 Studio della deglutizione videoendoscopica (SDVS, VESS)
Studio della deglutizione videoendoscopica (SDVS, VESS)
Metodo per valutare la capacità di deglutizione di una persona mediante un esame fisico documentato tramite video, guardando dall’interno della gola. Chiamata anche valutazione endoscopica a fibre ottiche della deglutizione (FEES). Lo studio videoendoscopico della deglutizione (VESS in inglese) deve essere distinto dallo studio videofluoroscopico della deglutizione (VFSS), che è una valutazione basata sui raggi X.
 Come funziona un SDVS
Come funziona un SDVS
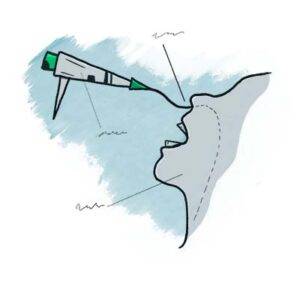
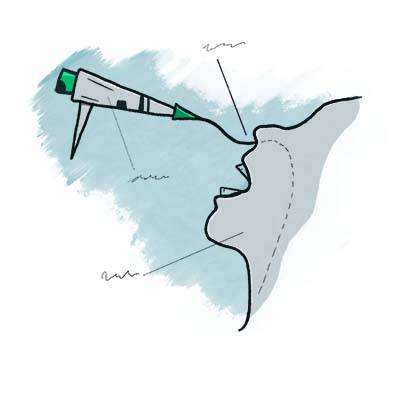
Per eseguire un VESS, un medico utilizza un nasolaringoscopio a fibra ottica o con chip distale. Il medico inizia esaminando la struttura e la funzione del palato, della lingua, della faringe e della laringe del paziente, compresa la sensibilità, se lo si desidera. Successivamente, per valutare le capacità e i limiti di deglutizione del paziente, il medico posiziona la punta del nasolaringoscopio appena sotto il rinofaringe e, guardando verso la gola, chiede al paziente di deglutire una serie di sostanze colorate con una gamma di consistenze (ad esempio, blu -acqua macchiata, salsa di mele macchiata di blu e cracker color arancione).
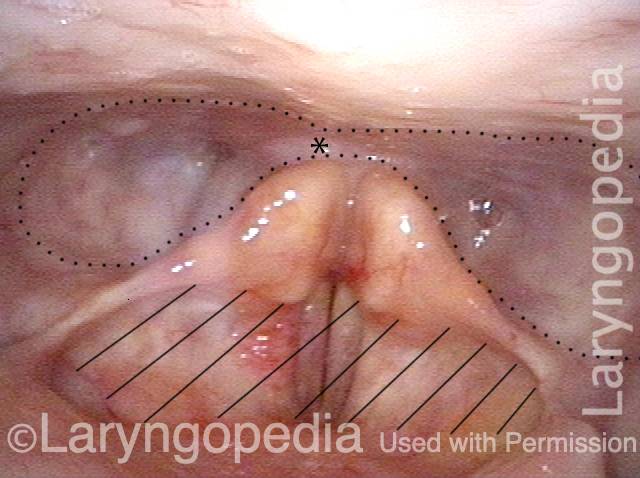
Mentre il paziente ingerisce queste sostanze, il medico osserva se rimangono o riappaiono tracce significative nello spazio sopra, intorno o all’interno della laringe, anziché scomparire nell’ingresso dell’esofago. Se rimangono tracce significative o se del materiale si riversa nell’apertura della laringe o nella trachea, il paziente può soffrire di presbifagia. Se inizialmente scompaiono tracce significative ma poi riemergono verso l’alto dall’ingresso esofageo, il paziente può avere una disfunzione cricofaringea, con o senza diverticolo di Zenker.
 Benefici dello studio della deglutizione videoendoscopica
Benefici dello studio della deglutizione videoendoscopica
This method has particular value for patients who are bedfast and cannot travel to the radiology suite, or for patients whose swallowing function is rapidly evolving (improving, usually), such as those recovering from a mild stroke. For clinicians experienced with this technique, VESS can also often be used with new patients complaining of dysphagia during the initial consultation as a robust and—depending on patient history—potentially stand-alone method of diagnosis and management.
Sometimes, the VESS findings, along with a patient history of solid food lodgment at the level of the cricoid cartilage or cricopharyngeus muscle, will indicate when VFSS should also be obtained to assess for possible cricopharyngeal dysfunction. Even in this latter circumstance, when VFSS is called upon to confirm a suspected diagnosis, VESS will have already oriented the examiner to the nature and severity of the problem. In most follow-up circumstances other than after cricopharyngeal myotomy, VESS is generally more efficient and inexpensive than VFSS.
SDVS valuta l’attrezzatura, le secrezioni e quindi la capacità di deglutizione
Part Ia: Palate elevates normally (1 of 7)
Part Ib: phonation (2 of 7)
Part Ic: High pitch elicited (3 of 7)
Part IIa: applesauce (4 of 7)
Part IIb: cracker (5 of 7)

