
Cake Icing and Spilled Milk Leukoplakia after Covid in a Former Smoker
This is a person who had smoked ½ pack per day for a little over a decade but stopped nearly 15 years ago. Voice was always normal until Covid-19 infection (despite vaccination). Laryngitis occurred during that illness and never resolved across six months to the time of this examination.
He is hoarse but voice is functional for basic communication. After supportive (acid reflux, etc.) treatments failed to resolve these lesions, microlaryngoscopy with meticulous “basement membrane” peeling of these lesions will follow.
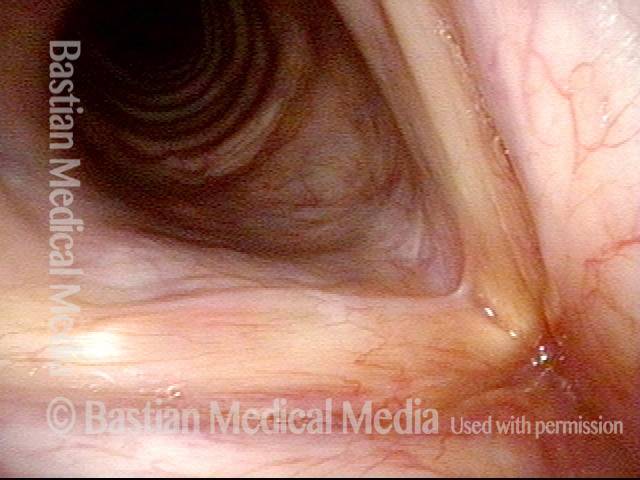
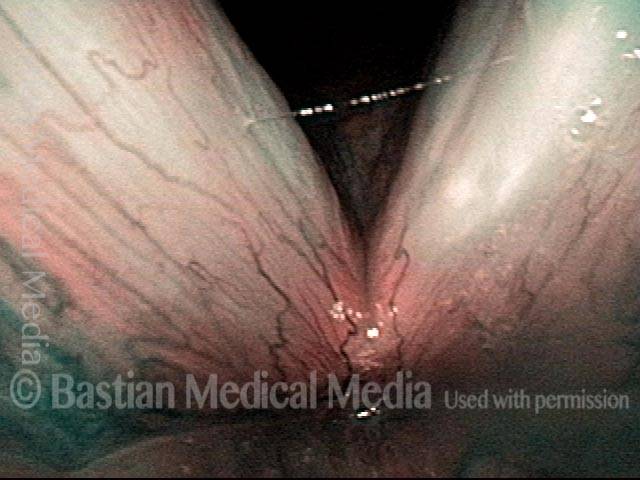
Leukoplakia (1 of 16)
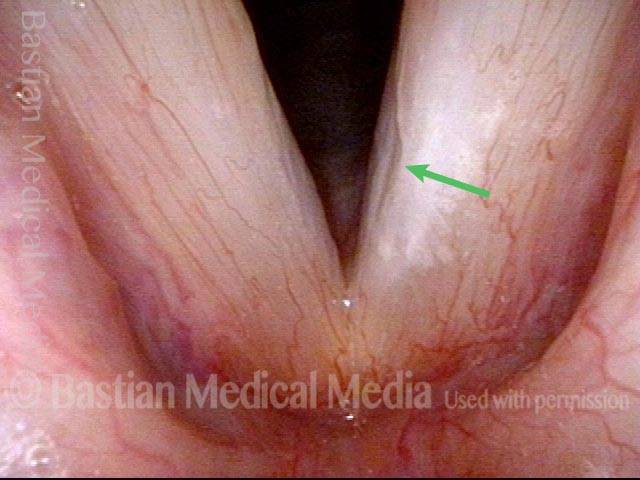
The view from a distance shows a kind of “chapped lip” leukoplakia involving almost all of both vocal cords. There are elevated “cake icing” areas. The hazy “spilled milk” type of leukoplakia is seen better in subsequent photos. Note the lack of inflammation in the false vocal cords (arrows).
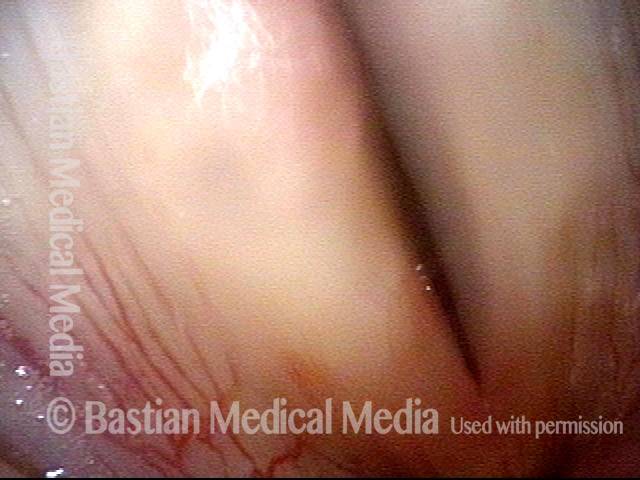
Spilled milk Leukoplakia (2 of 16)
At closer range, one can see that the leukoplakia around the projecting “cake icing” component is of the spilled milk variety. See tiny arrows that indicate examples of this more hazy component.
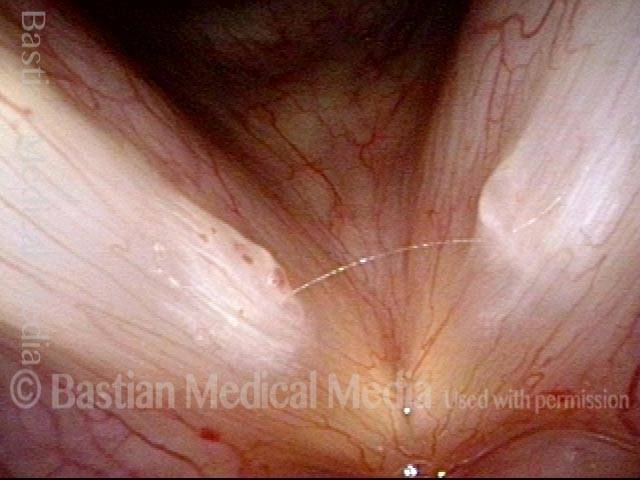
Superficial ulceration (3 of 16)
Under narrow band (blue-green) light, an area of superficial ulceration is also outlined on the right cord (left of photo), and there is a smaller similar area on the left cord (right of photo).

Closed phase of vibration (4 of 16)
Under strobe light, here is the closed phase of vibration. There is a reasonably good match of both vocal cord margins.

Stiff mucosa limits vibration (5 of 16)
The open phase of vibration is seen here under strobe light. The mucosa only vibrates at low pitch due to stiffness of the mucosa.

