
Office Laser, Even Occasionally for Singers
Ordinarily, vocal cord microsurgery is only for otherwise irreversible lesions. This is especially so in singers, even though when done well, such surgery is extremely safe and voice restoring. And if time and therapy approaches fail to resolve a lesion, the typical venue for surgery is in the operating room under brief general anesthesia, with use of an operating microscope and tiny instruments.
Still, there is an office option that can occasionally be considered. Capillary ectasia without a nodule or polyp, for example, can be well managed in the videoendoscopy procedure room using only topical anesthesia. And there are circumstances (medical issues, jaw anatomy, etc.) that cause a specific singer to prefer office-based laser surgery with pulsed-KTP, thulium, or “blue” laser.
Right Vocal Cord Polyp (1 of 8)
Polyp interferes with voice (2 of 8)

Laser surgery in singer (3 of 8)

Coagulated polyp (4 of 8)

Coagulated polyp (5 of 8)
Voice fully restored (6 of 8)

Margins match during phonation (7 of 8)

Equal vibration (8 of 8)

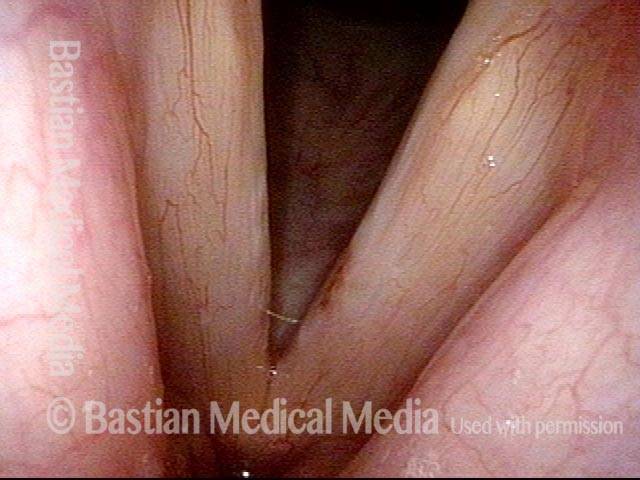
Vocal Polyp, Removed and then Recurring
Vocal polyp (1 of 4)
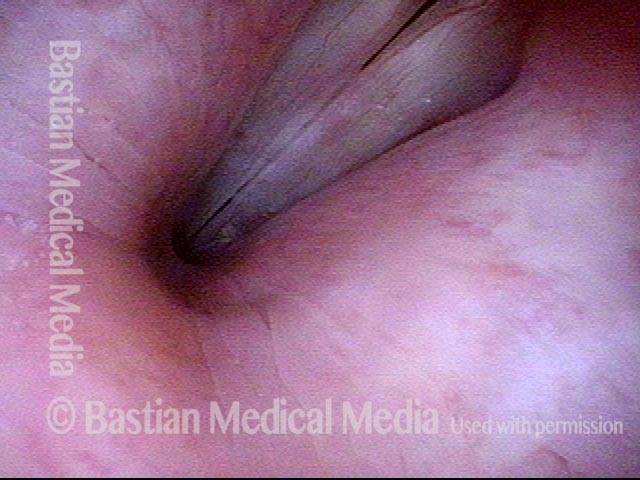
Vocal polyp (2 of 4)
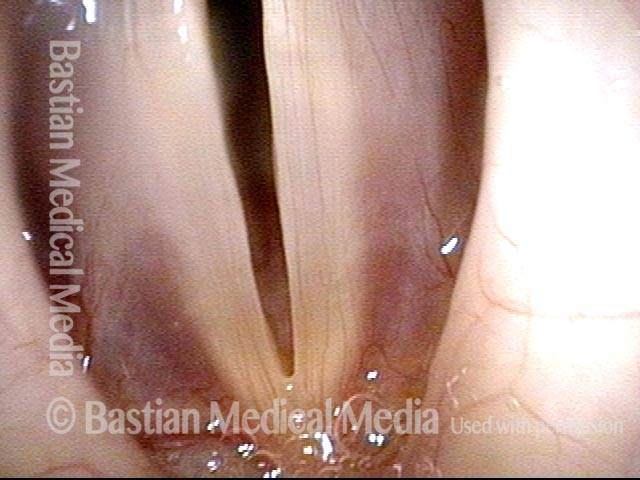
Vocal polyp, one week after surgical removal (3 of 4)

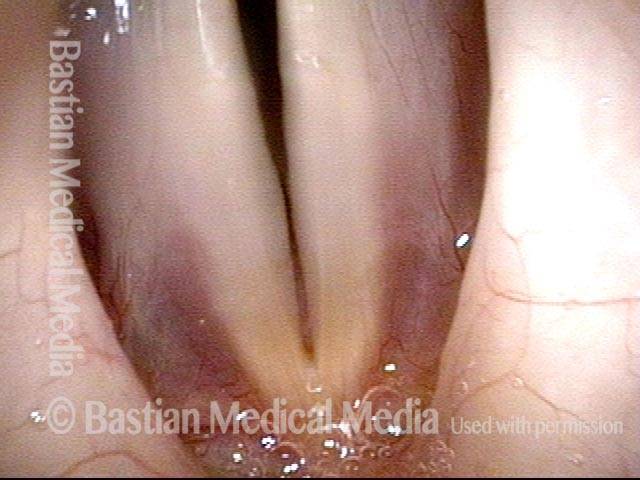
Vocal polyp, subsequent new injury (4 of 4)
Vocal Polyp, Before and After Surgery
Vocal polyp (1 of 6)
Vocal polyp (2 of 6)
Vocal polyp (3 of 6)
Vocal polyp, surgically removed (4 of 6)
Vocal polyp, surgically removed (5 of 6)

Vocal polyp, surgically removed (6 of 6)
Example 2
Vocal polyp (1 of 2)

Vocal polyp, surgically removed (2 of 2)

Example 3
Vocal polyp (1 of 6)

Vocal polyp (2 of 6)

