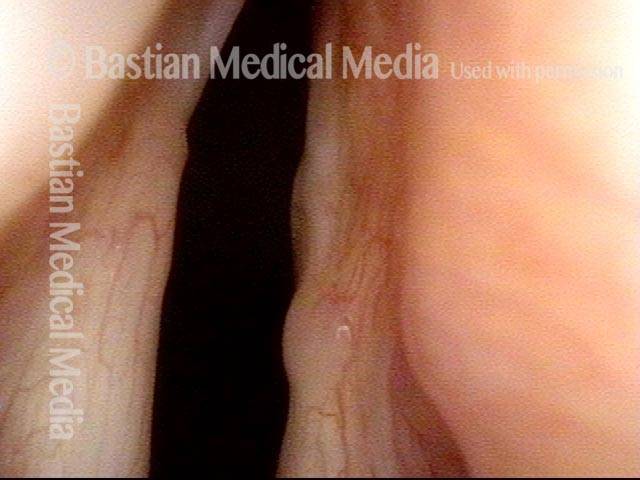
Saccule blocks airway (3 of 5)
The saccule is at peak inflation. Note how this obstructs the laryngeal airway.
Phonation ending (4 of 5)
The saccule is deflating. Note the motion blur; inflation and deflation each happens in a fraction of a second.

Phonation ended (5 of 5)
The laryngocele is again fully deflated and hidden from view.
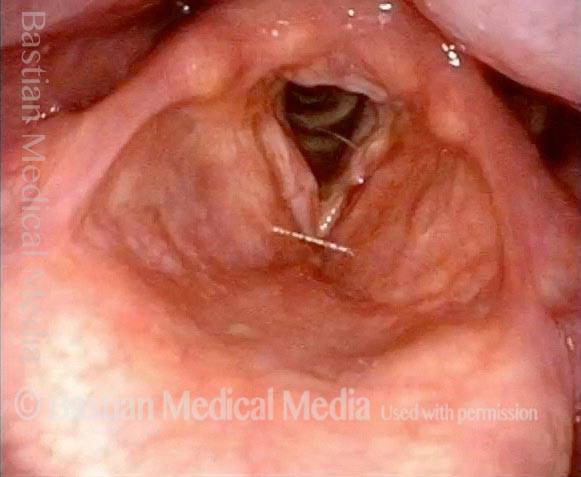
Bilateral Laryngocele, Before and After Removal
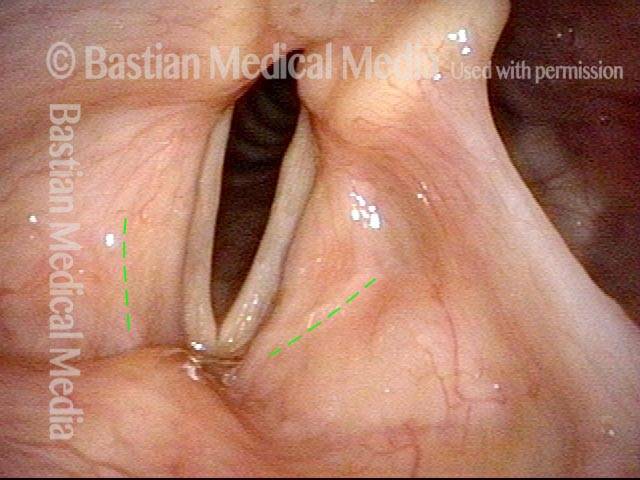
Bilateral laryngocele (1 of 8)
Vocal cords approaching point of best closure possible (due to left cord paresis). Faint dotted lines outline the approximate boundary of each laryngeal saccule, which not yet inflated.

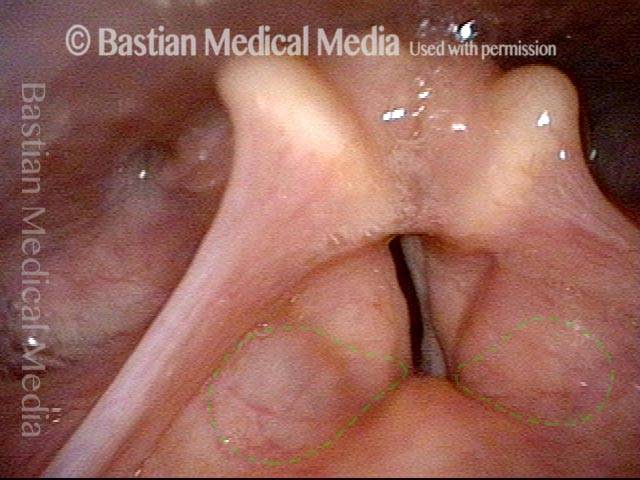
Bilateral laryngocele (2 of 8)
As air just begins coming upward between the cords, one can see subtle inflation (dotted lines), particularly of the right saccule (left of image).