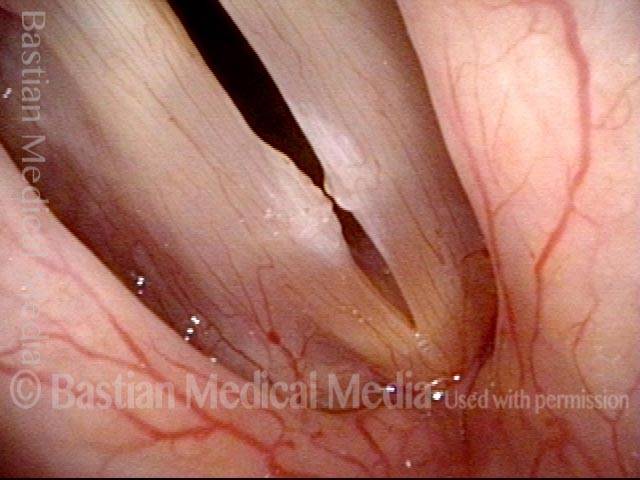
Operative view, first surgical procedure (6 of 16)
Here, we see the surgical view at his first microlaryngoscopy procedure. Note that the “V” of the office view is now “upside down” in the operative view.
Peeling begins (7 of 16)
Though the aiming beam is “smeared” photographically, at the time of surgery it is focused to a pinpoint spot on the junction between the leukoplakia and (conceptually) the basement membrane of the “first normal cell layer.” Reinke’s space is not entered.
Can be relatively bloodless (8 of 16)
With less inflammation than in some with leukoplakia, the dissection is relatively bloodless. Often, tiny capillaries on the surface of the base of removal remain intact.
Near complete (9 of 16)
After both sides are peeled. Some final debridement was done, but there is no photo available for the final result.
Leukoplakia diminishes (10 of 16)
About 4 months after a meticulous “basement membrane” peel of the leukoplakia seen in the prior 5 photos, voice is dramatically improved and we have “won territory, but not (yet) the war.” The right vocal cord (left of photo) is particularly improved.

Residual leukoplakia (11 of 16)
At closer range, one can also see that the residual leukoplakia seems more focal and defined. Additional surgery is planned to see if further territory can be won. In some cases it can be; in others, the leukoplakia continues to recur aggressively.

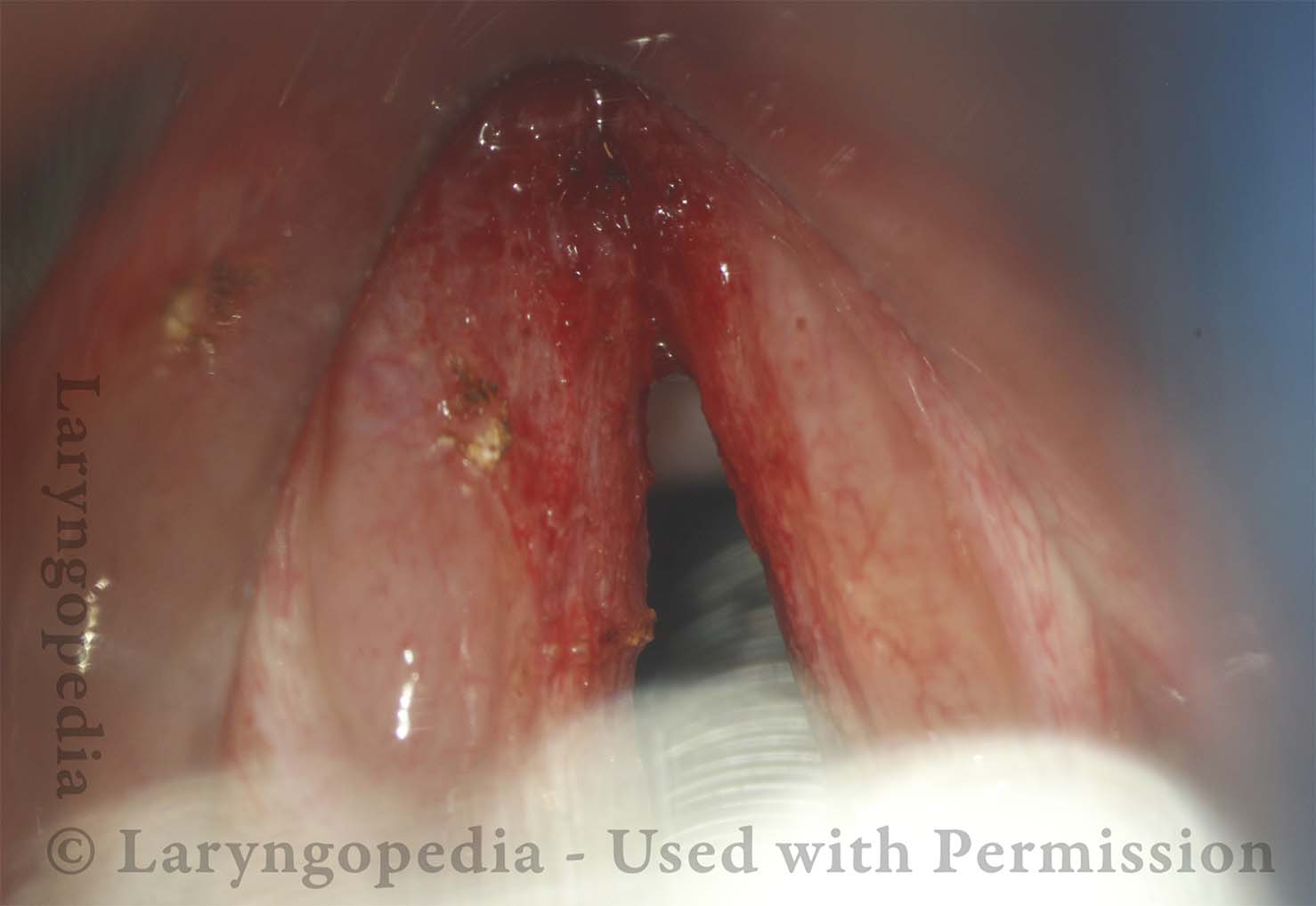
Hazy grey is surgical wound not leukoplakia (12 of 16)
One week after surgery, the cords display grey pseudomembranes; the surgical “wound” has not yet been mucosalized. Think of the white “wound” when you bite your cheek. Reminder: The “peel” was so superficial, that vibratory flexibility should be preserved. Dots of persistent leukoplakia left cord (right of photo) are already evident (arrows).

About to win more territory (13 of 16)
Initial operative view at microlaryngoscopy #2. Most of the territory has been won on the right. We are attempting to win the rest during this procedure…

Second battle (14 of 16)
Basement membrane peel is a little more difficult on the upper surface of the cord, and again there is no final photo of the surgical result (after removal of a few charred crusts).