Part IIb: continued (6 of 7)
Part IIc: water (7 of 7)
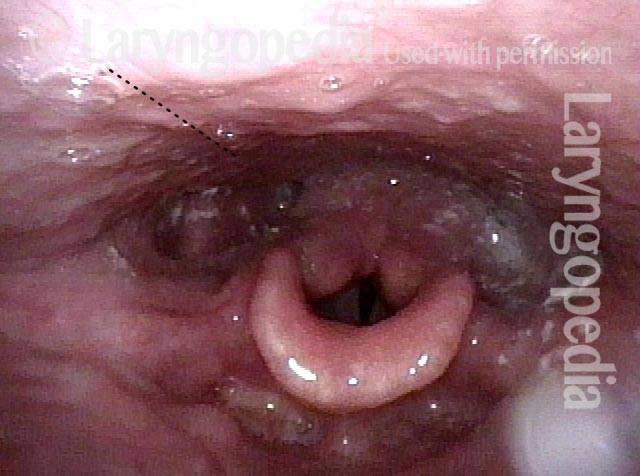
Disfagia/Riflesso ritardato della deglutizione
Laryngopharynx (1 of 3)
Dysphagia / Delayed swallow reflex (2 of 3)
Hypopharyngeal pooling (3 of 3)
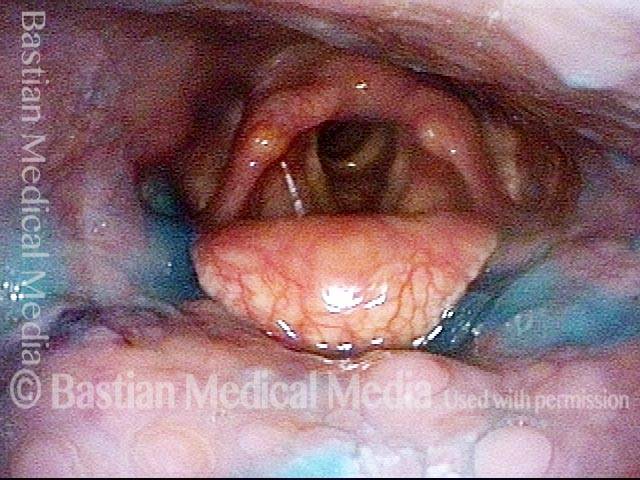
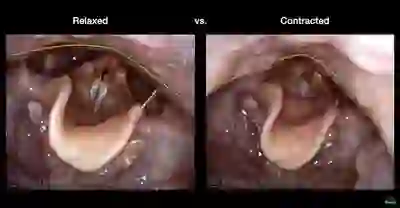
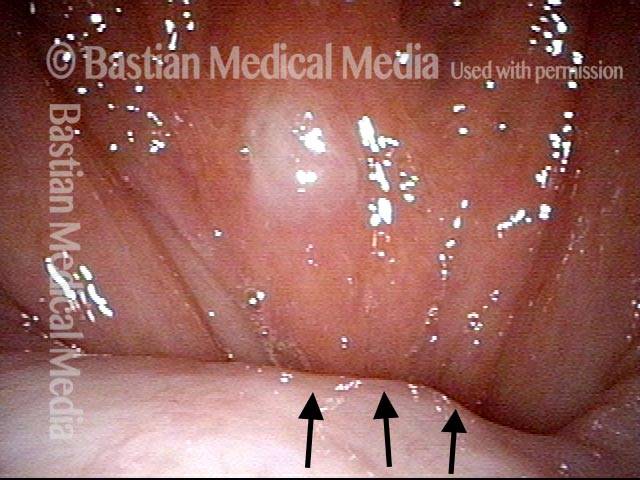
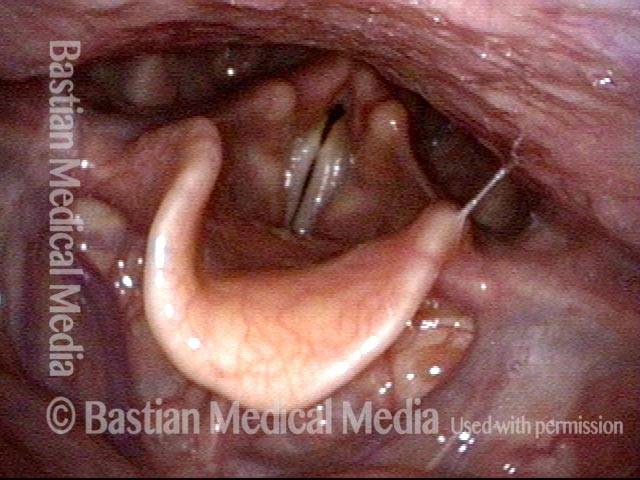
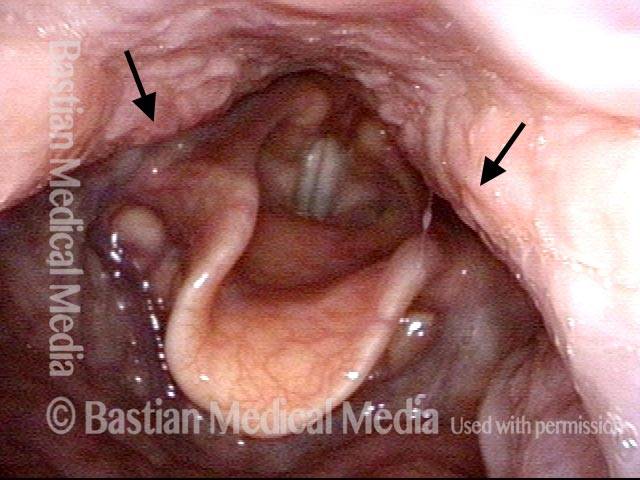
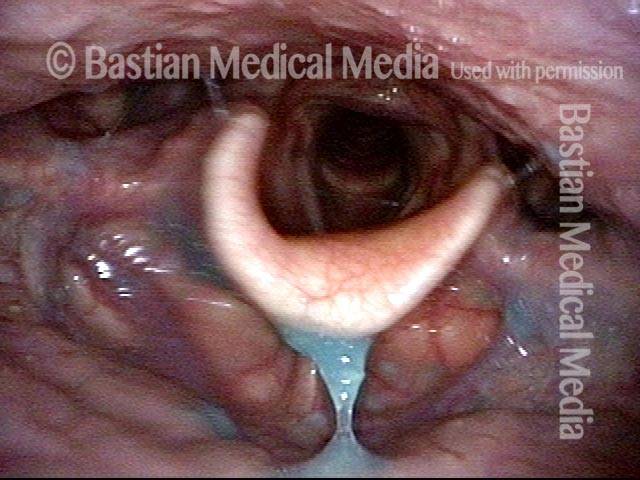
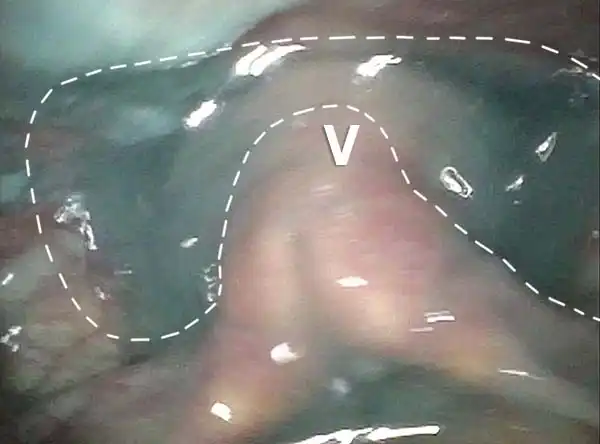
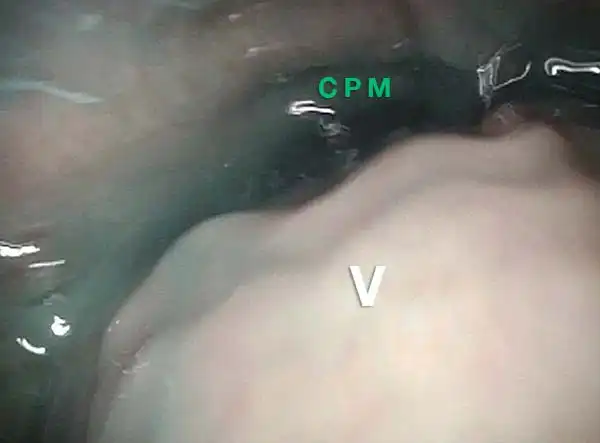
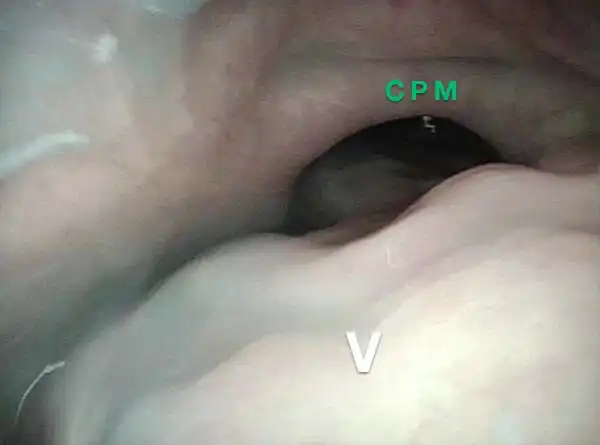
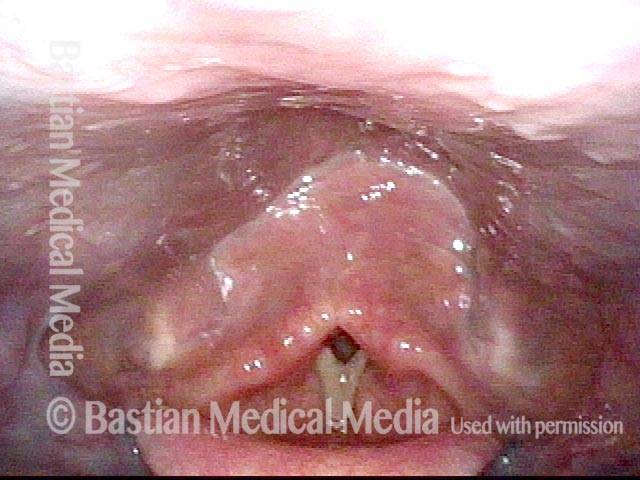