Vocal polyp, surgically removed (3 of 6)
Vocal polyp, surgically removed (4 of 6)
Vocal polyp, surgically removed (5 of 6)
Vocal polyp, surgically removed (6 of 6)
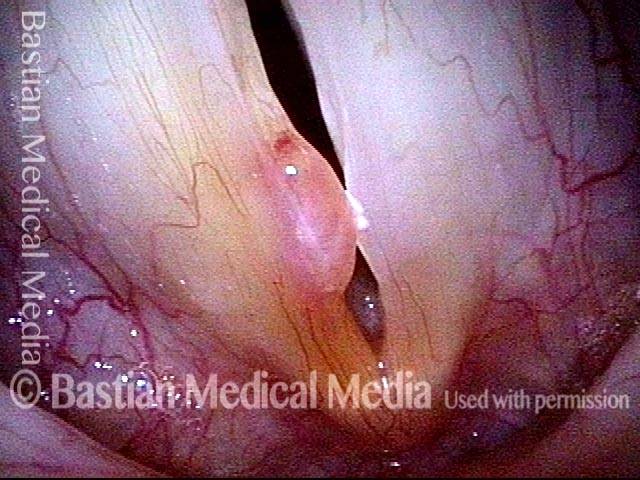
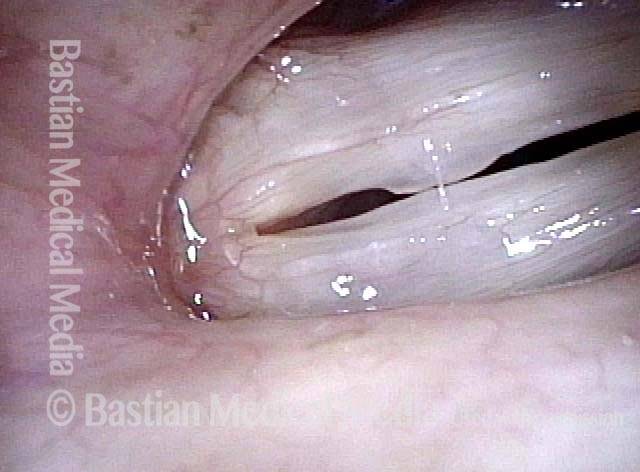
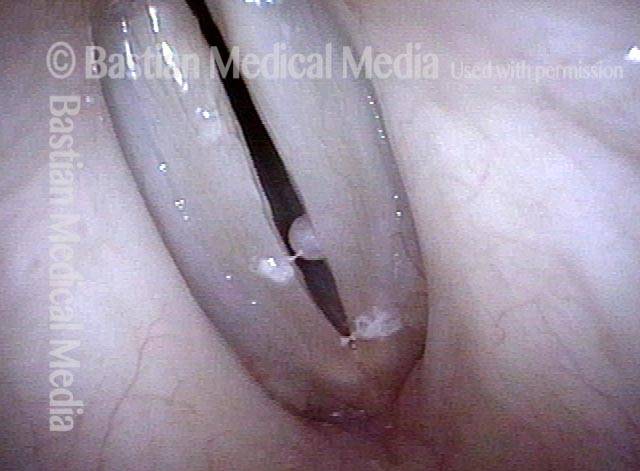
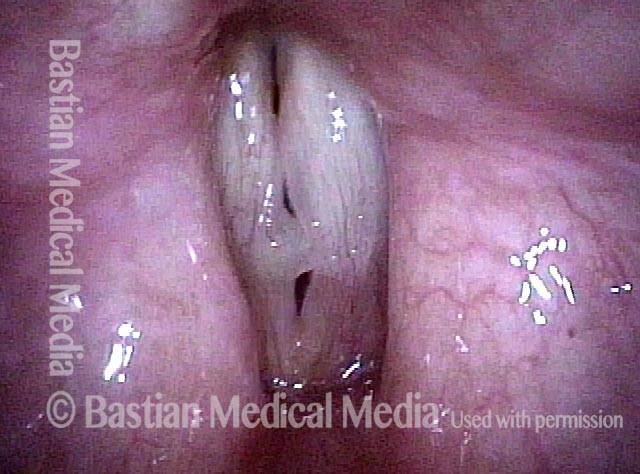
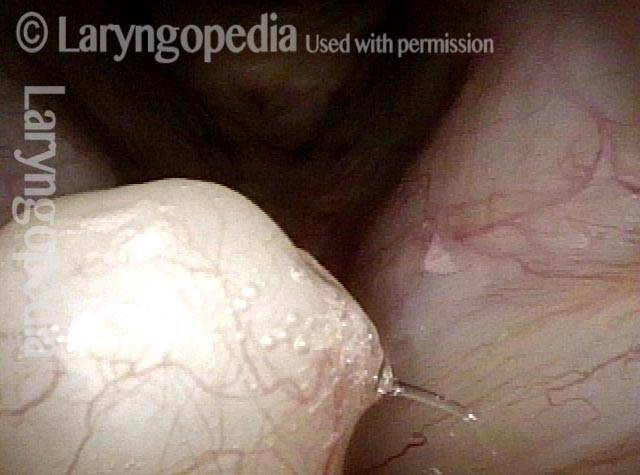
Translucent Polyp
Translucent polyp (1 of 4)