Winning the war (15 of 16)
In this suboptimal examination, many months after the final microlaryngoscopy, it appears that the “war” with this man’s leukoplakia has been won. There are of course reticulated capillaries that signify regenerated mucosa. He considers his voice to be normal. The cords match during phonation very well. This is the longterm, stable, “final” result.

Good vibratory flexibility (16 of 16)
Open phase of vibration showing equal amplitude and very good vibratory flexibility. The repeated “basement membrane peels” have not damaged mucosal oscillatory flexibility.

Leukoplakia, Before and After Surgical Removal
Diffuse leukoplakia (1 of 7)
Diffuse leukoplakia (seen under standard light) in a man who had undergone removal elsewhere at least twice, with rapid return of diffuse disease on both vocal cords.
HPV effect (2 of 7)
Closer view, using narrow-band illumination. Leukoplakia is accentuated, but punctate vascular markings are also accentuated. We sometimes call this “HPV effect,” though in fact this man’s HPV subtyping was negative.
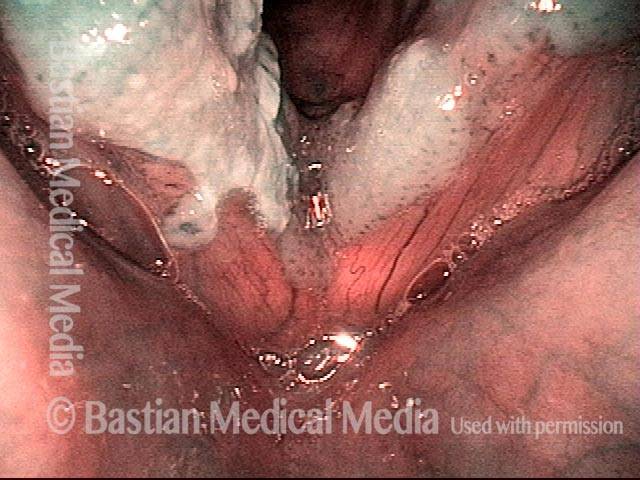
Surgical view (3 of 7)
Initial operative view. Note inversion of the photo (the “V” of lab view has become ^ in the operative view.

Basement membrane peeling (4 of 7)
During “basement membrane peeling.” One can see that the leukoplakia has been peeled like a piece of parchment. There is more bleeding than is often seen with this technique, but vibratory function should not be damaged because there has been no entry of Reinke’s space (lamina propria).

Removal complete (5 of 7)
After complete removal of the leukoplakia on not only right, but also left vocal fold.

Two years post-op (6 of 7)
Two years after one superficial yet intensely precise peeling of the leukoplakia, plus one follow-up thulium laser ablation of scattered residual disease. The patient, a tenor, considers his voice to be normal. Closed phase of vibration, as seen under strobe light.

Mucosa is flexible (7 of 7)
Open phase of vibration, demonstrating that the mucosa on both vocal cords remains flexible. The shifting hazy patches seen here and in photo 6 are collections of mucus.

Photo Examples of Leukoplakia
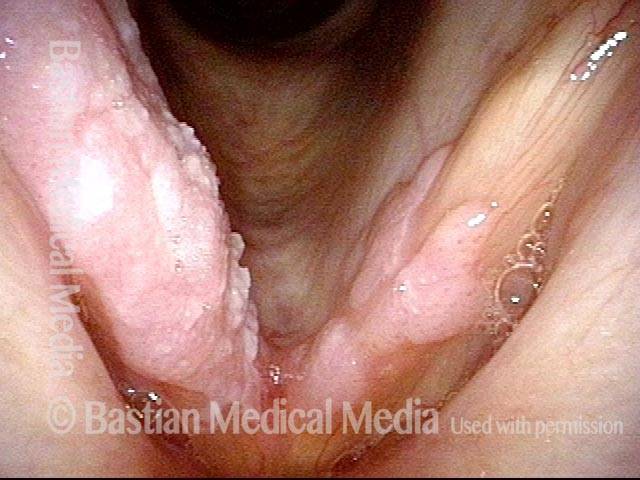
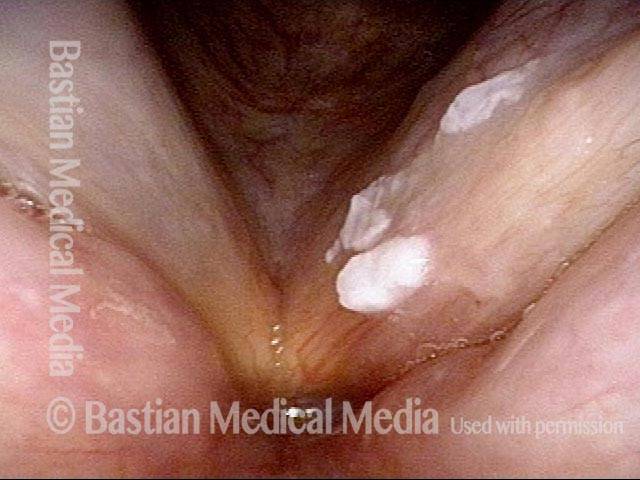
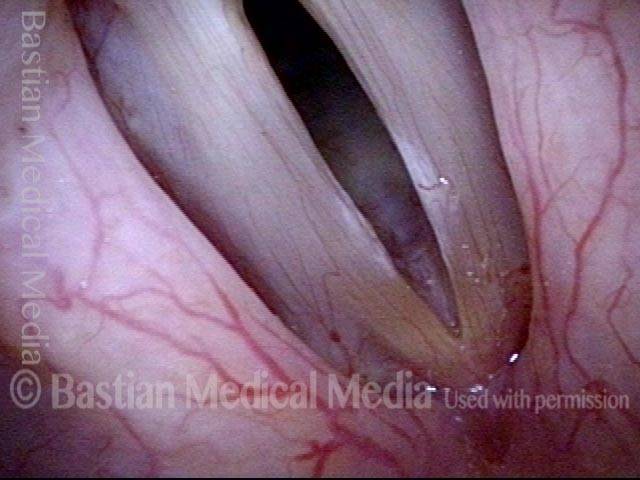
Cake-icing Leukoplakia (1 of 4)
The leukoplakia here is heaped up in three main areas, as what some might call “cake-icing” leukoplakia. With this view only, a person could easily overlook the second component of “hazy” or ” spilled milk” leukoplakia shown in the next three photos. All of this leukoplakia would be considered “bland” and non-threatening because there is no component of vascular prominence or erythema (erythroplasia). Erythroplasia would much more strongly indicate the need for biopsy.
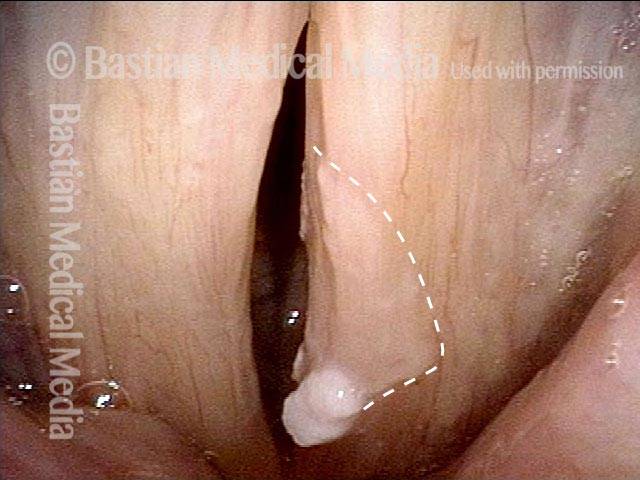
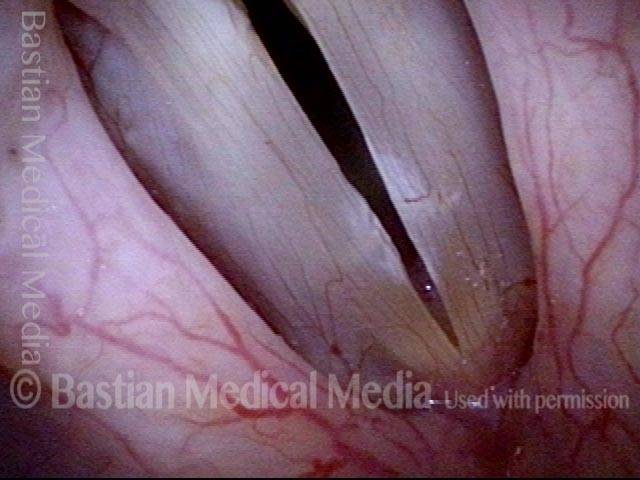
Hazy Leukoplakia (2 of 4)
Pre-phonatory phase, showing mild bowing of the vocal cords. There is also the hazy leukoplakia component indicated by the dotted line.
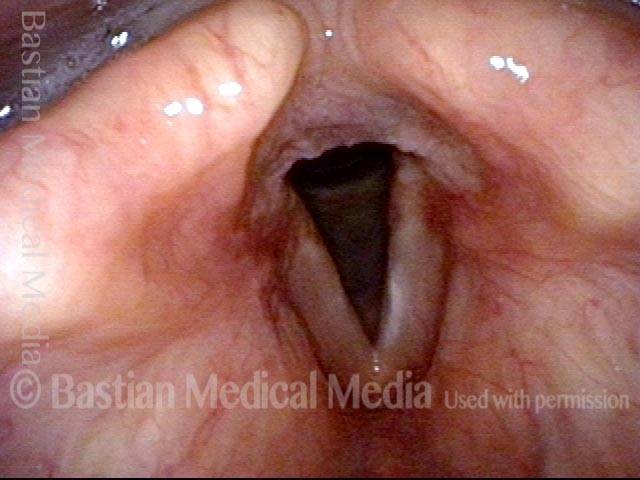
Leukoplakia (3 of 4)
Vocal cords are in the nearly closed phase of vibration. The bluish light from the strobe light makes the hazy leukoplakia even more evident (indicated by the dotted line).