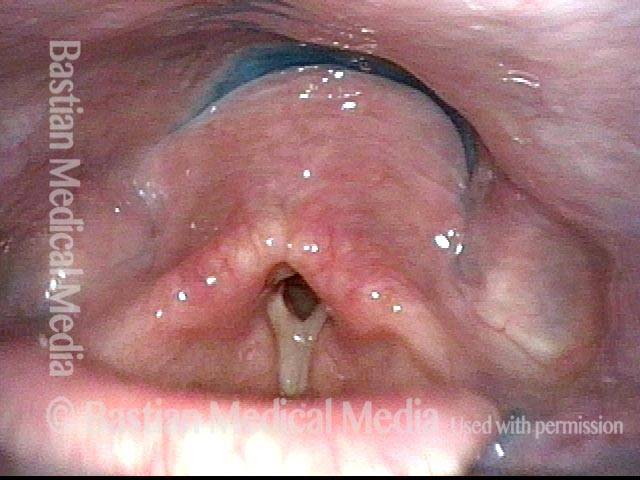
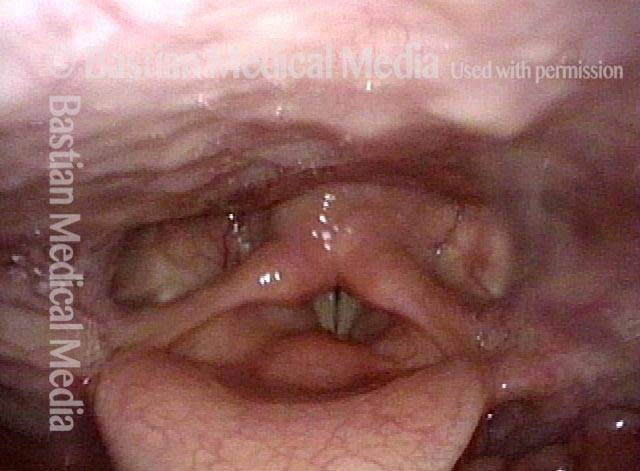
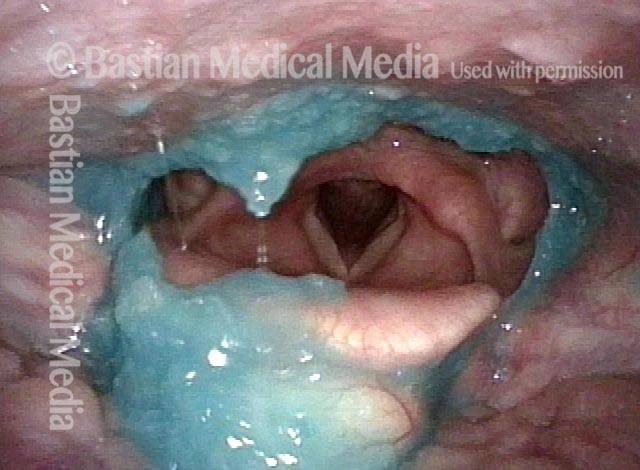
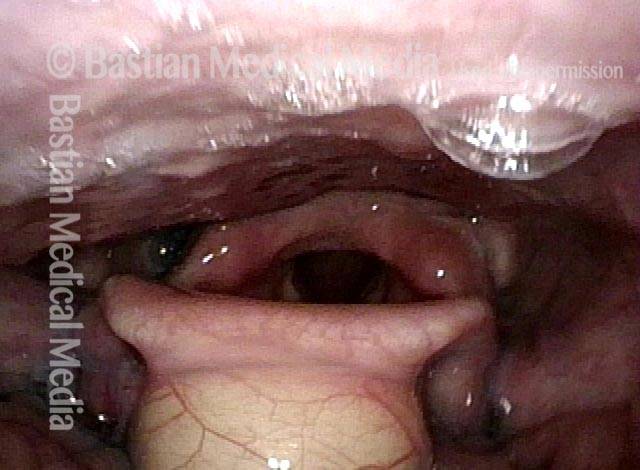
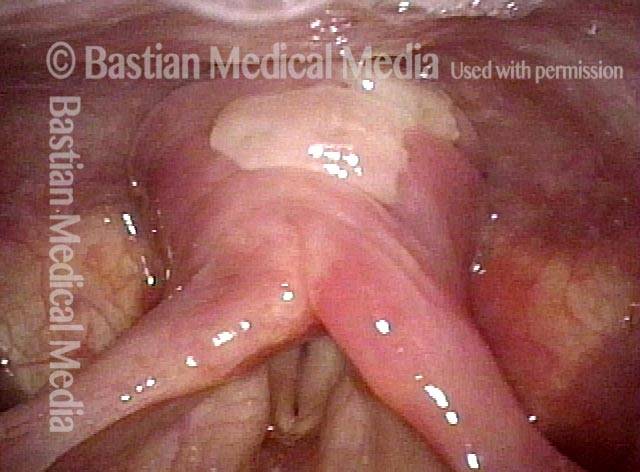
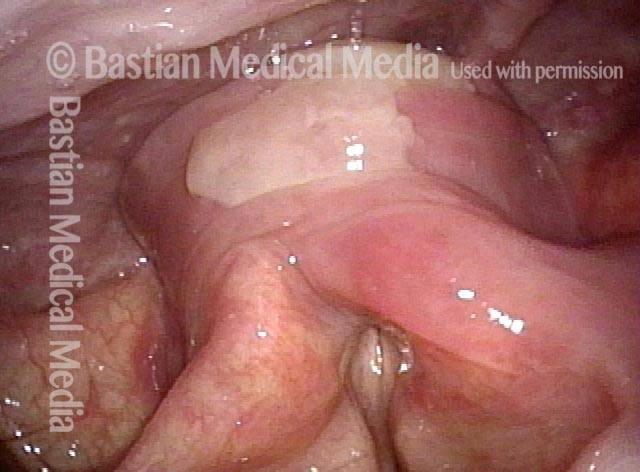
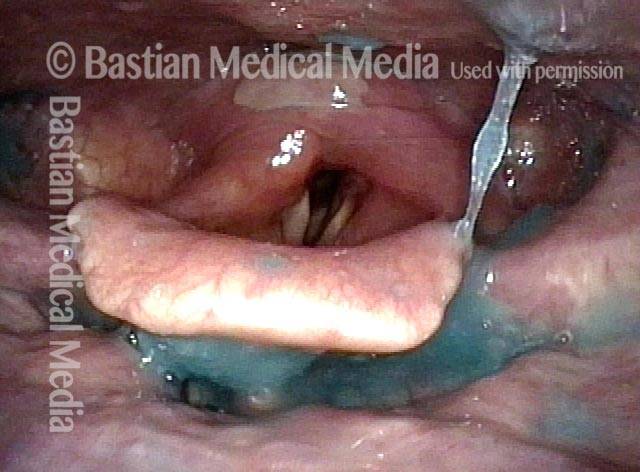
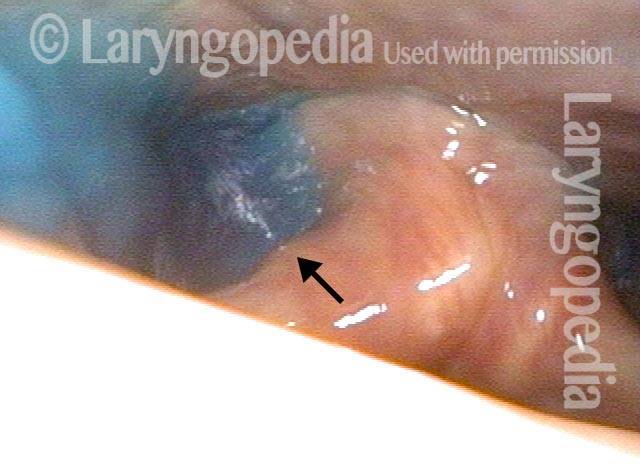
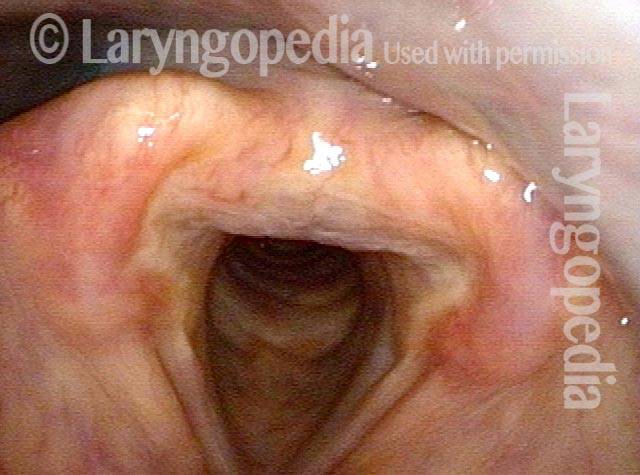
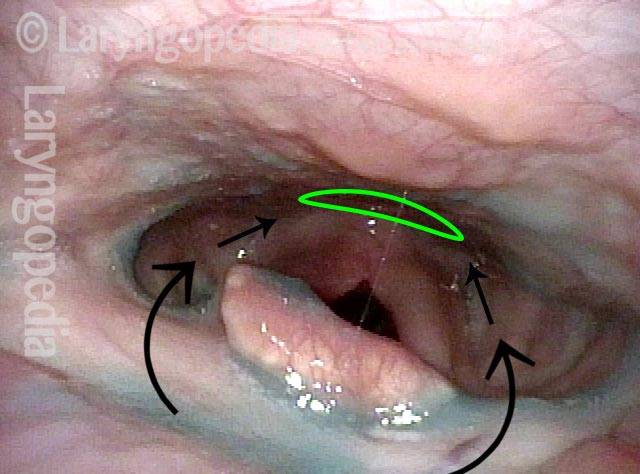
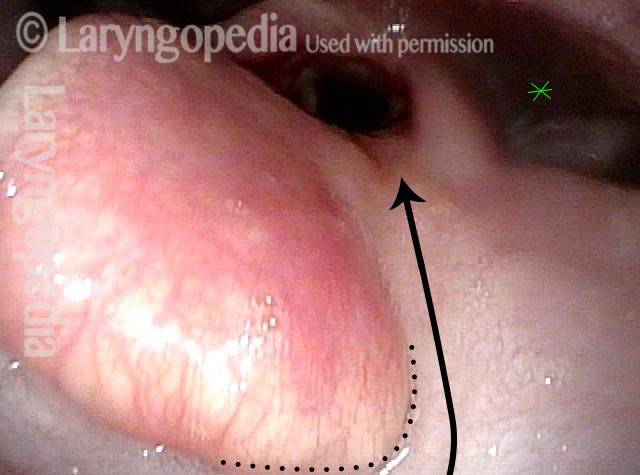
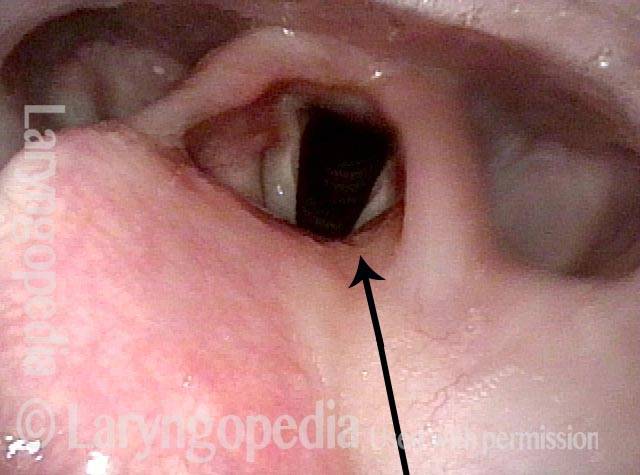
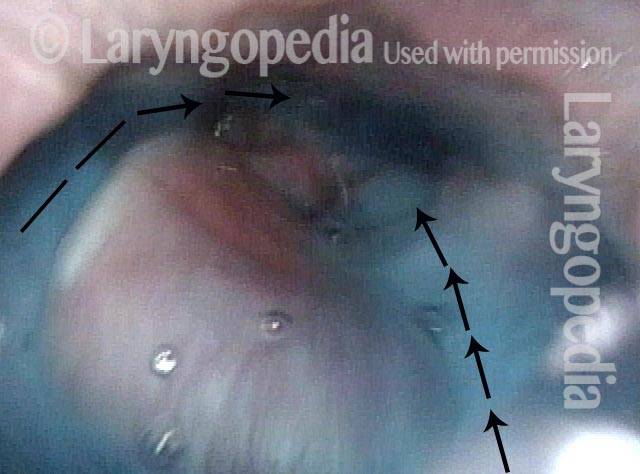
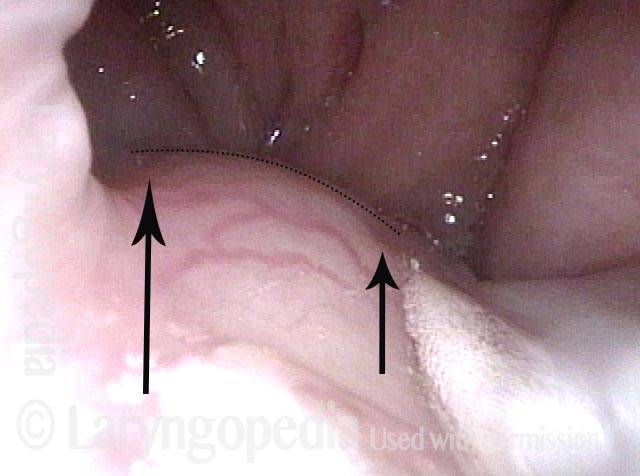
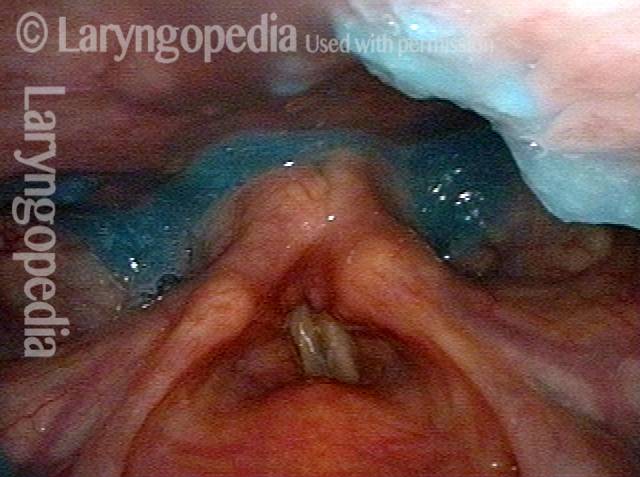
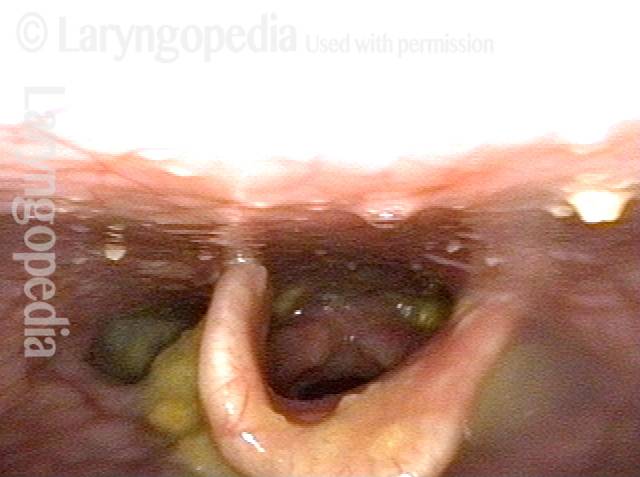