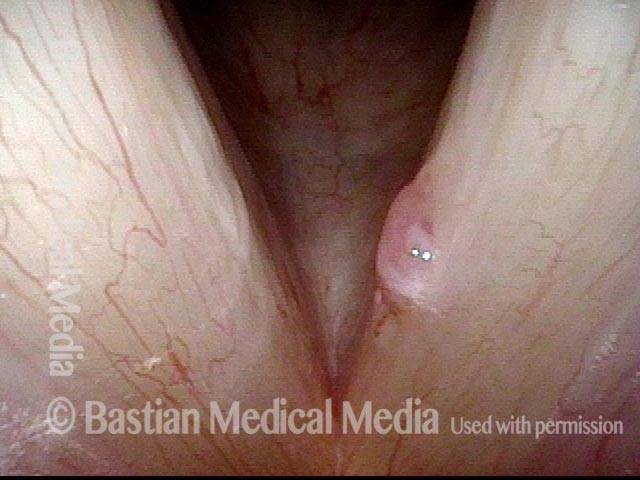
Translucent polyp (2 of 4)
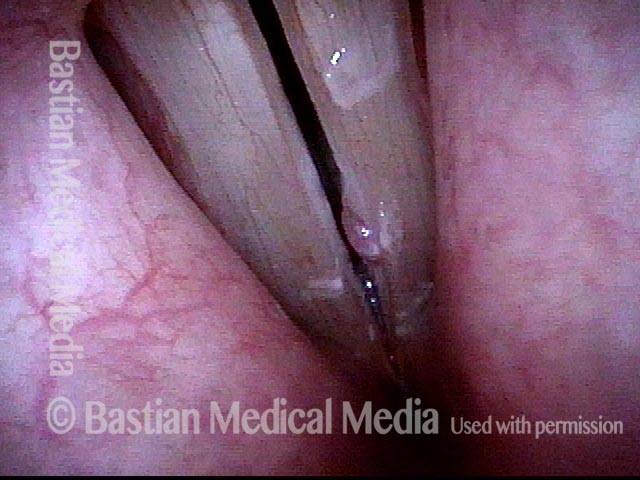
Translucent polyp (3 of 4)
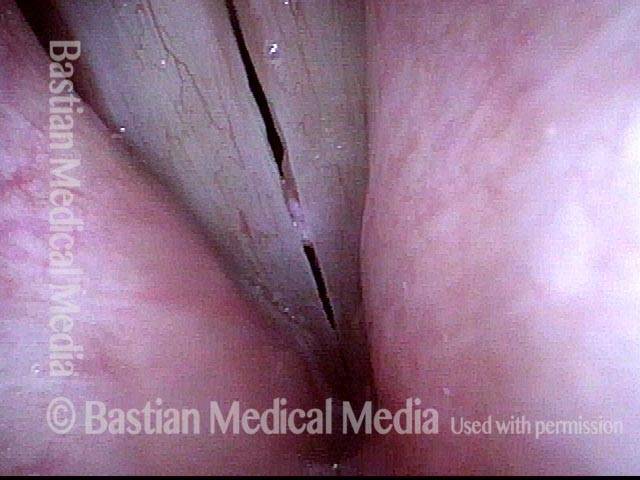
Translucent polyp (4 of 4)
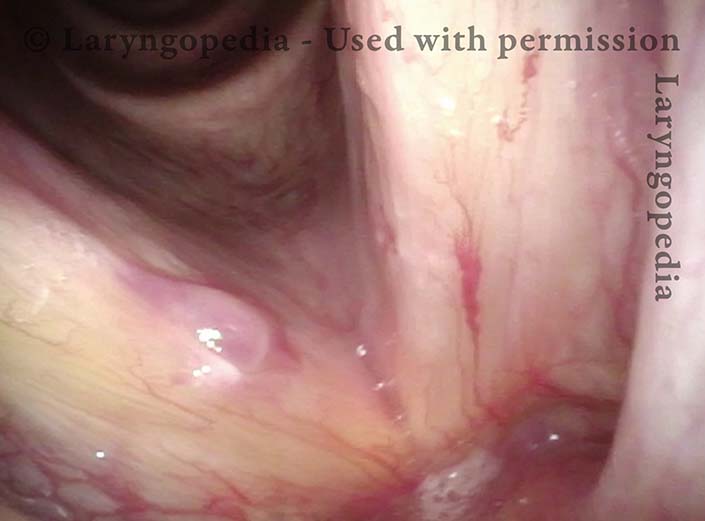
Opera Singer’s Polyp Removed with Restoration of Original Capabilities
Polyp and capillary ectasia (1 of 8)
Prephonatory instant (2 of 8)

One week post-op (3 of 8)
Prephonatory instant (4 of 8)

One month post-op (5 of 8)
Prephonatory instant (6 of 8)
Closed phase (7 of 8)

Open phase (8 of 8)
An Actress’ Polyp Before and Hours After Surgical Removal
Vocal cord polyp (1 of 8)
Closer view (2 of 8)

Closed phase (3 of 8)
Open phase (4 of 8)
24 hours post surgery (5 of 8)

Primary “wound” (6 of 8)
Closed phase (7 of 8)

Open phase (8 of 8)