Closer look (4 of 4)
Open phase of vibration, shown under strobe lighting.

Example 2
Leukoplakia (1 of 2)
Leukoplakia, left vocal cord (right of image), standard light.

Leukoplakia (2 of 2)
Same lesion, under narrow band illumination.

Leukoplakia Battled Over Time
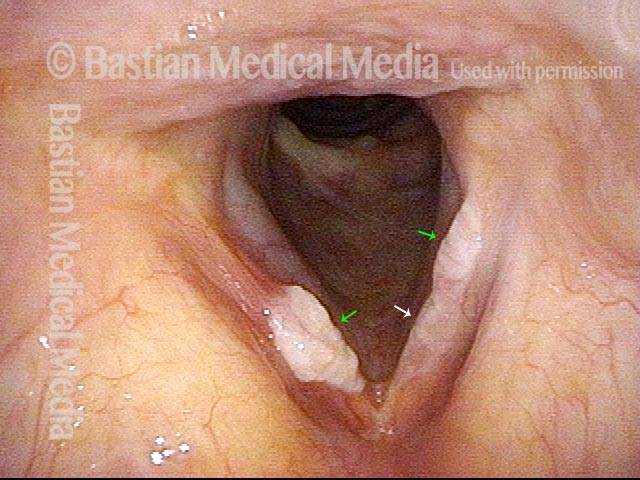
Leukoplakia (1 of 8)
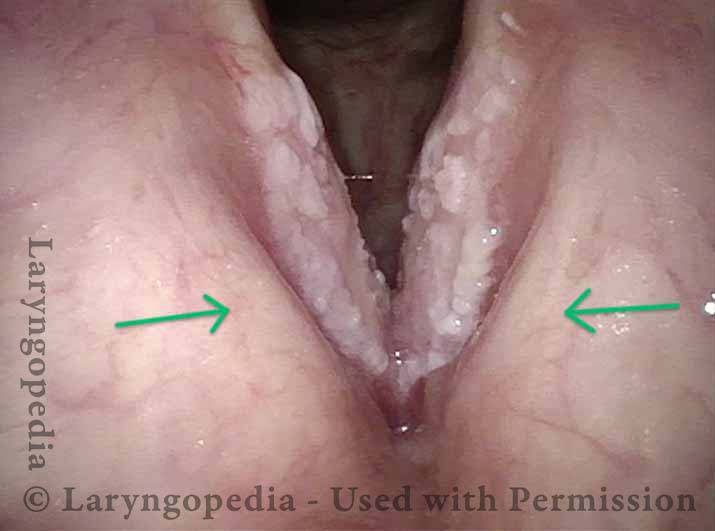
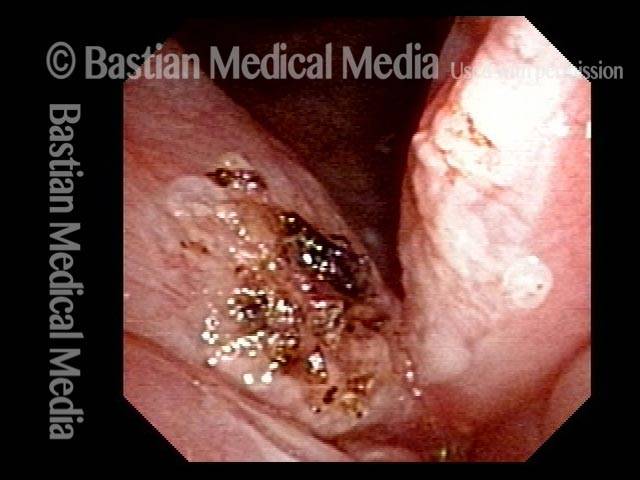
Leukoplakia, recurrent, in a former smoker, several years after initial diagnosis. The patient has had this removed in the operating room several times elsewhere, and pathology has only shown hyperkeratosis. HPV testing is negative. Notice both the “cake icing” (green arrows) and “spilled milk” (white arrow) components of the leukoplakia. At this examination, the patient is severely hoarse.
Spilled Milk (2 of 8)
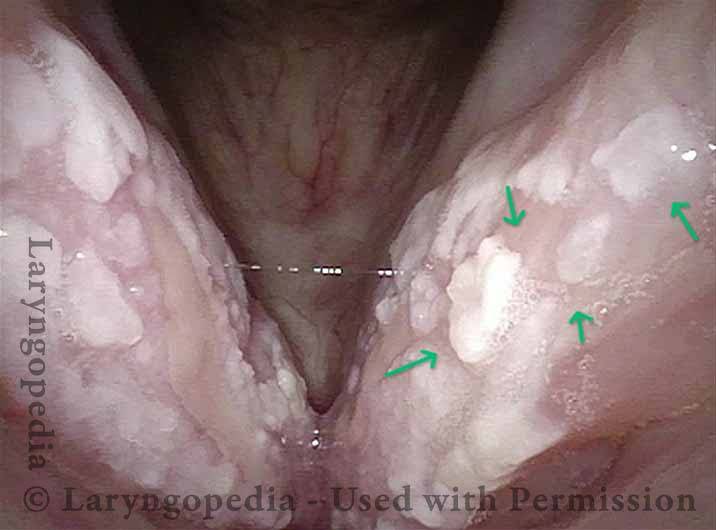
Closer view, under narrow-band illumination, which accentuates in particular the “spilled milk” component (arrows) of the leukoplakia on the left vocal cord (right of image).