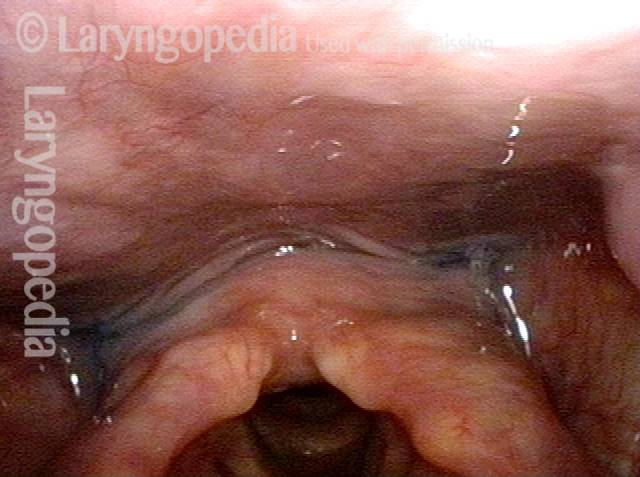
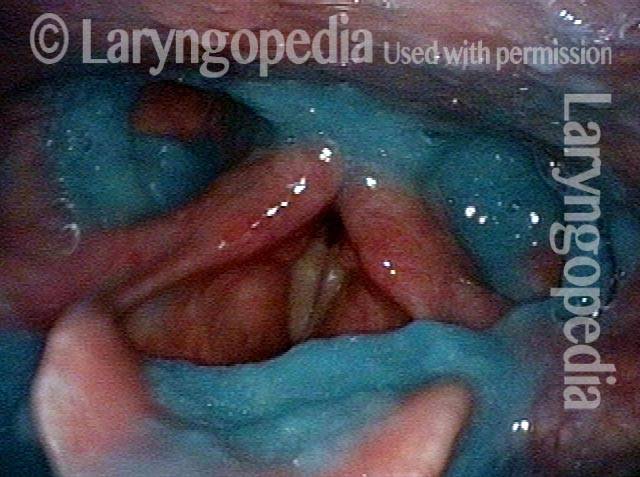
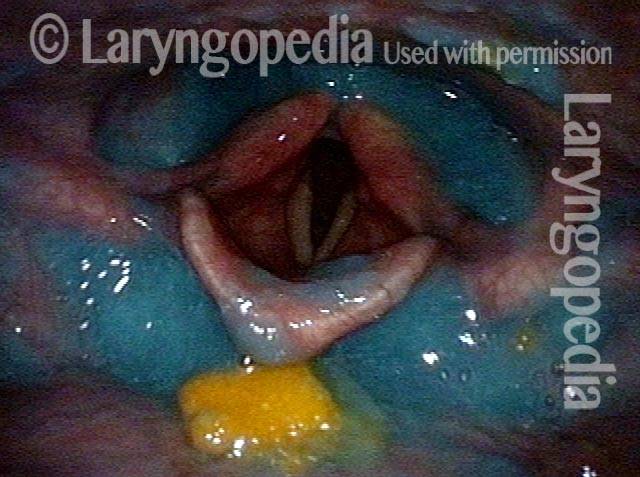
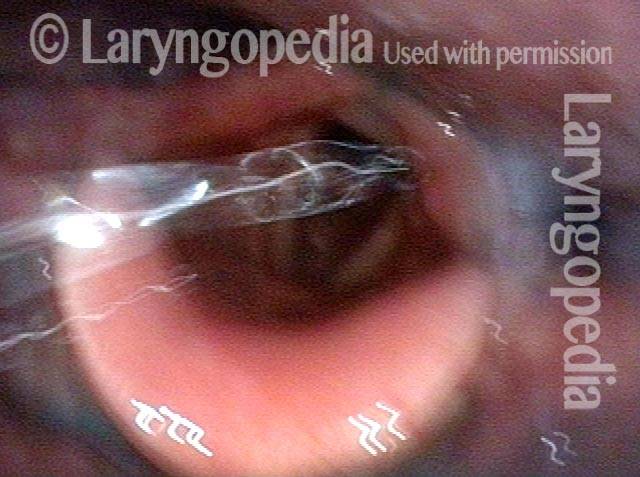
Il muscolo cricofaringeo visto durante la deglutizione
This person struggles to swallow due to a combination of prior tongue cancer surgery decades ago, and longterm radiation effects. Solid foods are the most problematic, and so this sequence shows an attempt to swallow water stained with blue food coloring.
Swallowing crescent (1 of 5)
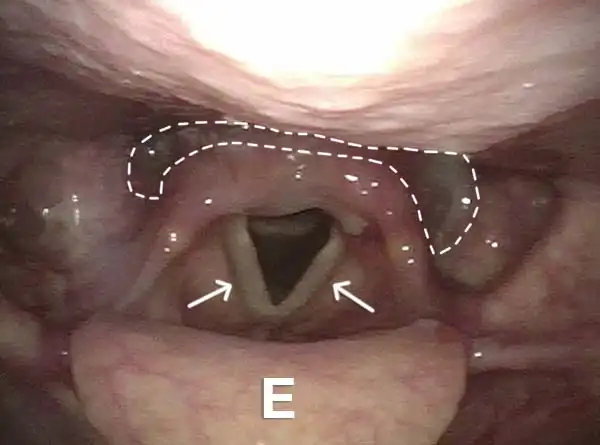
Swallowing water (2 of 5)
Cricopharyngeus muscle (3 of 5)
Relaxed CPM (4 of 5)