Operated Cord Looks Better than the Unoperated Cord
Singer with chronic hoarseness (1 of 4)
Attempting phonation (2 of 4)
One week post surgical removal (3 of 4)
Open phase (4 of 4)
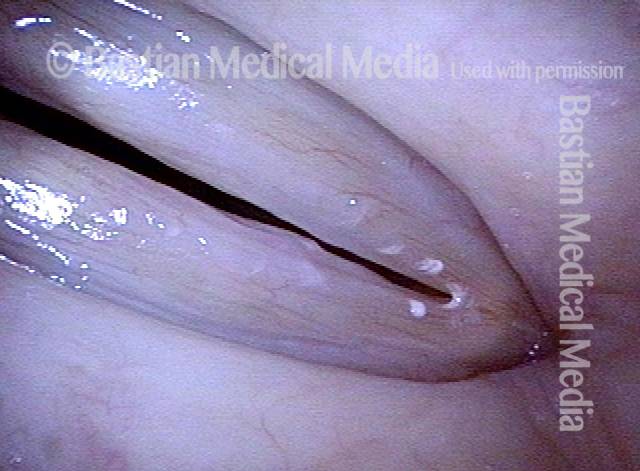
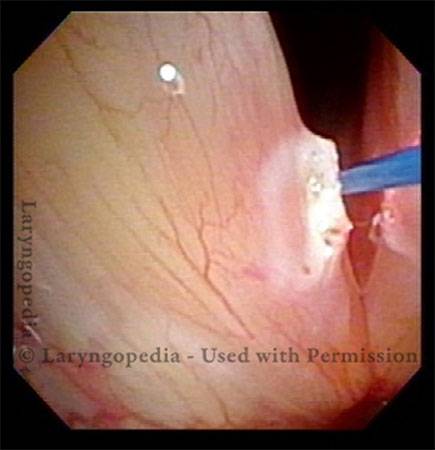
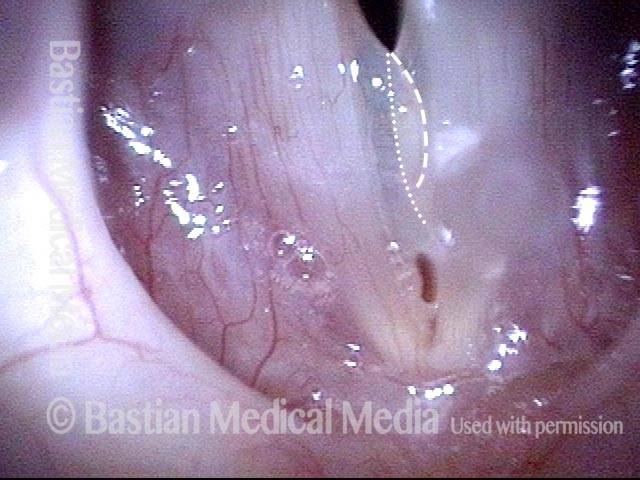
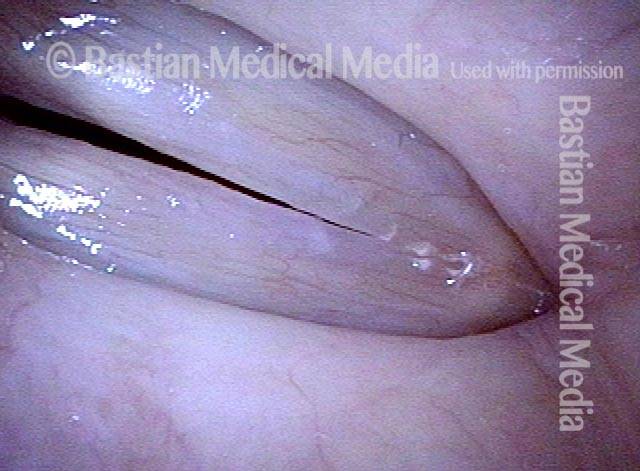
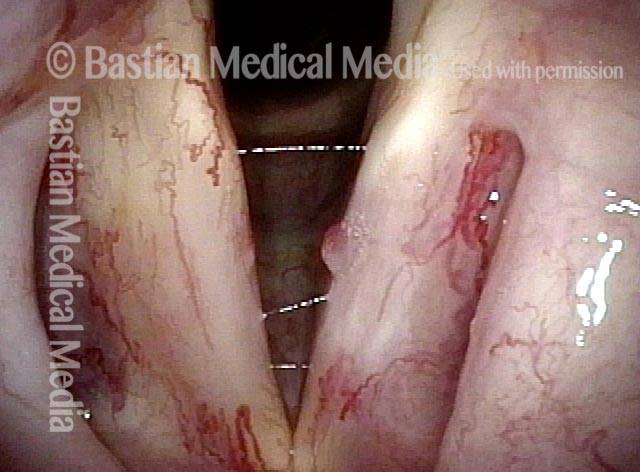
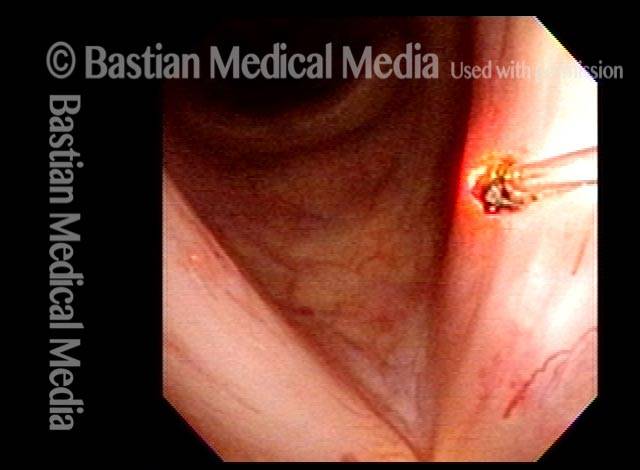
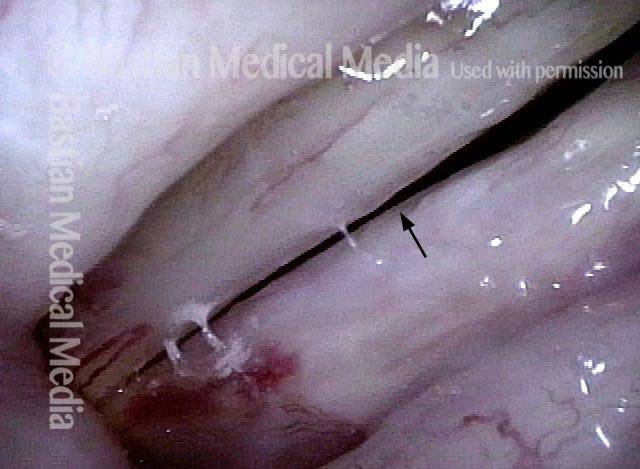
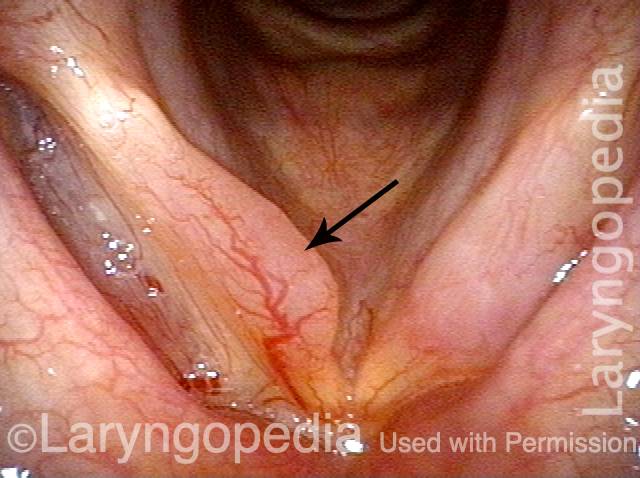
Office Laser of Post-radiation Telangiectatic Polyp
Post-radiation telangiectasias (1 of 4)
Pulsed-KTP coagulation (2 of 4)
“Polyp” pulled off (3 of 4)