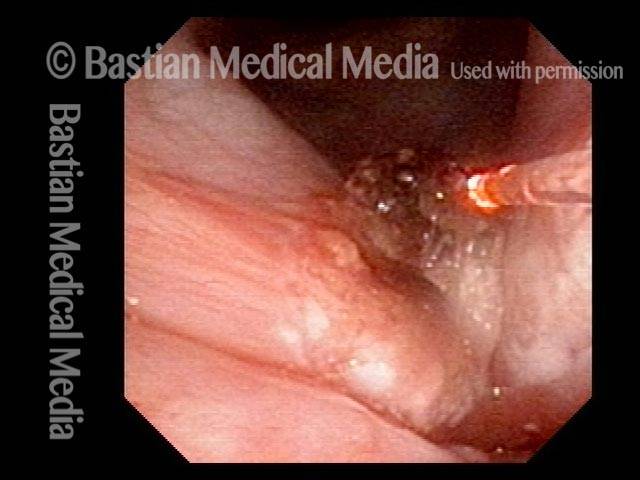
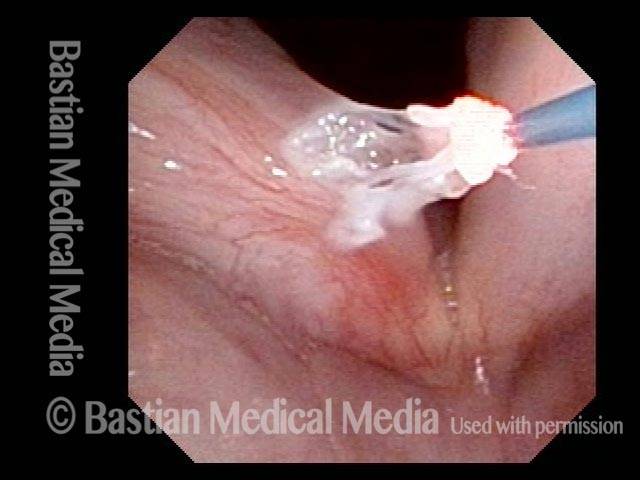
Thulium laser (3 of 8)
In the midst of coagulation using the thulium laser, delivered via glass fiber (right of image).
Coagulated tissue (4 of 8)
The thulium laser session is done. On the left cord (right of image), mostly near-contact mode was used, and the coagulated tissue, which has gone from leukoplakia-white to coagulated-white, will slough off within days. On the right cord (left of image), contact mode was used, to coagulate more deeply and detach the bulkier lesion. An additional surface layer will also slough on this cord.
Leukoplakia (5 of 8)
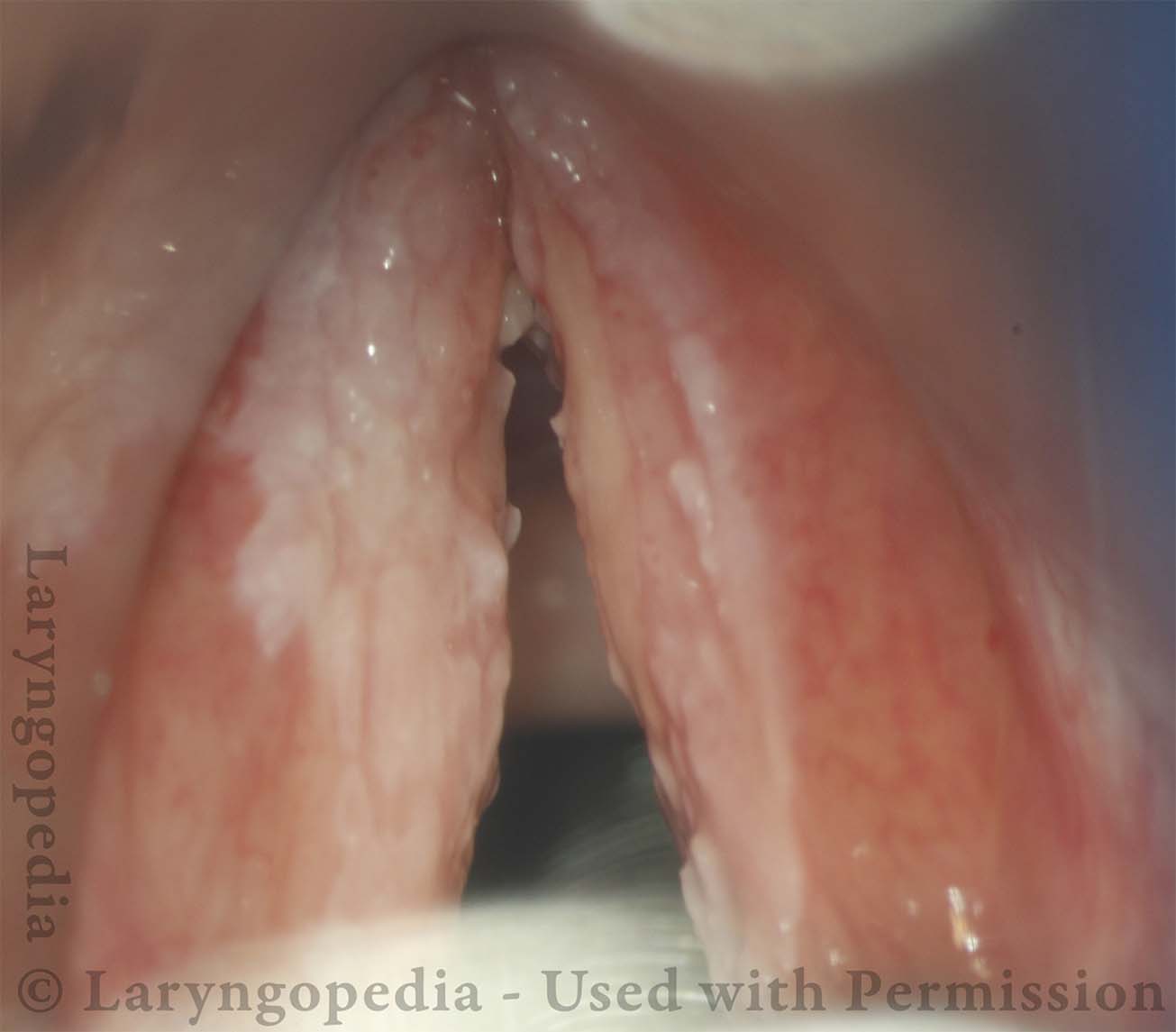
A year and a half later, after a few interval laser treatments, there is a small persistent patch of leukoplakia.