Partially open esophagus due to A-CPD (5 of 5)
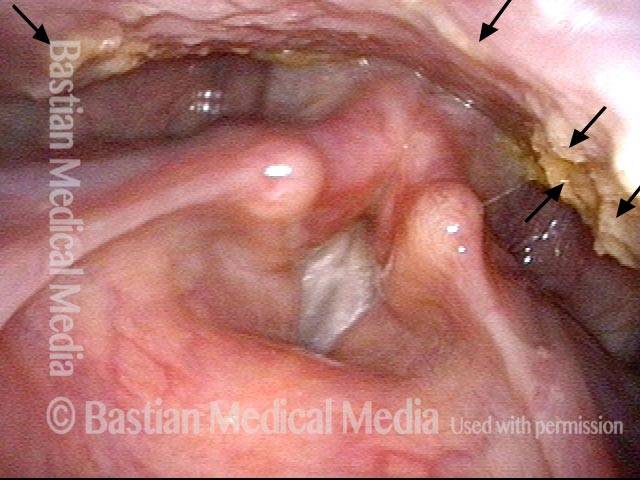
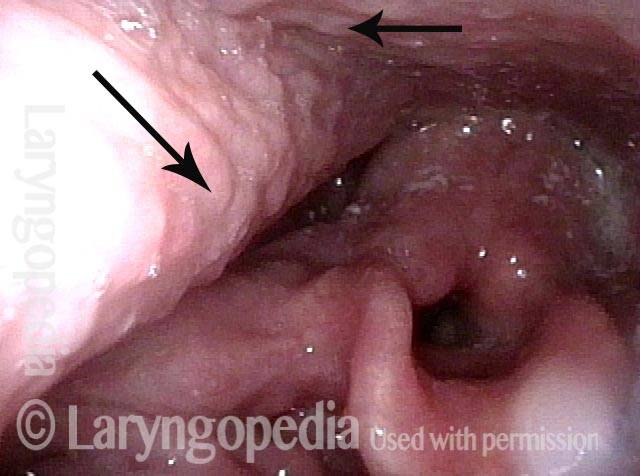
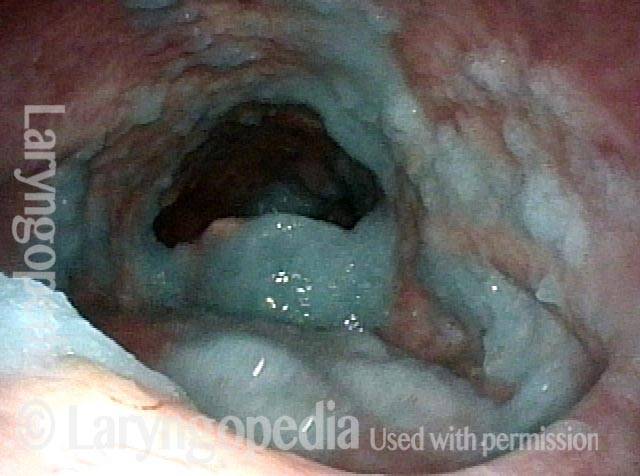
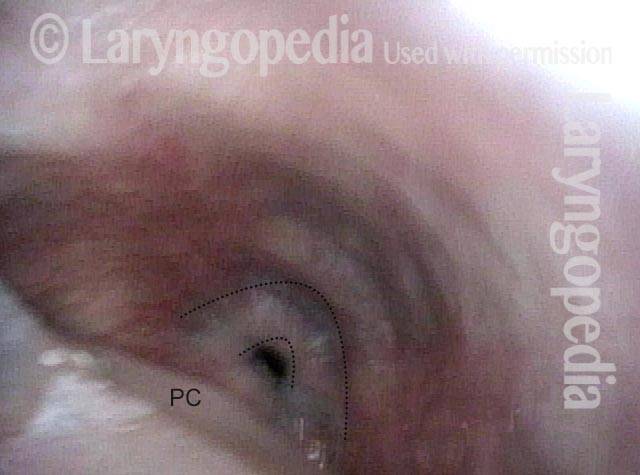
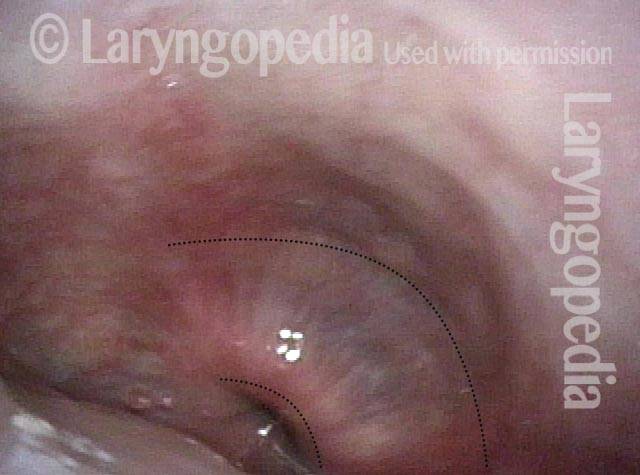
Diverticolo di Zenker
Zenker’s diverticulum (1 of 3)