Three weeks later (4 of 4)
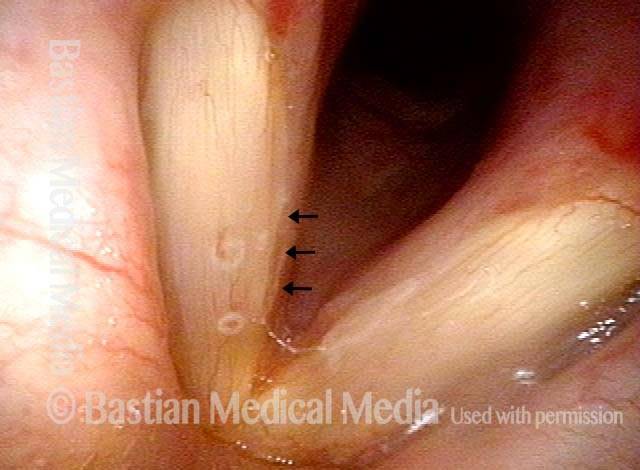
Nuances “Gleaned” from Daily Examinations
Vocal “overdoer” (1 of 4)
Inspiratory phonation (2 of 4)
Translucent polyp (3 of 4)

Open phase (4 of 4)

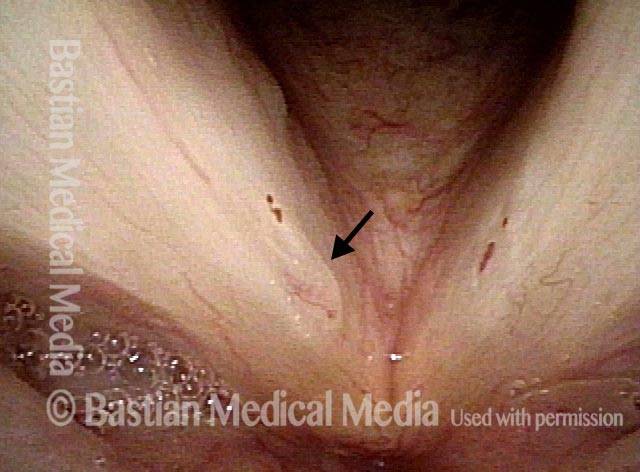
The Mucosa’s Expression of Injury Varies
Vocal cord injuries (1 of 4)

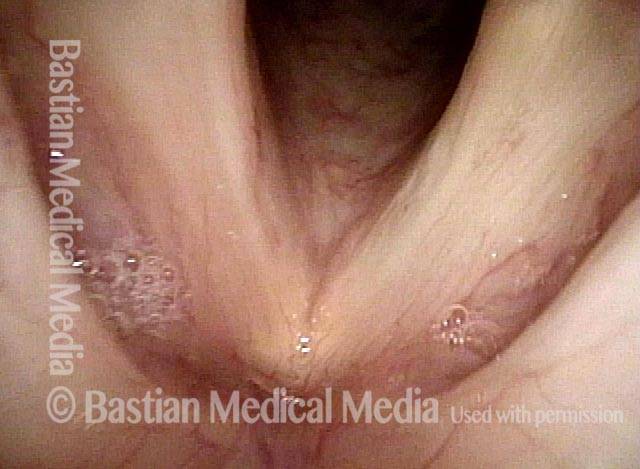
Narrow band lighting (2 of 4)