Detachment (6 of 8)
At the conclusion of another thulium laser procedure, using brief contact mode for superficial detachment of the patch of leukoplakia.
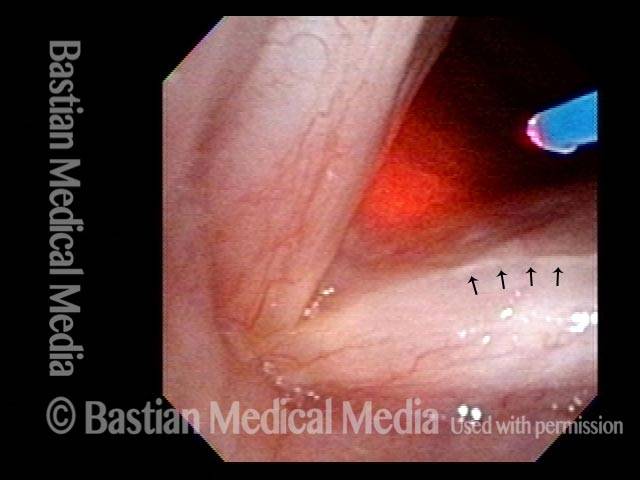
Superficial vascular pattern (7 of 8)
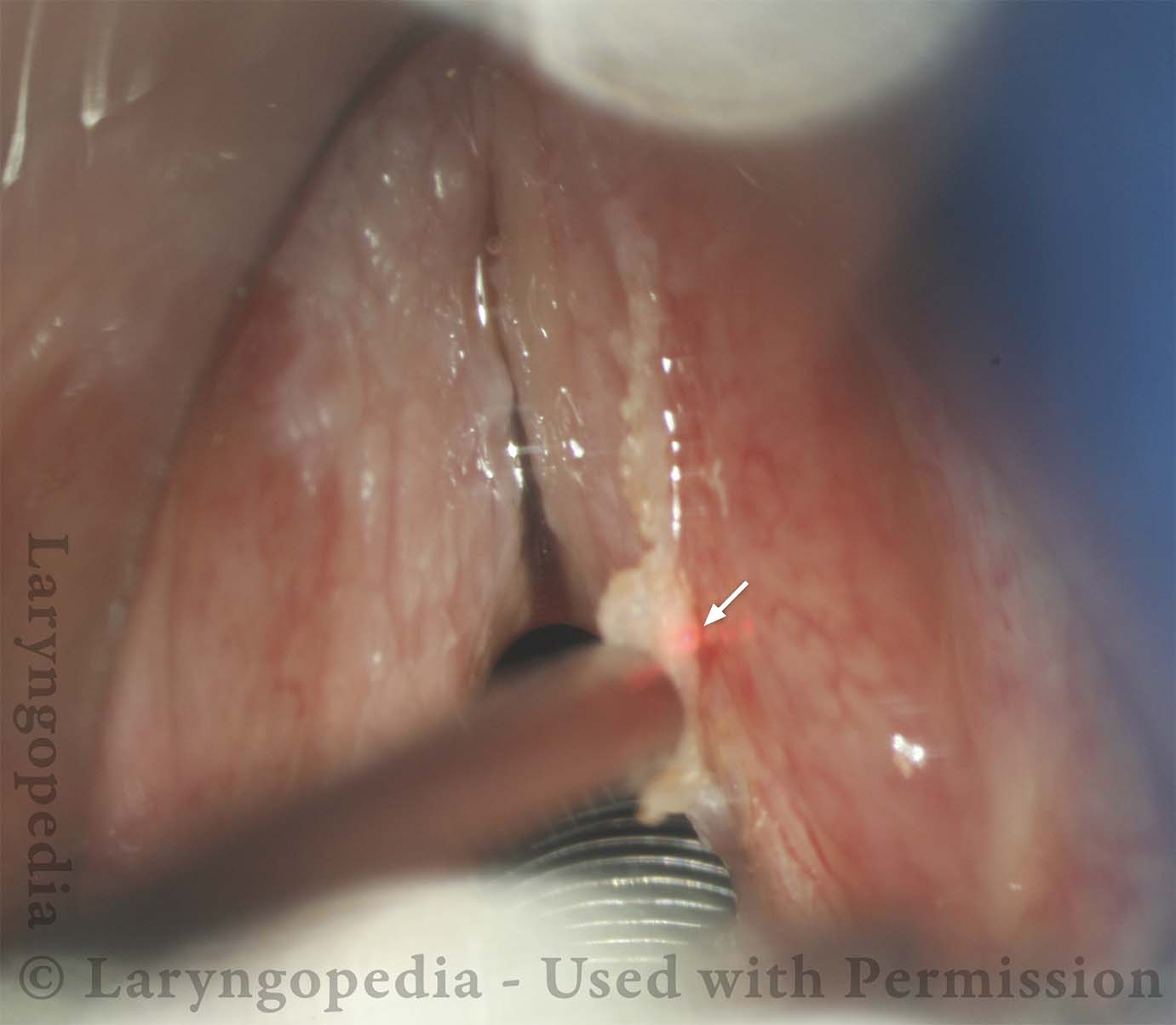
Fourteen months after photos 5 and 6. After roughly a dozen treatments spanning more than a decade, the voice sounds effortless and has no syllable dropouts. It is mildly husky but entirely satisfactory to the patient. Note how well-preserved and “unscarred” the superficial vascular pattern of the mucosa is (arrows), after so many surgical procedures.
Coagulated tissue (8 of 8)
At the conclusion of thulium coagulation of this linear patch of leukoplakia. Arrows show the line of coagulated tissue.