Postcricoid area (2 of 3)

Hypopharynx (3 of 3)

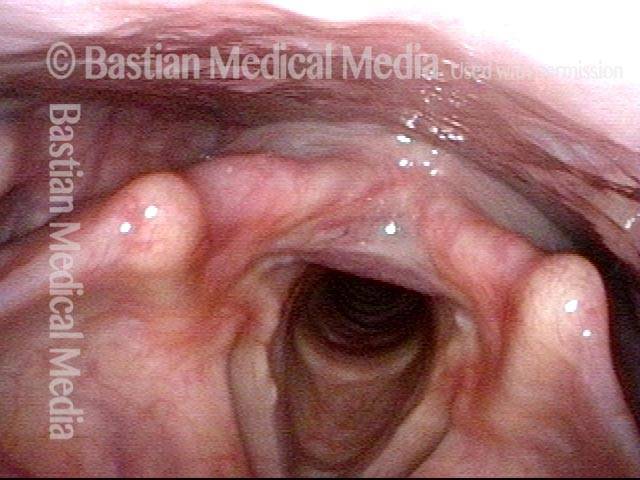
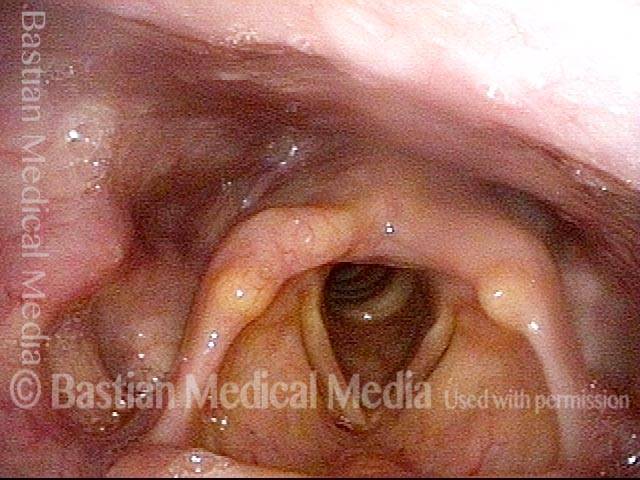
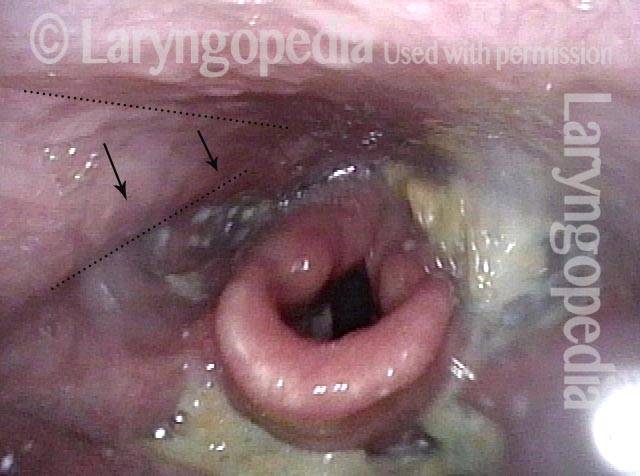
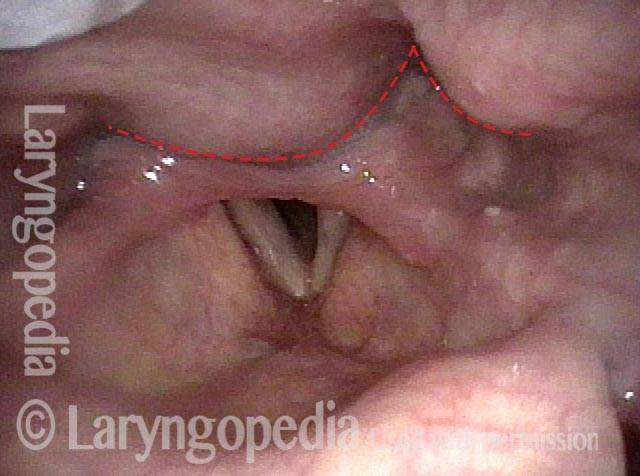
Reflusso nell’ipofaringe, caratteristico della disfunzione cricofaringea
Reflux into hypopharynx (1 of 3)
Water flows into the swallowing crescent (2 of 3)
Larynx opens up (3 of 3)