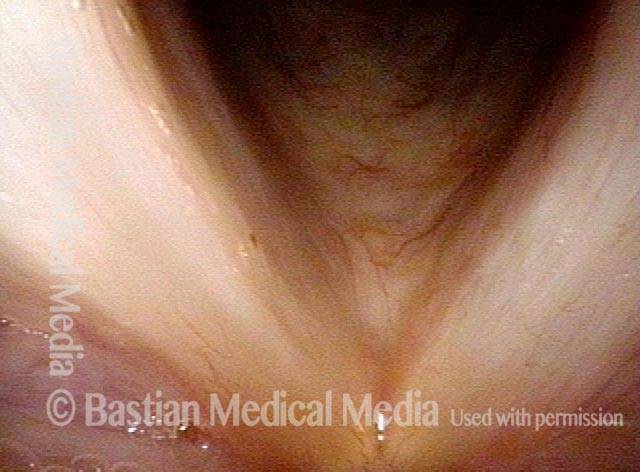
Strobe lighting (3 of 4)
Phonation (4 of 4)
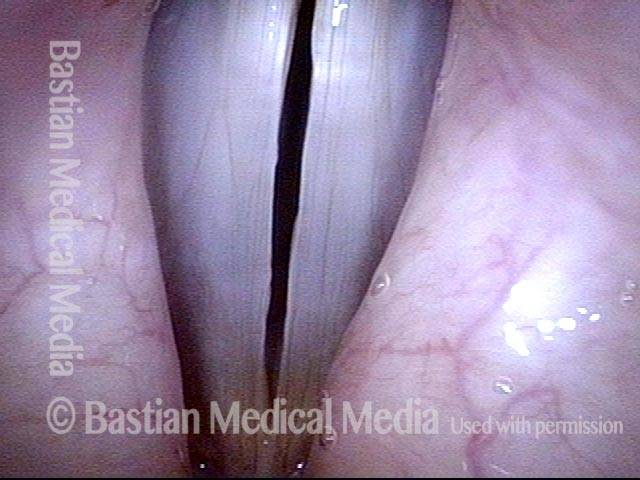
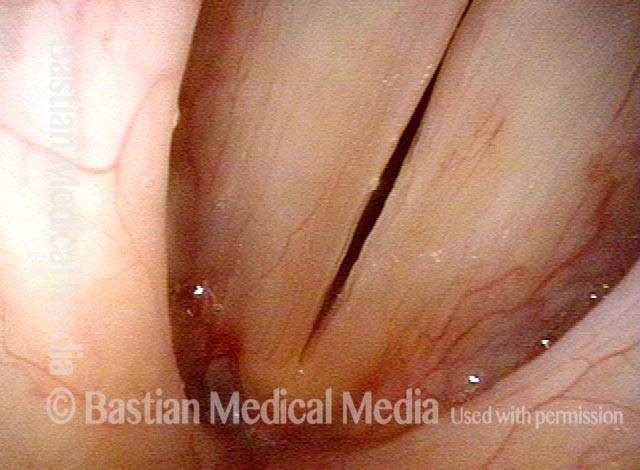
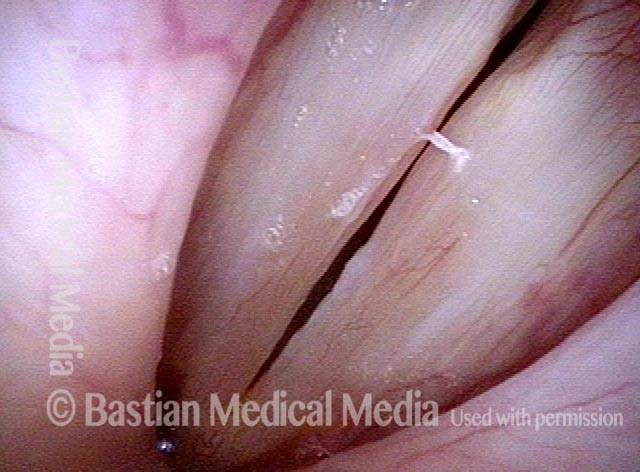
The Power of “Close-clear” Not “Far-fuzzy” to See a Polyp
Disant view (1 of 4)
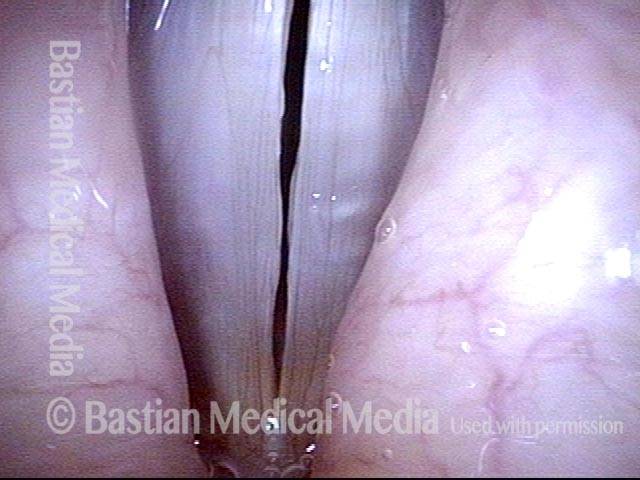
Closer view (2 of 4)
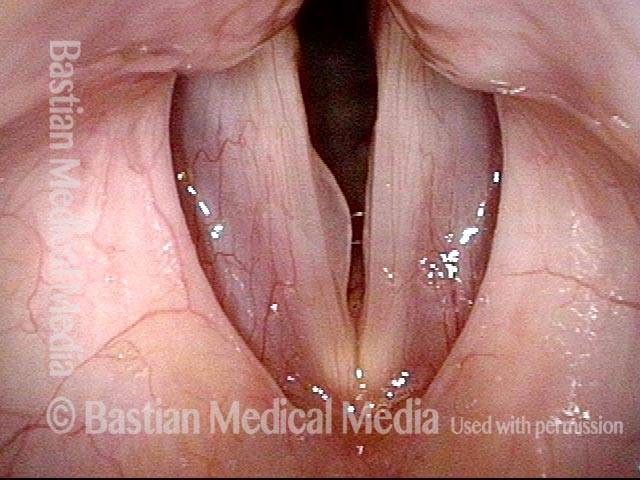
Close-clear view (3 of 4)

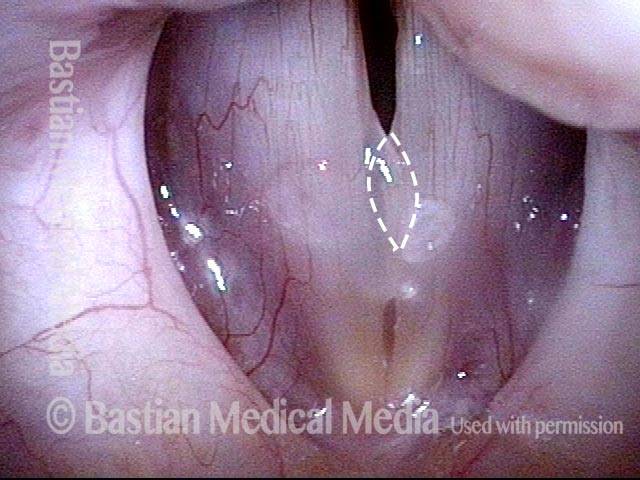
Open phase (4 of 4)