Thulium Laser Surgery, With Local Anesthetic Injection, to Treat Leukoplakia
Leukoplakia, about to be treated with laser (1 of 4)
Leukoplakia of the vocal cords in a patient radiated years earlier for glottic cancer. This disease is mostly benign, but foci of carcinoma-in-situ have also been removed twice in the operating room, yet with rapid return of leukoplakia. The patient has had no glottic voice. In an effort to avoid total laryngectomy, we are managing these visual abnormalities with the thulium laser in an outpatient videoendoscopy room.

Injection of local anesthetic (2 of 4)
Since this patient cannot tolerate aggressive laser therapy with topical anesthesia alone, we are here adding injection of local anesthetic. Note the blanching of tissue surrounding the needle.
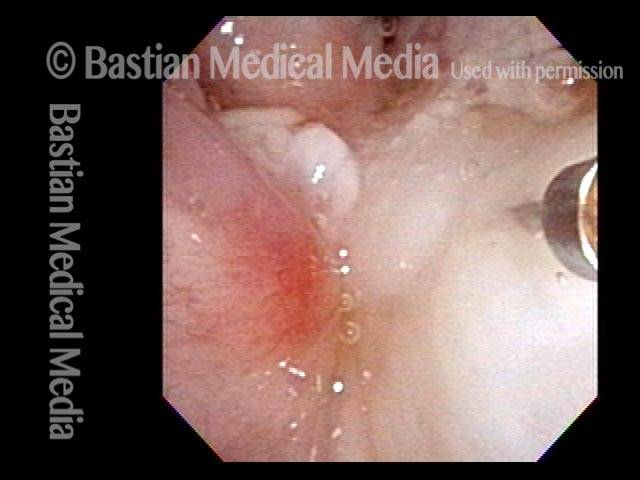
Injection of local anesthetic (3 of 4)
Further injection of the local anesthetic.
Right after thulium laser treatment (4 of 4)
At the completion of aggressive laser coagulation of abnormal tissue. Compare with photo 1. The patient will return in a month for additional laser treatment as indicated.

Leukoplakia, Before, During, and After Laser Coagulation
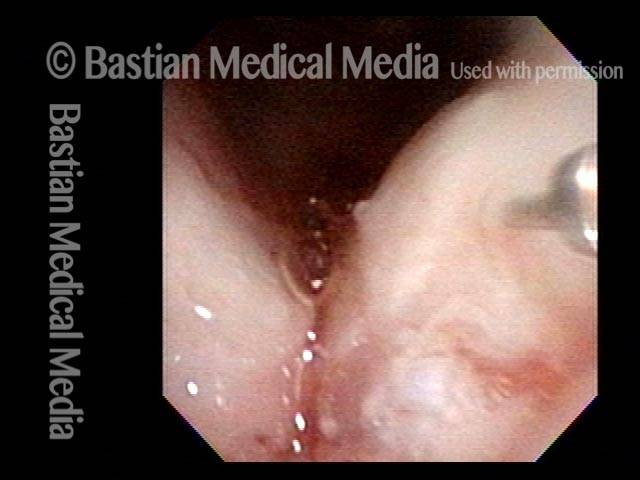
Leukoplakia, not yet seen (1 of 6)
A few years earlier, this patient underwent superficial laser cordectomy of the right vocal cord (left of photo) for cancer. The voice result is excellent, and the patient is being seen this day for a routine interval examination, and has no new complaints.
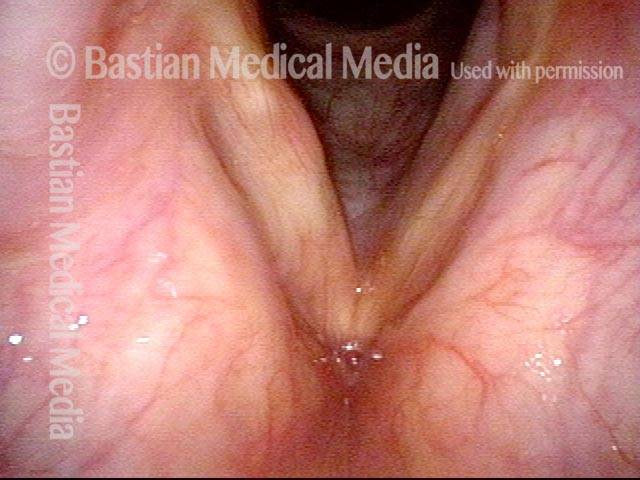
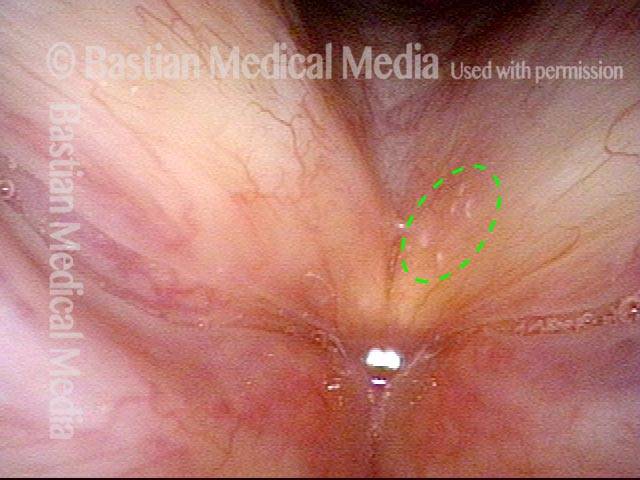
Leukoplakia (2 of 6)
At closer range, tiny points of leukoplakia (inside the green dotted oval) become evident. The bright white spot in the photo is just a light reflection.
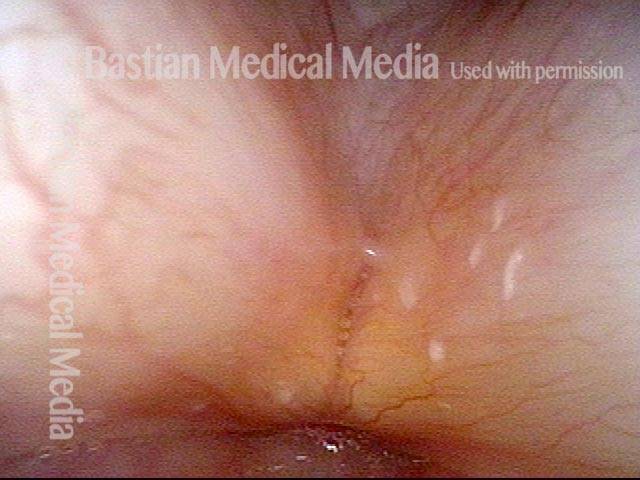
Leukoplakia (3 of 6)
Still closer view, again confirming the tiny patches of leukoplakia. There is another light reflection in this view, right in the middle of the photo.
Leukoplakia, coagulated by laser (4 of 6)
Thulium laser coagulation of the leukoplakia lesions, through a glass fiber (blue-ish cylinder at top-right of photo), as seen under narrow-band illumination. The Thulium laser had been placed on stand-by prior to the routine examination, to save the patient a potential second visit. The coagulated tissue is also white, but will slough off within a few days, and along with it, the leukoplakia.