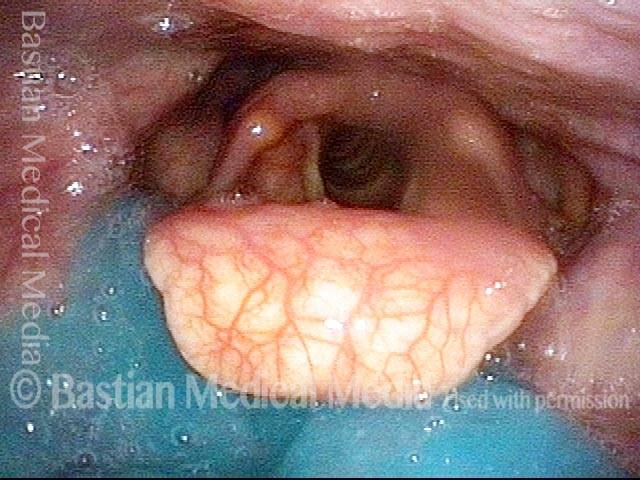
Le cisti vallecolari non disturbano la deglutizione, tranne quando lo fanno
Vallecular cyst (1 of 4)
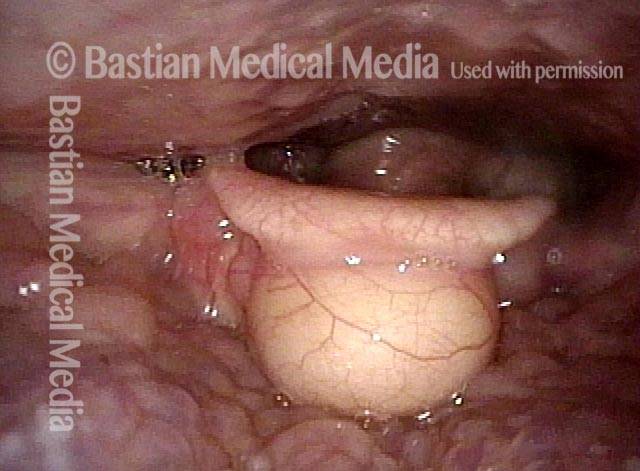
Evaluation of function (2 of 4)
Applesauce residue (3 of 4)
Water wash (4 of 4)
Alloggiamento della pillola a causa di difficoltà di deglutizione
Lodged pill (1 of 4)
Trumpet maneuver (2 of 4)
VESS (3 of 4)
Incomplete relaxation of CPD (4 of 4)