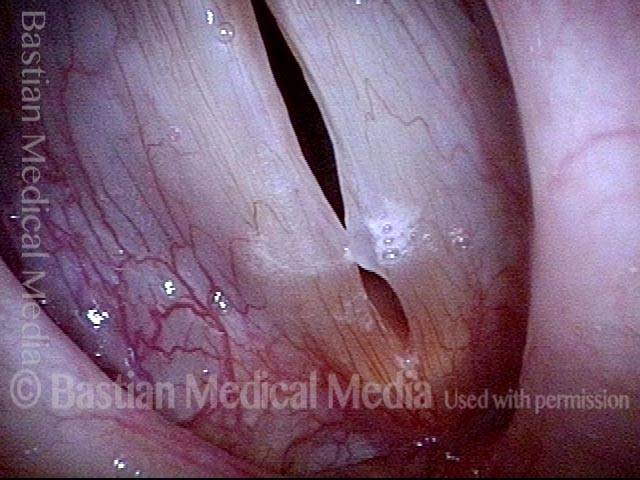
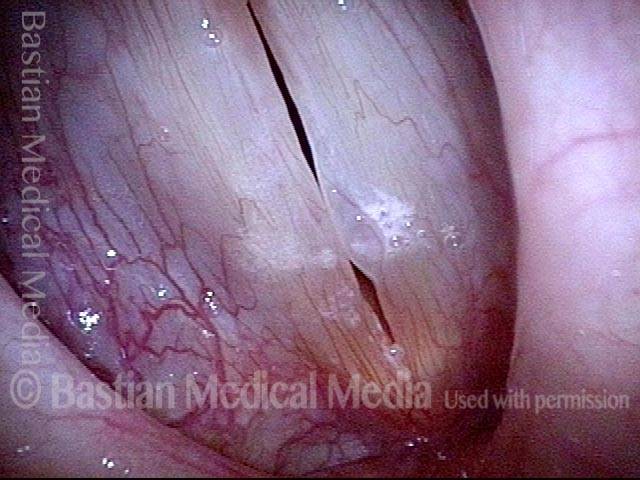
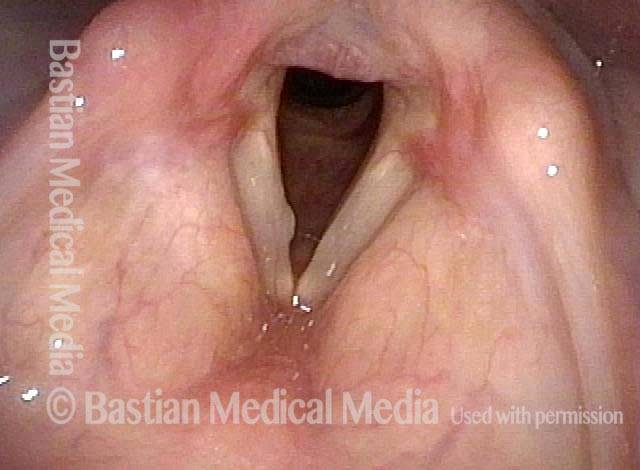
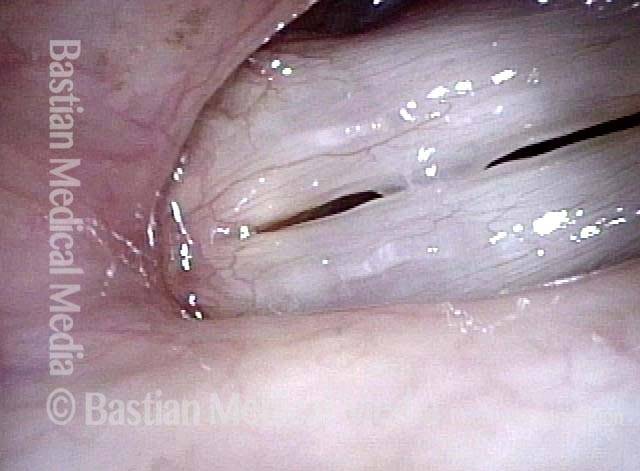
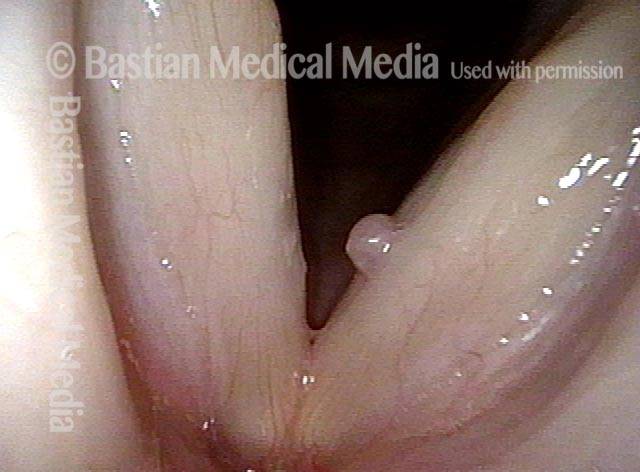
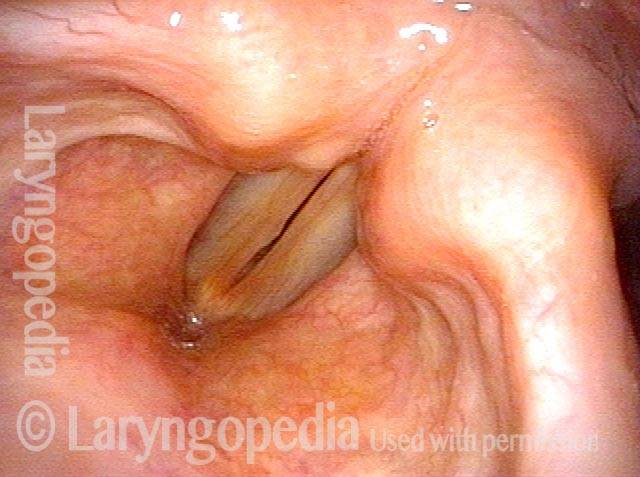
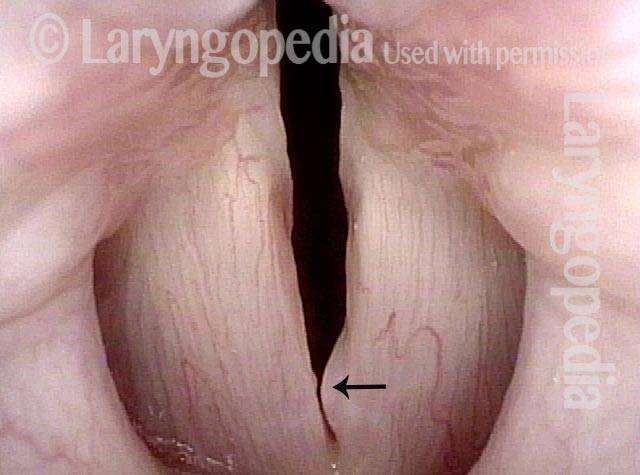
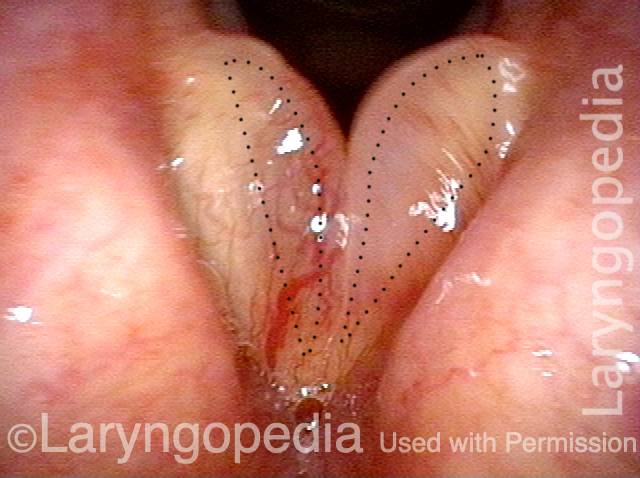
Polyp or Cyst?
Hoarseness (1 of 4)