Leukoplakia, 3 months after laser treatment (5 of 6)
Three months after laser treatment, the patient has healed.
Leukoplakia, 3 months after laser treatment (6 of 6)
Three months after laser treatment, a close up view shows no signs of leukoplakia spots.
Vocal Nodules, Leukoplakia, and Capillary Ectasia
Vocal nodules, leukoplakia, and capillary ectasia (1 of 4)
Abducted breathing position, standard light. Notice not only the margin swellings (nodules) but also the ectatic capillaries and the roughened leukoplakia. This person illustrates well the idea that vibratory injury can be manifested differently. Many express the injury more in the form of sub-epithelial edema and other changes; this person also has considerable epithelial change.
Vocal nodules, leukoplakia, and capillary ectasia (2 of 4)
Prephonatory instant, standard light.
Vocal nodules, leukoplakia, and capillary ectasia: 6 months later (3 of 4)
Partial resolution of mucosal injury as a result of behavioral changes directed by a speech pathologist. Strobe light, open phase of vibration.
Vocal nodules, leukoplakia, and capillary ectasia: 6 months later (4 of 4)
Strobe light, moving towards closed phase of vibration.
Glottic Furrow / Leukoplakia / Acid Reflux
Glottic furrow / Leukoplakia / Acid reflux (1 of 4)
Panoramic view, standard light. Note general inflammatory appearance, left vocal cord leukoplakia, interarytenoid pachyderma. Some would call this a sulcus.
Leukoplakia (2 of 4)
Furrow-like groove best seen on the left vocal cord (arrow). Beneath the arrow is the leukoplakia. Notice loss of fine surface vessels in this area.
Glottic furrows (3 of 4)
Furrows seen bilaterally.
Gap during closed phase (4 of 4)
Strobe light, closed phase. Note the slight gap; this is often seen as a kind of pseudo-bowing with furrow.

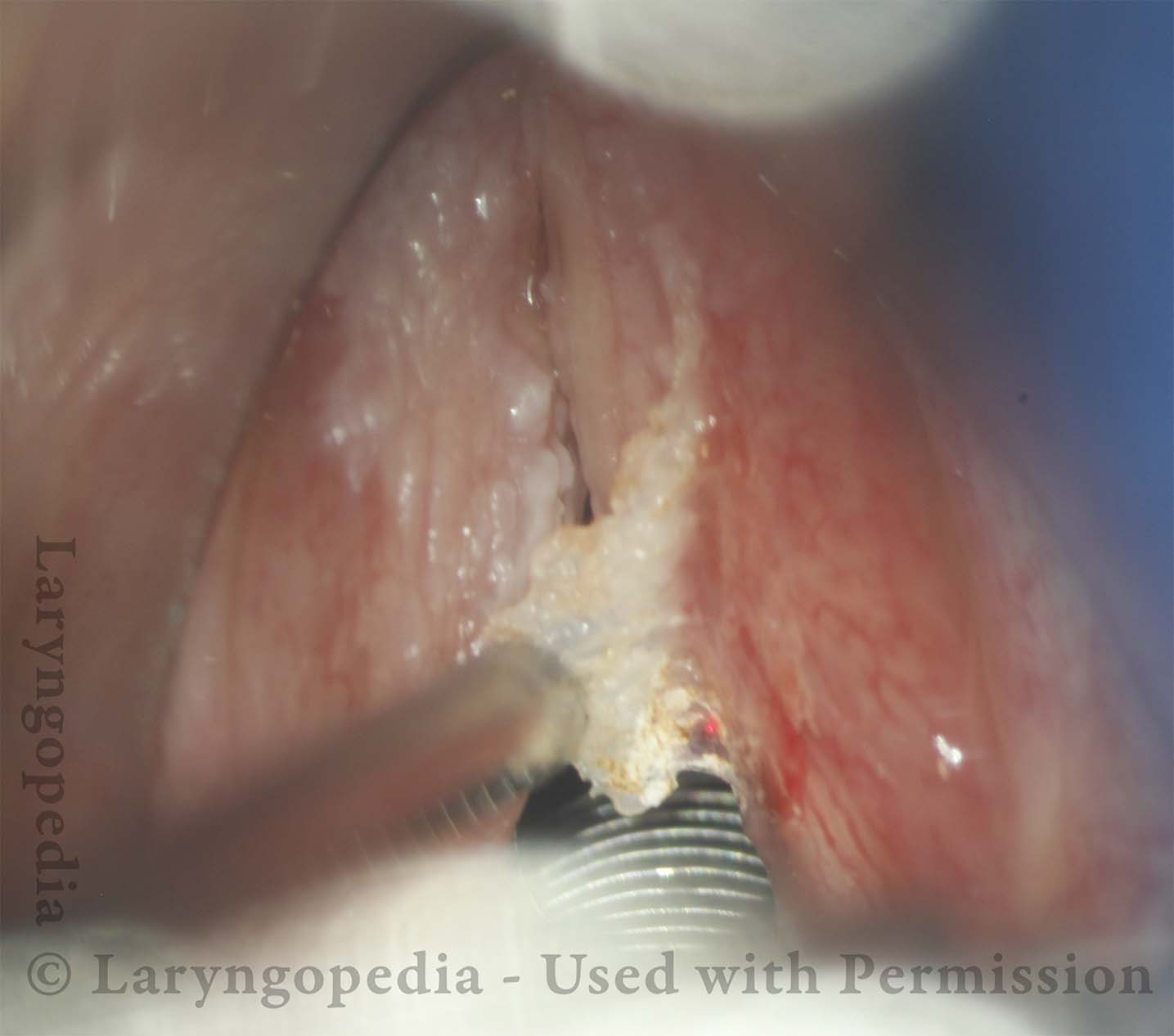
Leukoplakia Biopsy
HIV Testing (1 of 2)
2-millimeter forceps being used to scrape the area of leukoplakia to retrieve cells for HPV testing. In this case, it was negative.

Biopsy (2 of 2)
Cup forceps closed. Note that there is no biopsy, per se, but just scraping of the surface of the cords.

Narrow-band vs. Standard Light: Leukoplakia
Narrow-band vs. standard light: leukoplakia (1 of 2)

Narrow-band vs. standard light: leukoplakia (2 of 2)