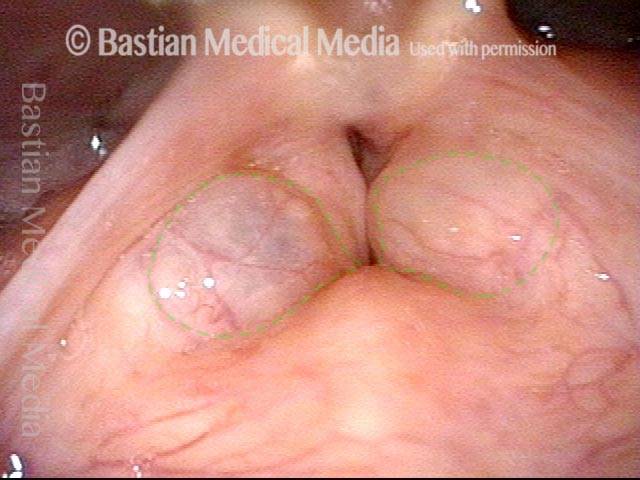
Bilateral laryngocele (3 of 8)
As phonation continues, inflation of the (now diagnosable) laryngocele becomes obvious, and the left laryngocele (right of image) is now more obviously inflated than before, again indicated by the dotted lines.
Bilateral laryngocele (4 of 8)
Near the end of a sustained period of voicing, maximum inflation of the laryngoceles is seen (dotted lines). On the right side (left of image), the stretching mucosa is so thinned as to appear translucent.
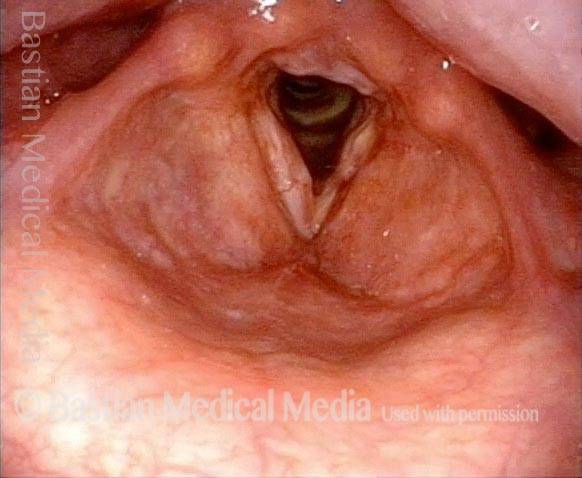
Bilateral laryngocele, after removal (5 of 8)
Same patient, breathing position, 12 weeks after complete removal of the bilateral laryngoceles via false cord incisions (lines of incision shown by dotted lines). This patient also has long-standing paralysis of the right vocal cord (left of image) and limited mobility of the left cord, so the cords don’t open fully for breathing.
Bilateral laryngocele, after removal (6 of 8)
Phonatory position. Note the lack of inflation of the now-absent laryngoceles, and compare that with photos 3 and 4 of this series.
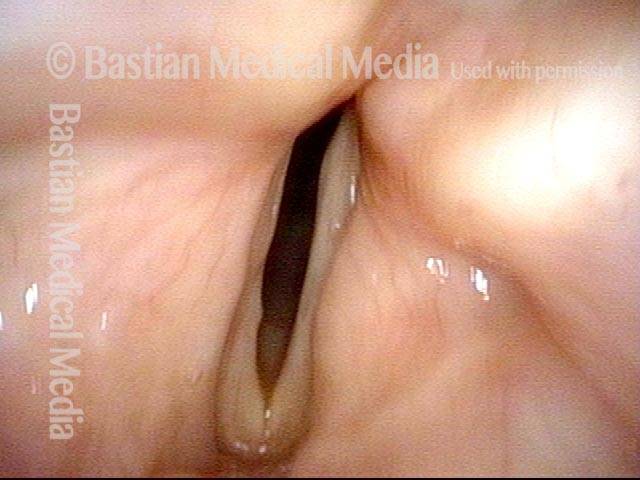
Bilateral laryngocele, after removal (7 of 8)
Closer view of the posterior ends of the true vocal cords during maximal abduction for breathing. Space between the vocal cords is an estimated 50% of normal, because of the paralyzed right cord and the limited mobility of the left cord.

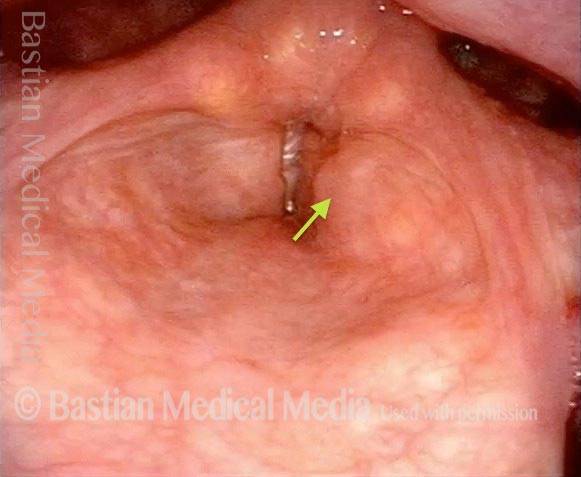
Bilateral laryngocele, after removal (8 of 8)
Same close-up view, but during phonation. The left vocal cord (right of image) has shifted slightly toward the midline, but the cords do not actually close and, thus, the patient cannot produce glottic (true vocal cord) voice. An implant could help to close this gap, but the patient will first try developing a “false cord voice.”