Riflesso ritardato della deglutizione: confronta la salsa di mele blu e l’acqua blu
VESS (1 of 4)

Delayed swallow reflex (2 of 4)

Blue-stained water (3 of 4)
No residue (4 of 4)
Scarring Diverts Swallowed Materials Directly into the Larynx
Post tonsillectomy (1 of 4)
Closer view (2 of 4)
The “chute” (3 of 4)
Abnormal diversion (4 of 4)
Frattura della base cranica e lesione del nervo vago: notare la contrazione della faringe e l’impatto sulla deglutizione
Palate branch of the vagus nerve (1 of 4)
Pharynx branch of the vagus nerve (2 of 4)
Damage to left vagal nerve function (3 of 4)
Residue during swallowing test (4 of 4)
SDVS in 6 foto
Assessing the patient’s swallowing (1 of 6)

Observing the pharynx (2 of 6)

Patient secretions (3 of 6)

Pooling of swallowed pureed food (4 of 6)
Swallowing solids (5 of 6)
Residue after foods (6 of 6)
Risultati SVDS dopo la radioterapia
Narrowed pharyngeal wall (1 of 7)

Swallowing applesauce (2 of 7)
After sipping water (3 of 7)

Gravity aiding in swallowing (4 of 7)

Lifting larynx (5 of 7)
A closer look (6 of 7)
Gravity aiding again in swallowing (7 of 7)
Gli osteofiti cervicali non sembrano di per sé un grave ostacolo alla deglutizione
Protruding osteophytes (1 of 2)
Rapid swallowing (2 of 2)

Aspirazione e fontana dell’aspirazione restituita dopo la tosse
Salivary pooling (1 of 5)

After applesauce (2 of 5)
After cheese cracker (3 of 5)
After water (4 of 5)
Cough expels the water from airway (5 of 5)

Tre viste dell’ingresso dell’esofago da lontano a da vicino
Swallowing Crescent (1 of 3)
Closed esophagus (2 of 3)
Open Esophagus (3 of 3)