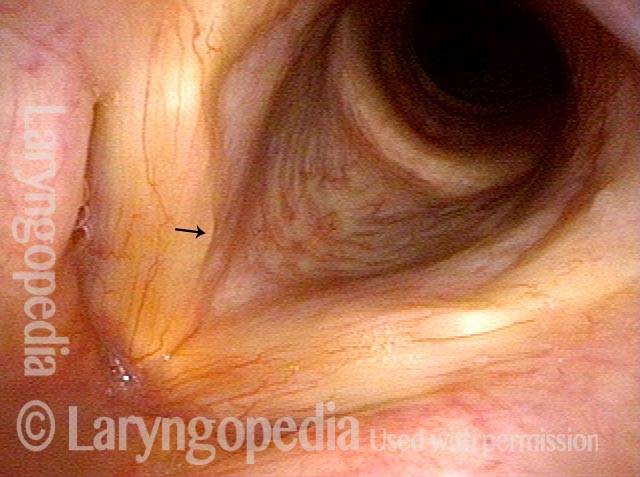
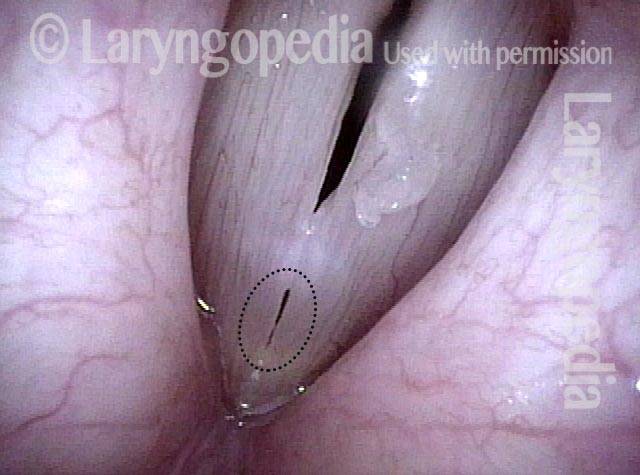
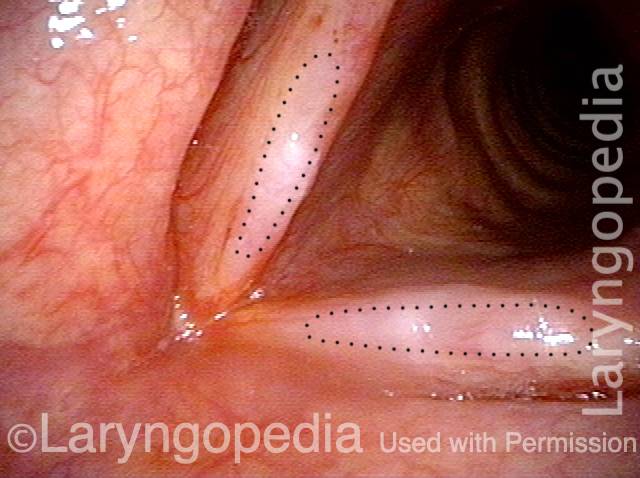
Position of lesion (2 of 4)
Close view (3 of 4)
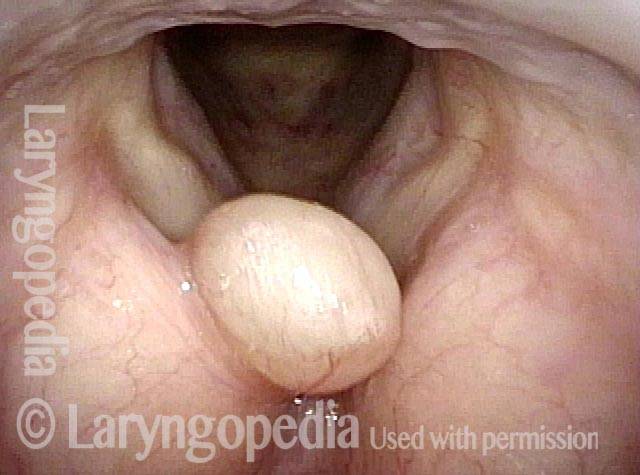
Anterior saccular cyst (4 of 4)

Tiny Vibrating Segment Gives Tiny Tin Whistle Voice
Prephonatory instant (1 of 6)
Phonation (2 of 6)

Gaps due to nodules (3 of 6)

Open phase (4 of 6)

“Tin whistle” sound (5 of 6)
“Tin whistle” at open vibration (6 of 6)

Smoker’s Polyp Reduction Improves Voice Even Though the Larynx Result May not be “Pretty”
Smokers Polyp (1 of 5)
Reine’s edema (2 of 5)
A week after surgery (3 of 5)
Residual Reinke’s edema (4 of 5)

Residual submucosal edema (5 of 5)
![]()
Audio Example 1
Patient comments about the improvement of voice after surgical removal of a vocal cord polyp:
![]()
Audio Example 2
Voice quality, with a vocal polyp, BEFORE surgery:
Same patient, AFTER surgery: