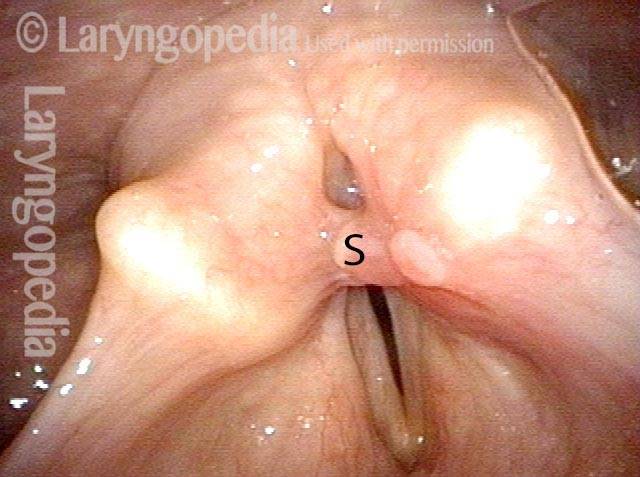
Stenosis is the abnormal narrowing of a passageway in the body. At our practice, it typically refers to narrowing in the breathing passage, such as for narrowing in the glottic, subglottic, or tracheal areas.
Stenosis in the airway can be the result of prolonged endotracheal intubation, external trauma such as gunshot wound, crush injury, or tracheotomy, an inflammatory or auto-immune process, surgical resection of part of the airway for tumor, or other causes.
Symptoms
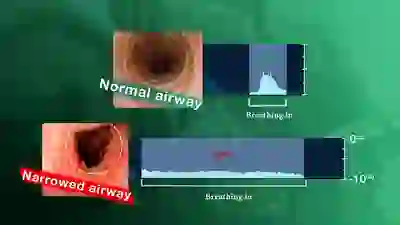
Persons with airway stenosis will note a reduced capacity for exercise. Often the clinician hears noisy breathing on inhalation, especially when the patient is asked to fill the lungs quickly. Esophageal stenosis gives symptoms of difficulty swallowing solids more so than liquids.
Types of stenosis: Idiopathic Subglottic Stenosis, Subglottic Stenosis, Hypopharyngeal Stenosis, Glottic Stenosis, Esophageal Stenosis
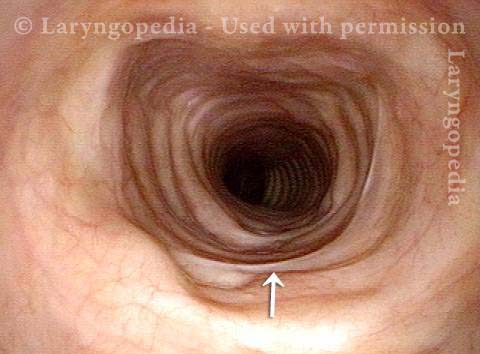
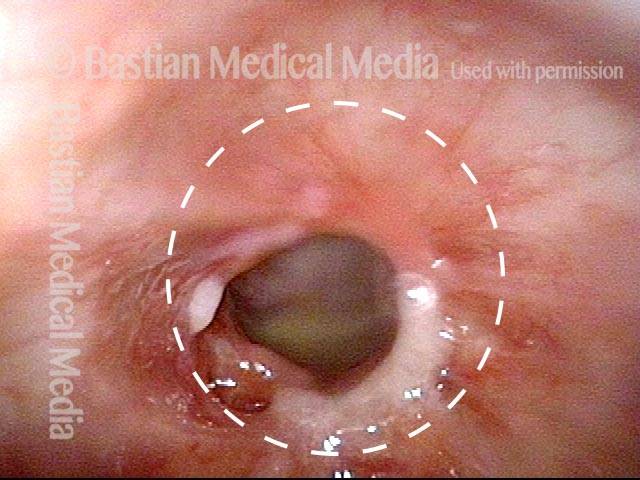
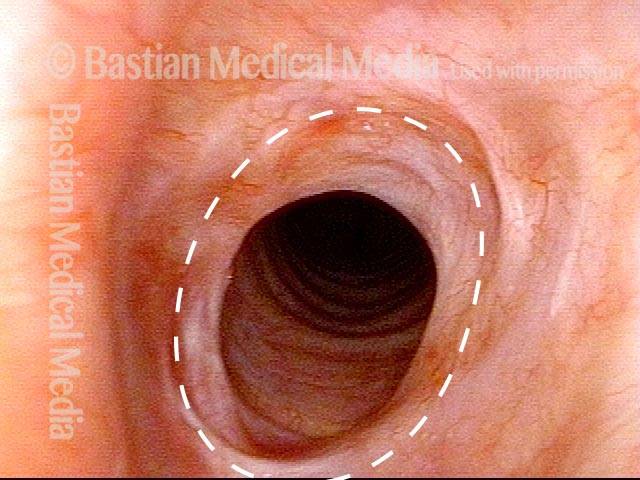
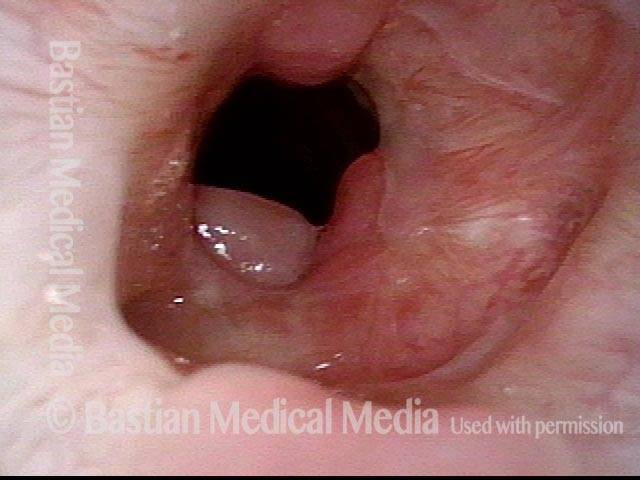
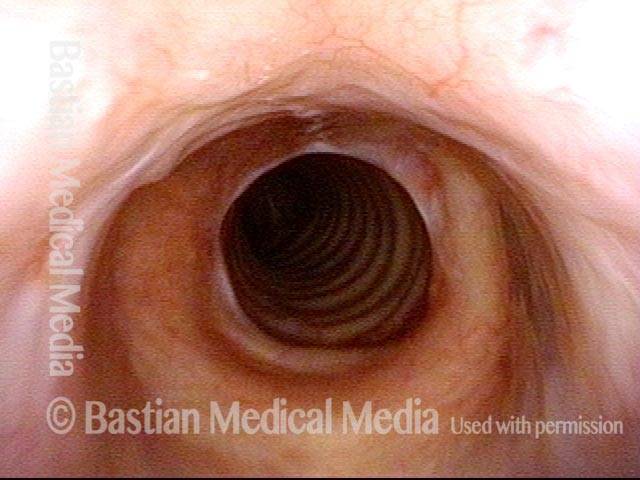
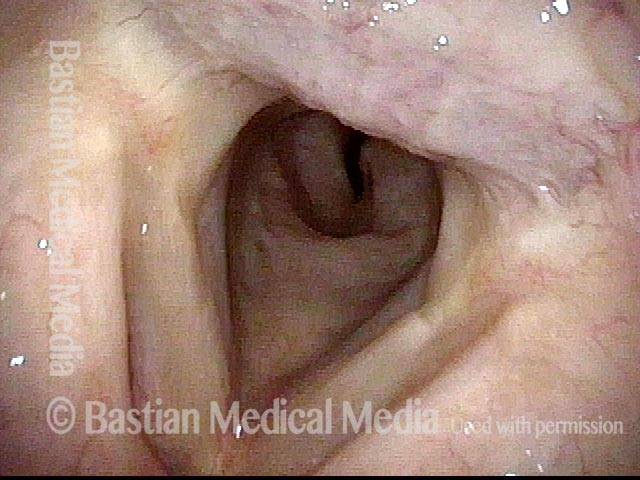
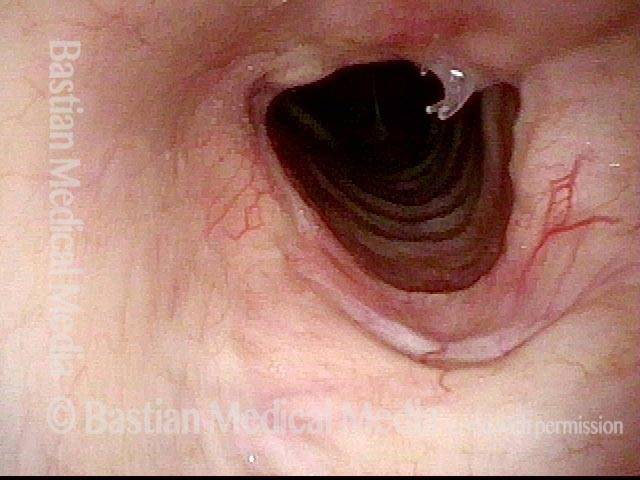
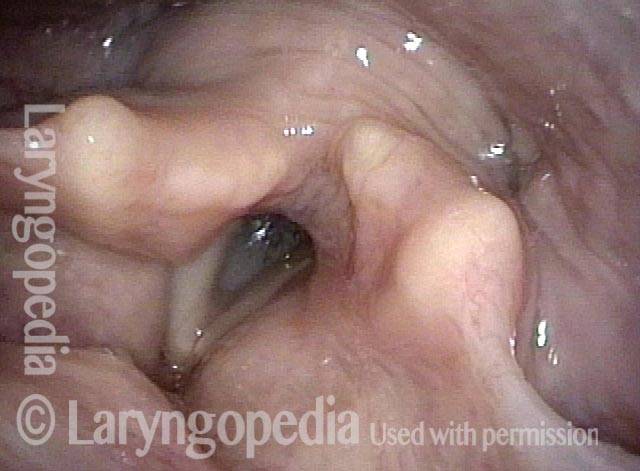
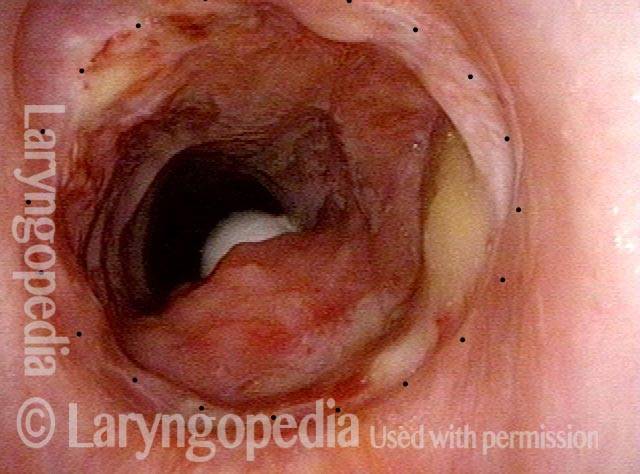
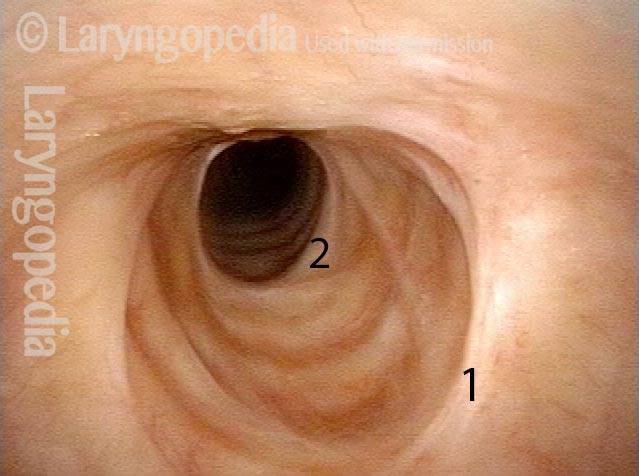
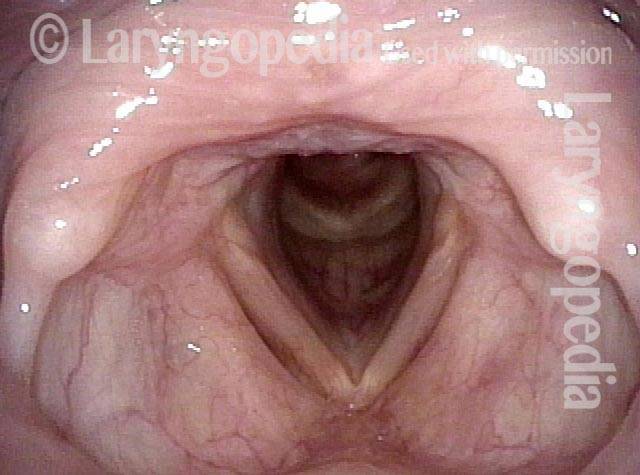
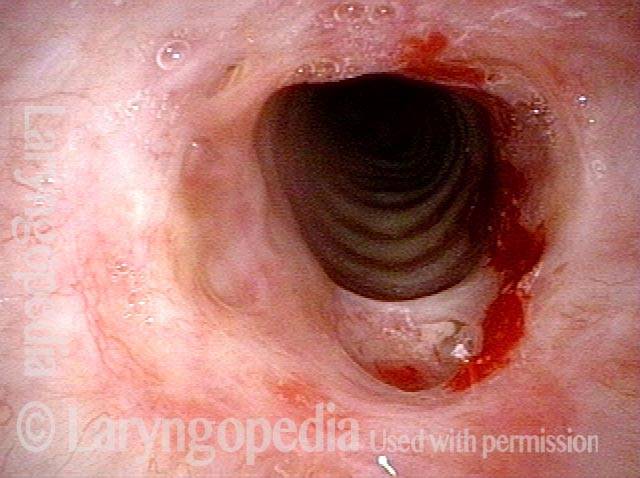
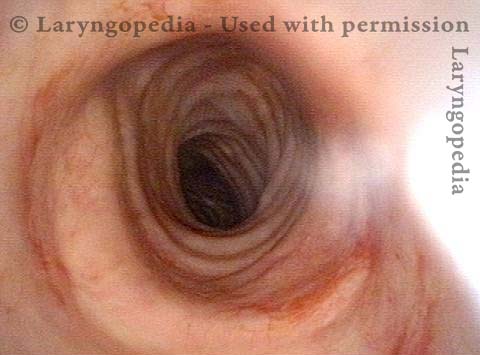
Tracheal Stenosis
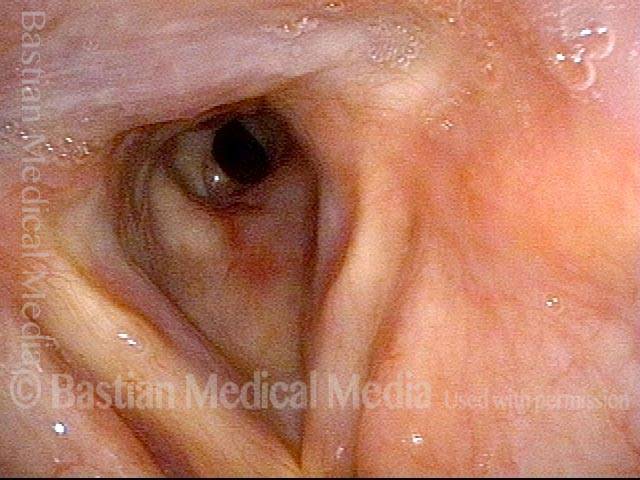
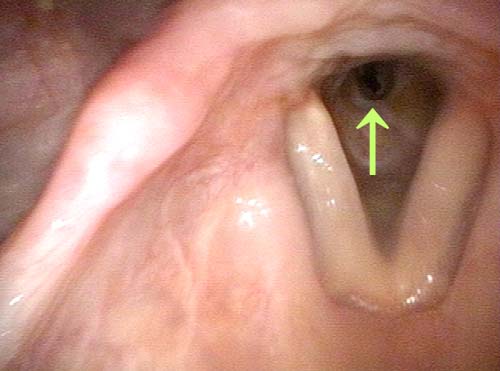
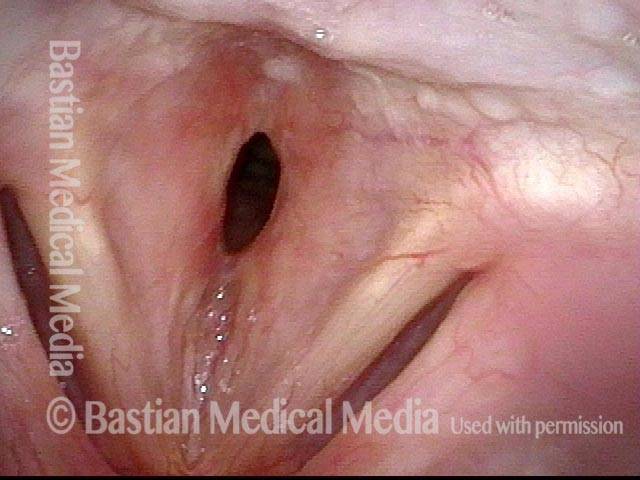
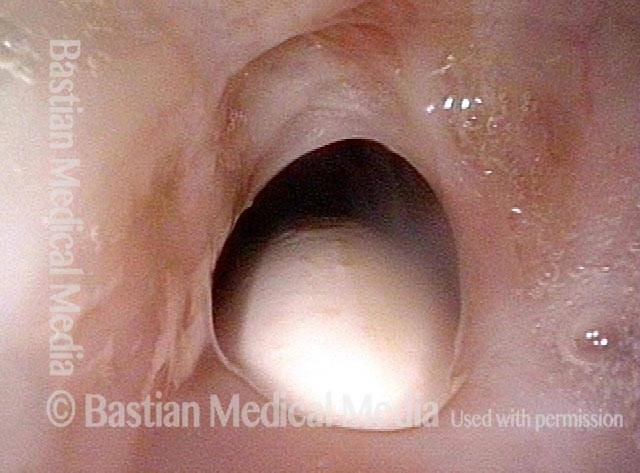
Tracheal stenosis (1 of 4)
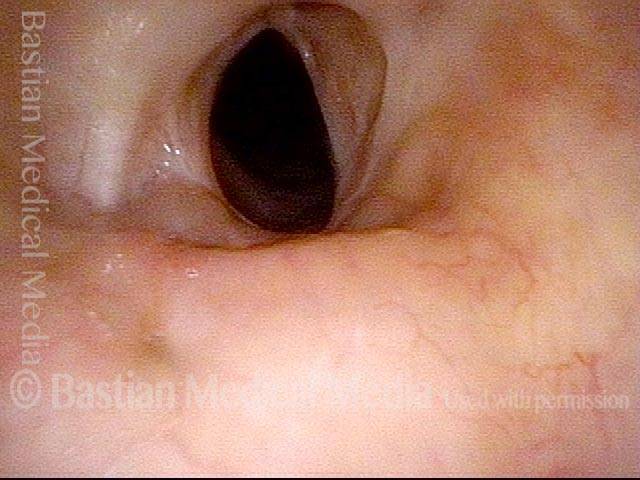
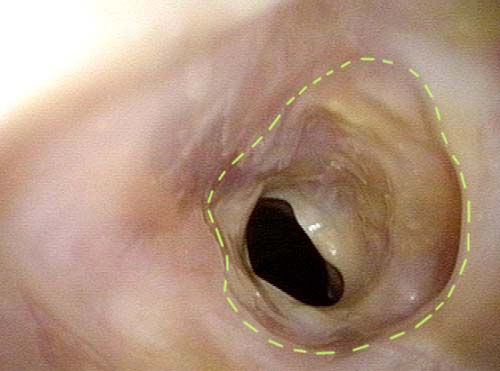
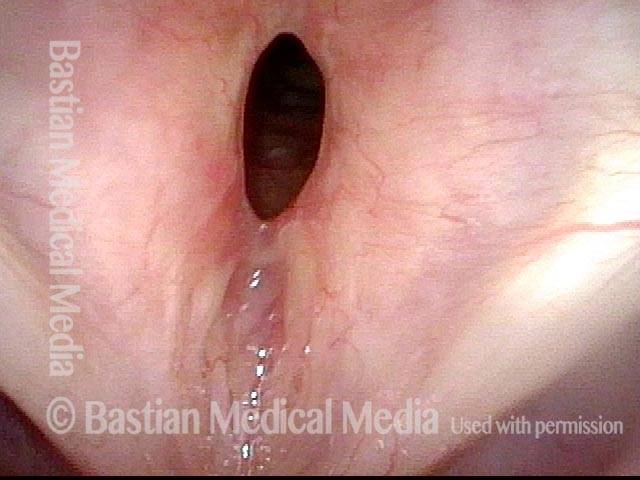
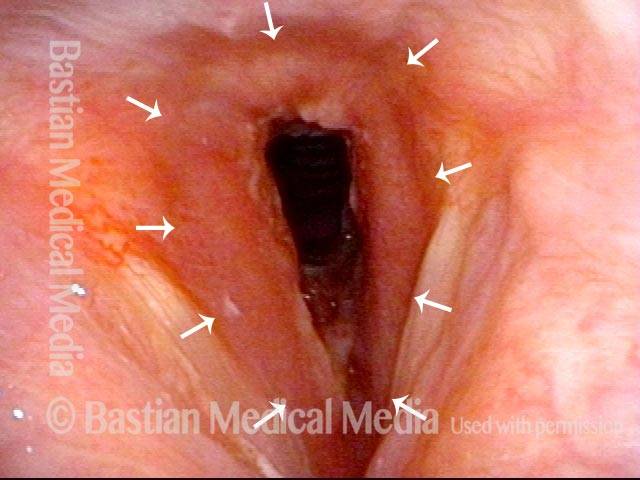
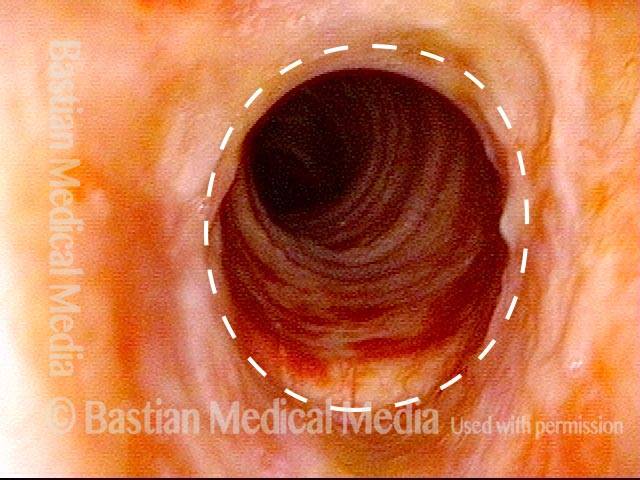
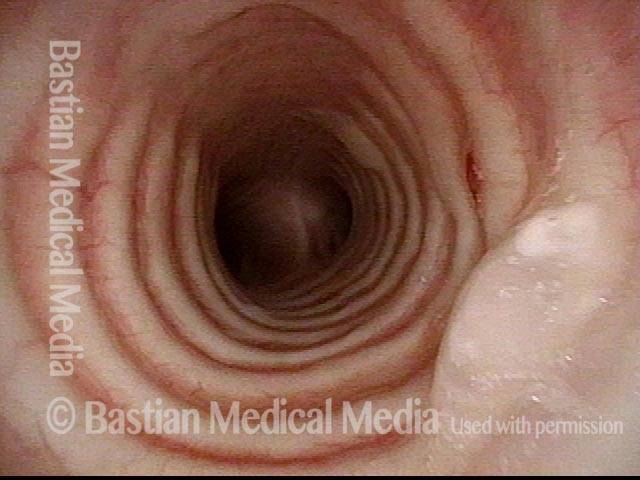
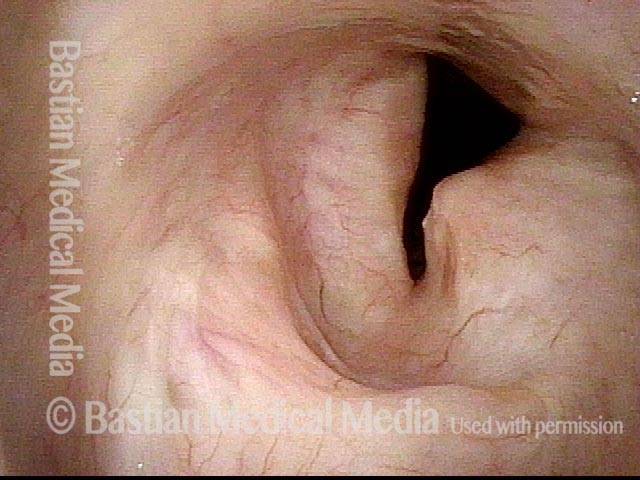
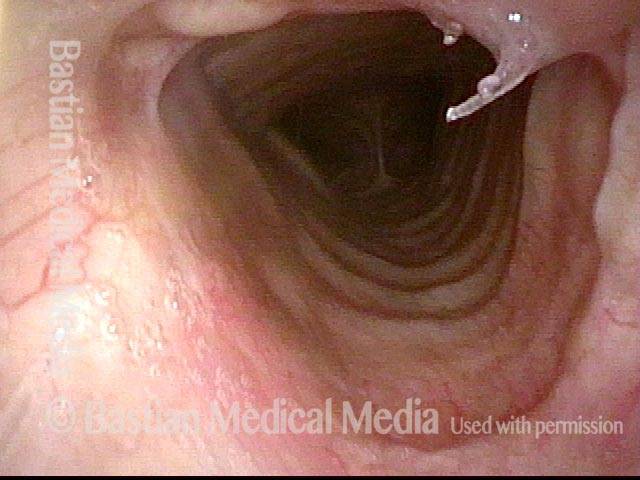
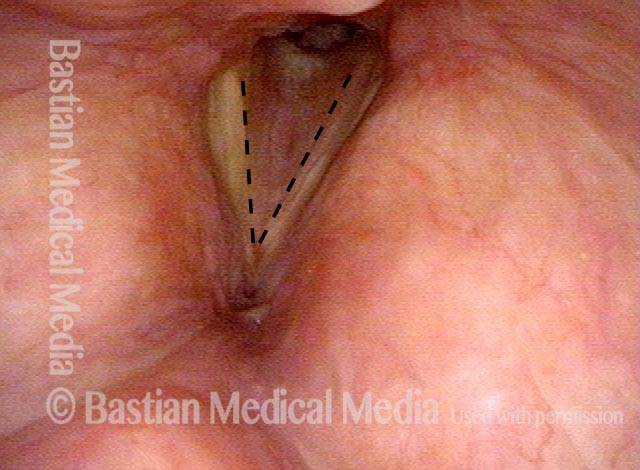
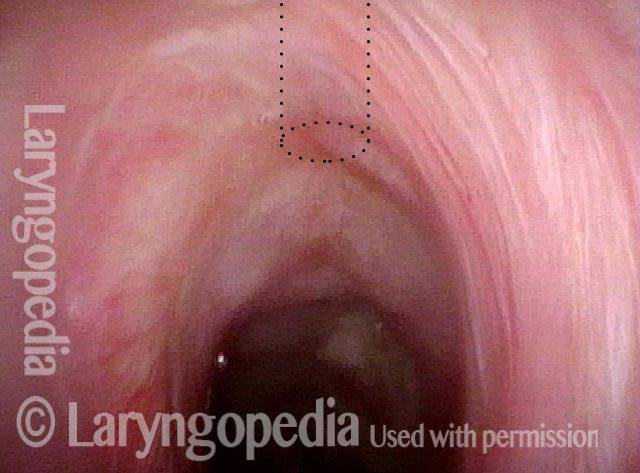
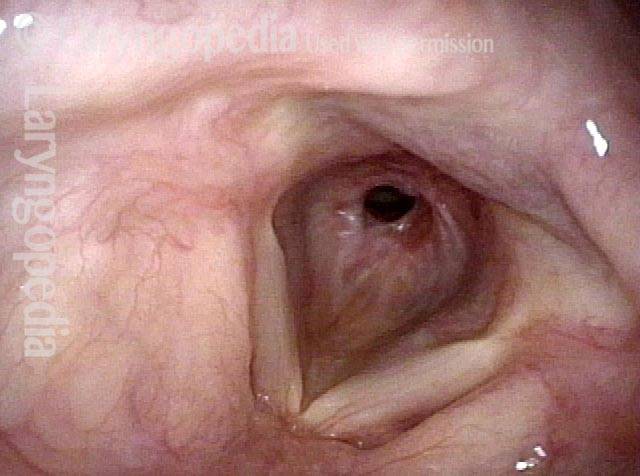
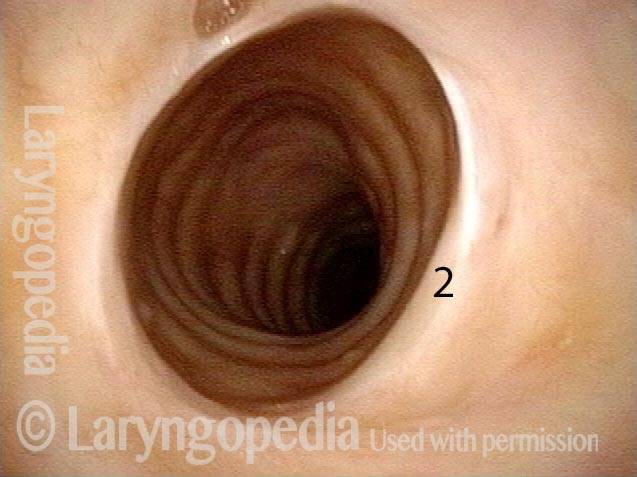
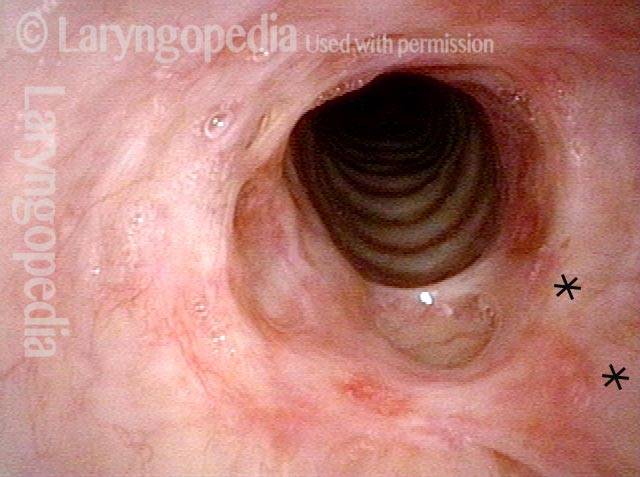
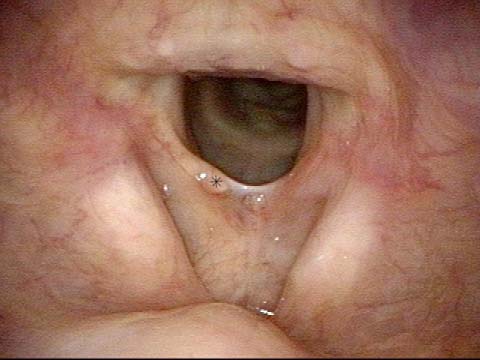
Tracheal stenosis (2 of 4)
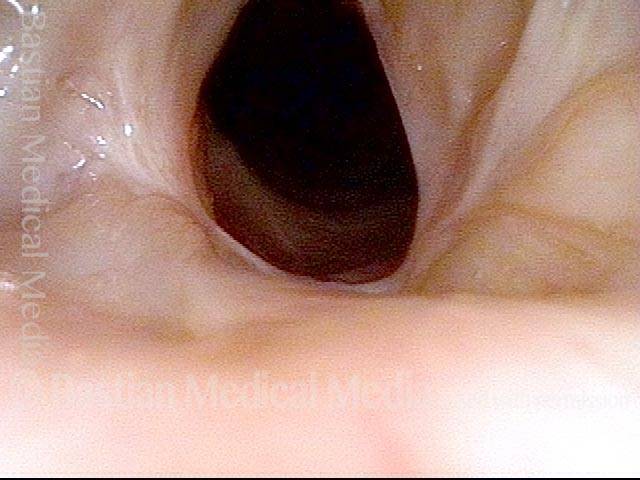
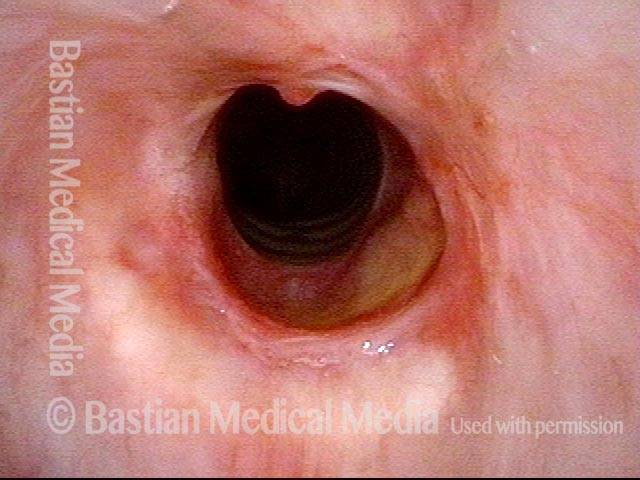
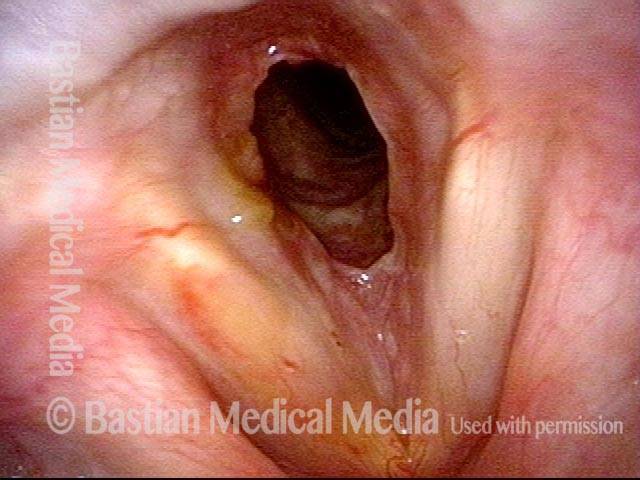
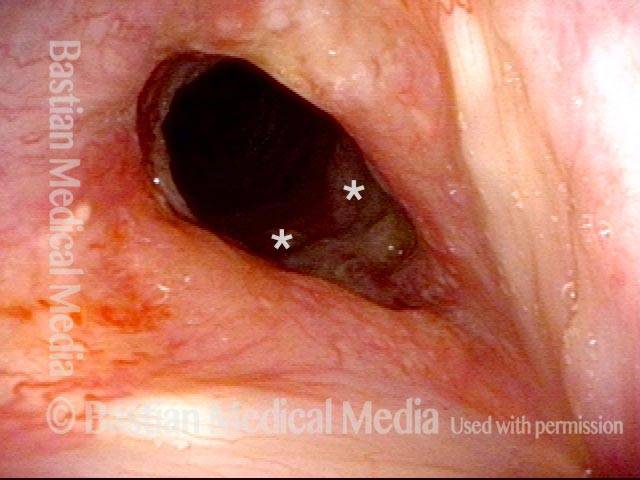
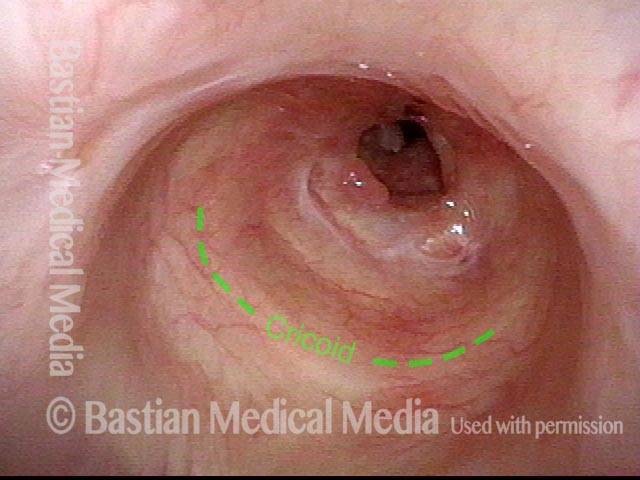
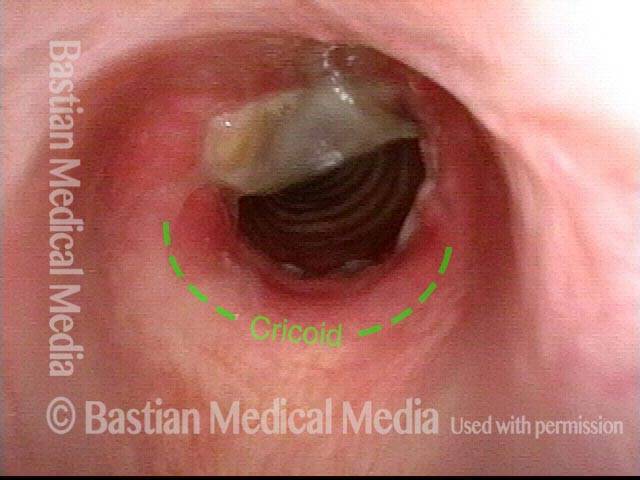
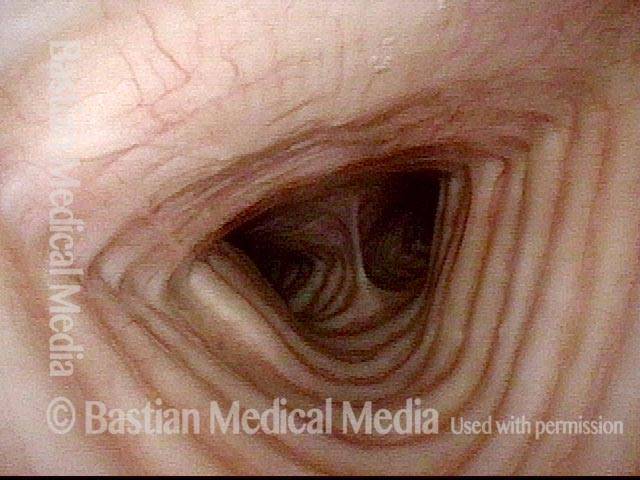
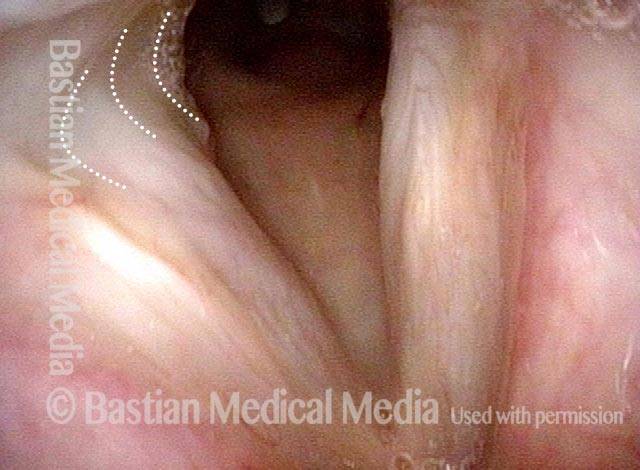
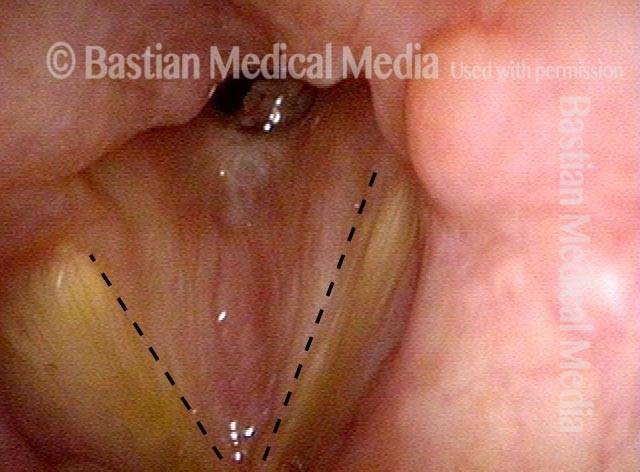
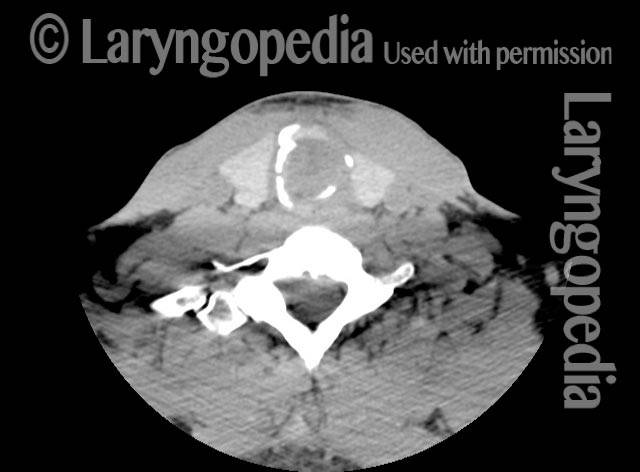
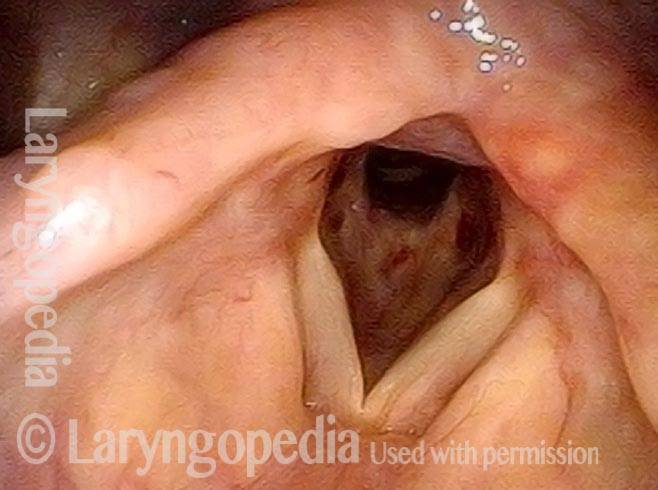
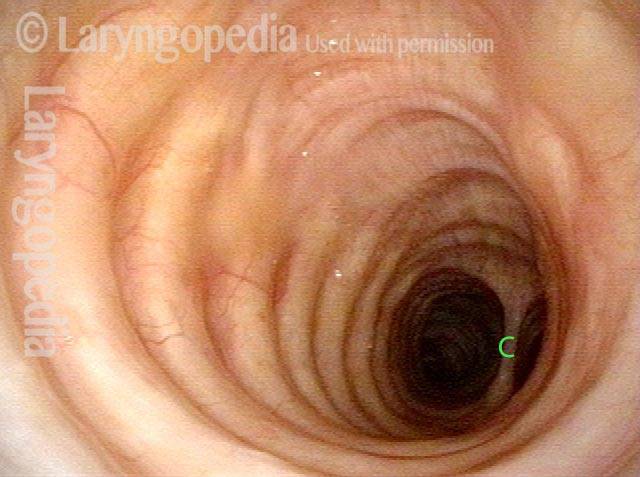
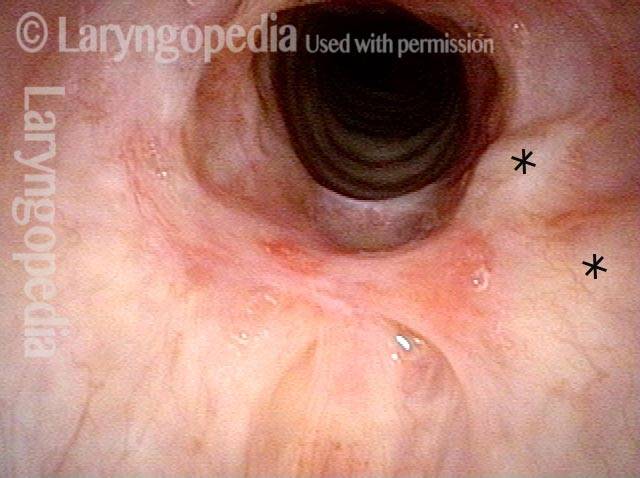
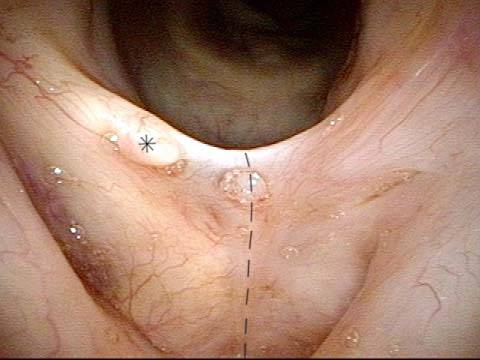
Tracheal stenosis (3 of 4)
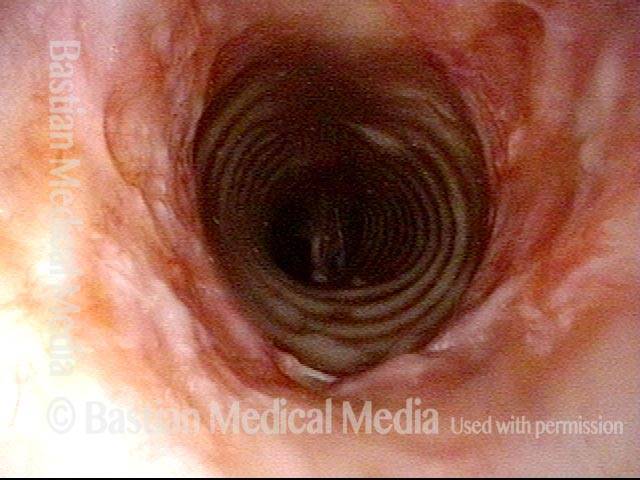
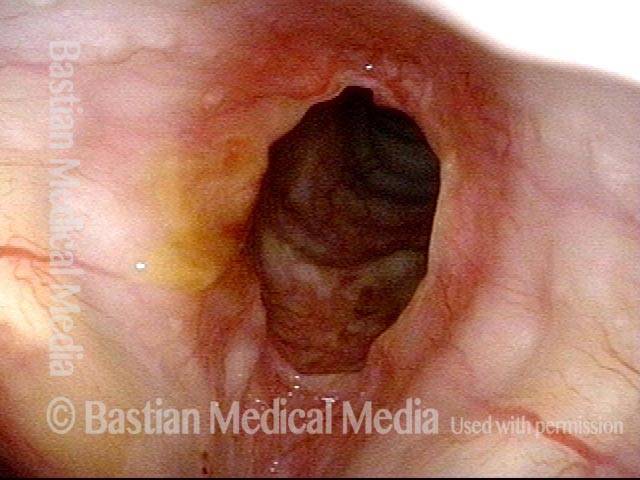
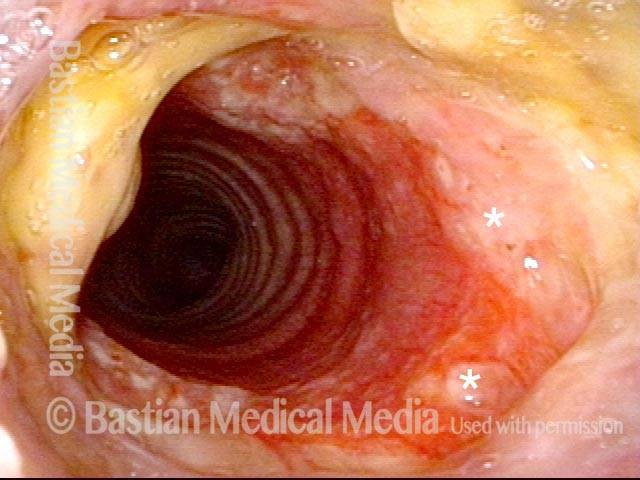
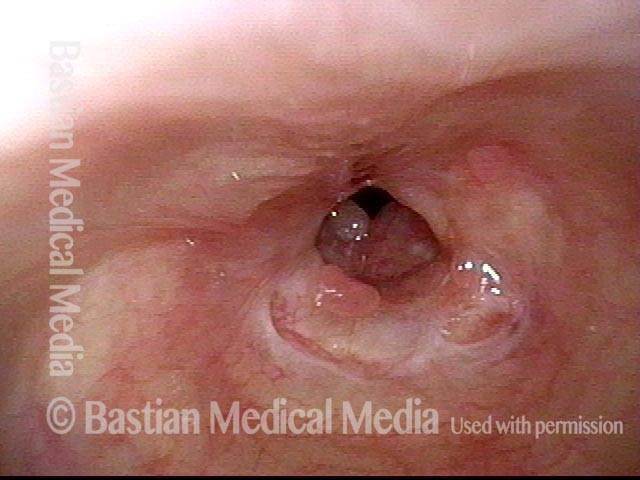
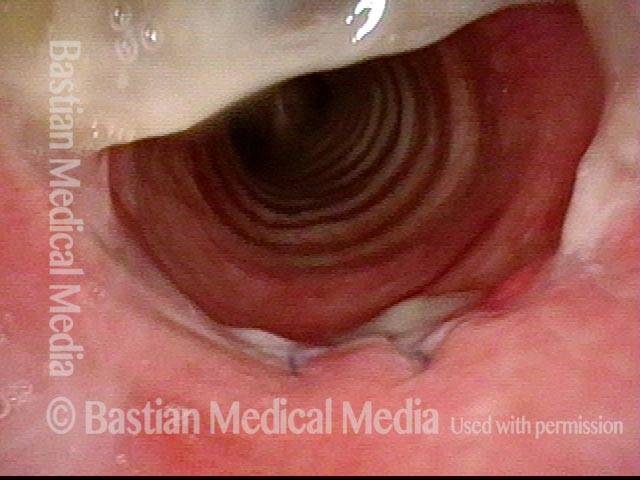
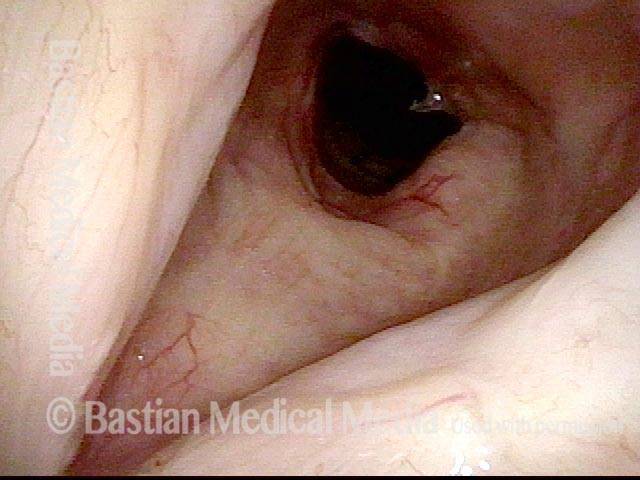
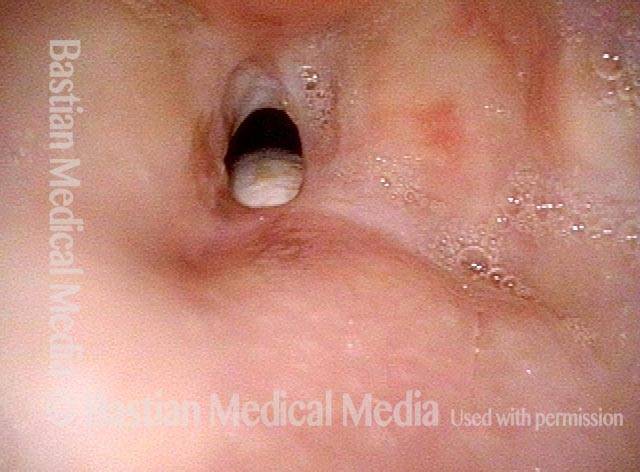
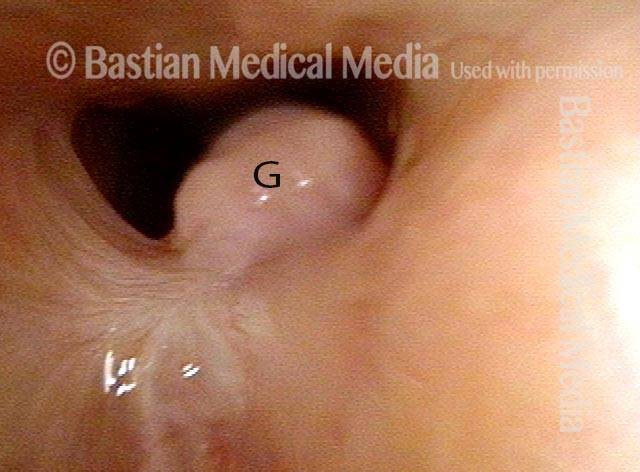
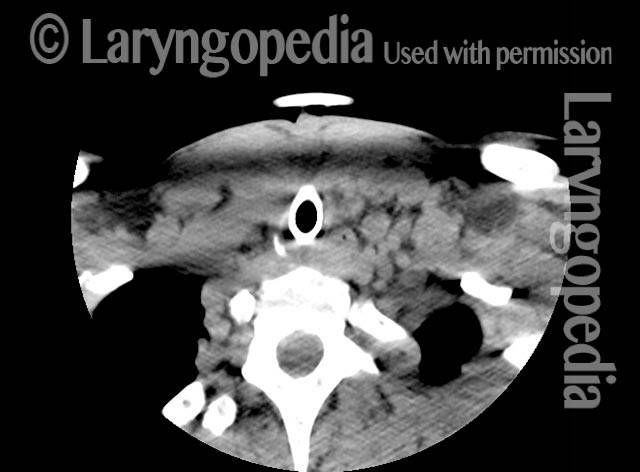
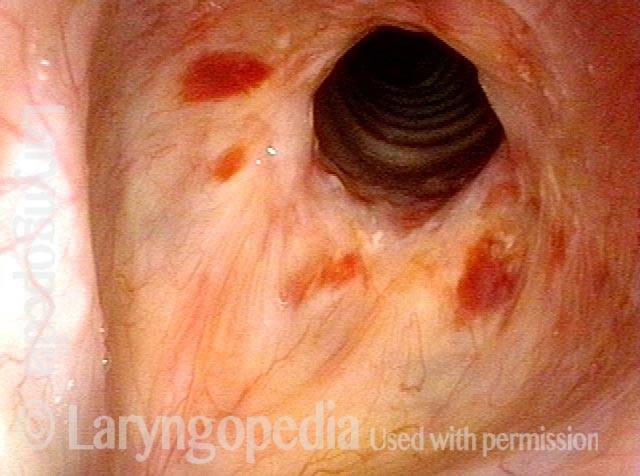
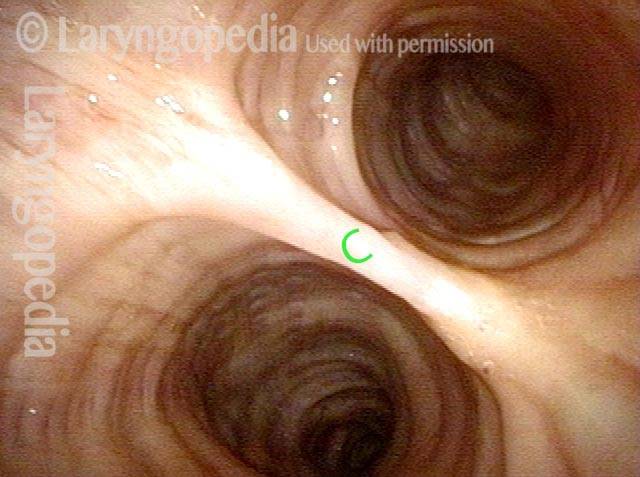
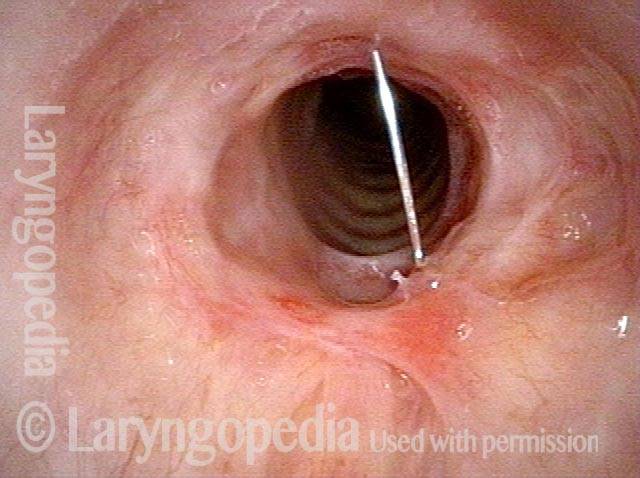
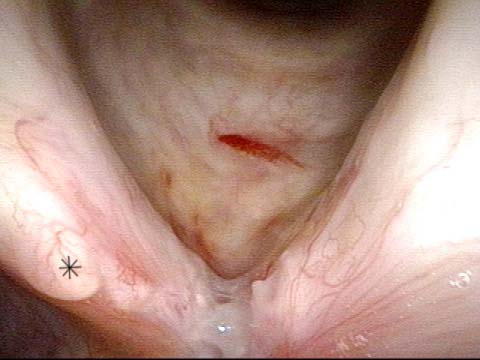
Just below the tracheal stenosis (4 of 4)

Example 2
Tracheal stenosis (1 of 3)

Tracheal stenosis (2 of 3)

Just below the tracheal stenosis (3 of 3)

Example 3
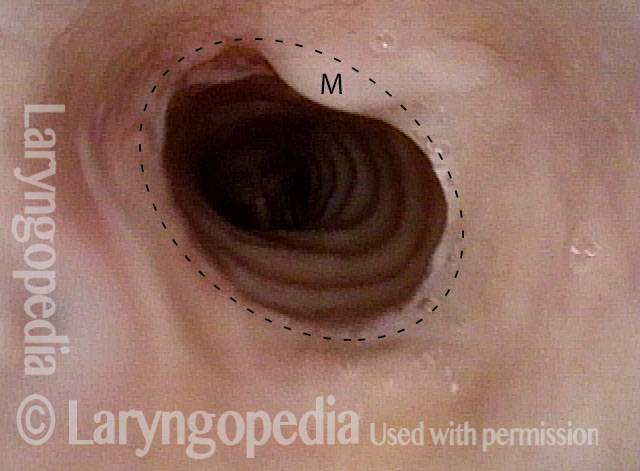
Narrowing in the Trachea > 50% (1 of 2)
Expected Size of Tracheal Opening (2 of 2)
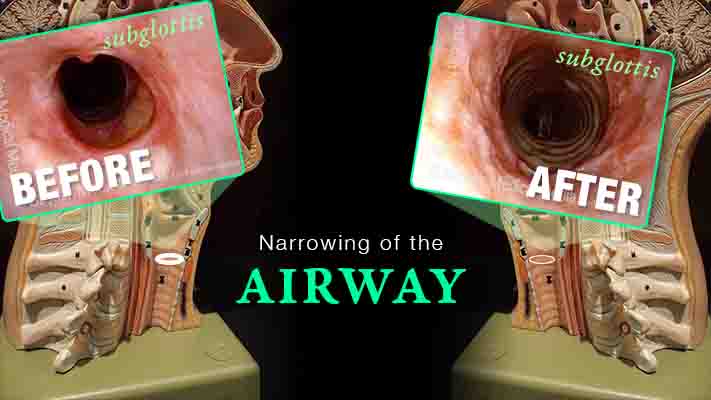
Subglottic Stenosis, before and after Dilation
Subglottic stenosis, before dilation (1 of 2)
Subglottic stenosis, after dilation (2 of 2)
Example 2
Subglottic stenosis (1 of 5)

Subglottic stenosis, worsened (2 of 5)
Subglottic stenosis, worsened (3 of 5)
Subglottic stenosis, after dilation (4 of 5)
Subglottic stenosis, after dilation (5 of 5)
Tracheal Stenosis and Collapse
Tracheal stenosis and collapse (1 of 2)
Tracheal stenosis and collapse (2 of 2)
Tracheal Stenosis, Due to Forme Fruste Wegener’s Granulomatosis
Tracheal stenosis (1 of 3)
Tracheal stenosis (2 of 3)
Just below the tracheal stenosis (3 of 3)

Subglottic / Tracheal Stenosis
Wegener’s granulomatosis (1 of 4)
Subglottic / Tracheal stenosis (2 of 4)

Subglottic / Tracheal stenosis (3 of 4)

Inflammed Stenosis (4 of 4)

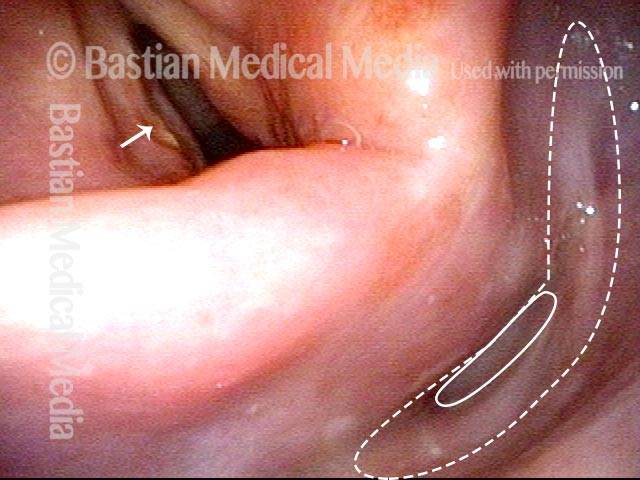
Hypopharyngeal Stenosis
Hypopharyngeal stenosis: not yet visible (1 of 2)
Hypopharyngeal stenosis: revealed (2 of 2)
Subglottic Stenosis, Due to Wegener’s Granulomatosis
Subglottic stenosis, due to Wegener’s (1 of 2)
Subglottic stenosis, due to Wegener’s (2 of 2)
Airway Stenosis Caused By Wegener’s Granulomatosis, Before and After Dilations
Airway stenosis (1 of 5)
Airway stenosis, after dilation (2 of 5)
Airway stenosis, after dilation (3 of 5)
Airway stenosis, before another dilation (4 of 5)
Airway stenosis, after another dilation (5 of 5)
Tracheal Stenosis, before and after Tracheal Resection and Primary Reanastomosis
Tracheal stenosis (1 of 8)
Tracheal stenosis (2 of 8)
Close up view (3 of 8)
Just below the tracheal stenosis (4 of 8)
Tracheal stenosis, 5 days after surgery (5 of 8)
Tracheal stenosis, 5 days after surgery (6 of 8)
Tracheal stenosis, 2 months after surgery (7 of 8)
Tracheal stenosis, 2 months after surgery (8 of 8)

Dilation for Post-Radiation Hypopharyngeal Stenosis
Dilation for post-radiation hypopharyngeal stenosis (1 of 4)
Dilation for post-radiation hypopharyngeal stenosis (2 of 4)
Dilation for post-radiation hypopharyngeal stenosis (3 of 4)
Dilation for post-radiation hypopharyngeal stenosis (4 of 4)

Tracheal Deformity and Stenosis, before and after Repair
Upper tracheal stenosis, before repair (1 of 6)
Upper tracheal stenosis, before repair (2 of 6)
Looking from below the stenosis (3 of 6)
After tracheal repair (4 of 6)
After tracheal repair (5 of 6)
After tracheal repair (6 of 6)
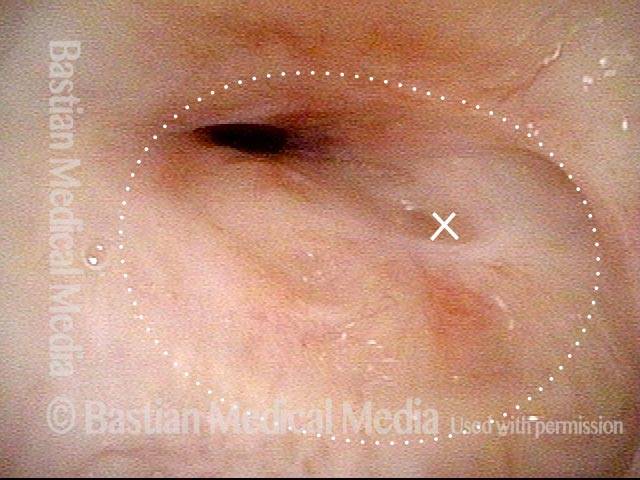
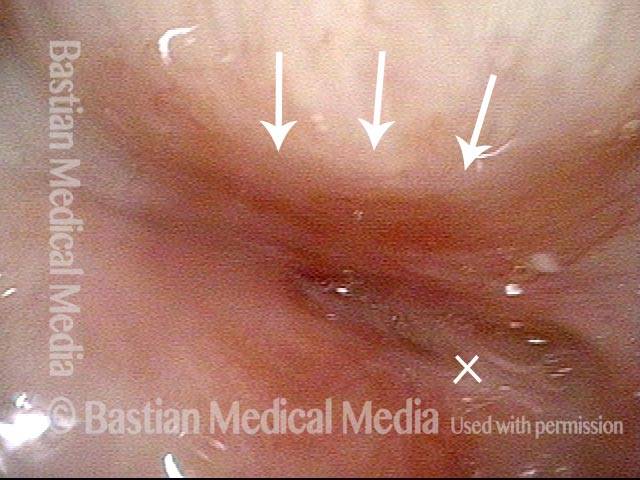
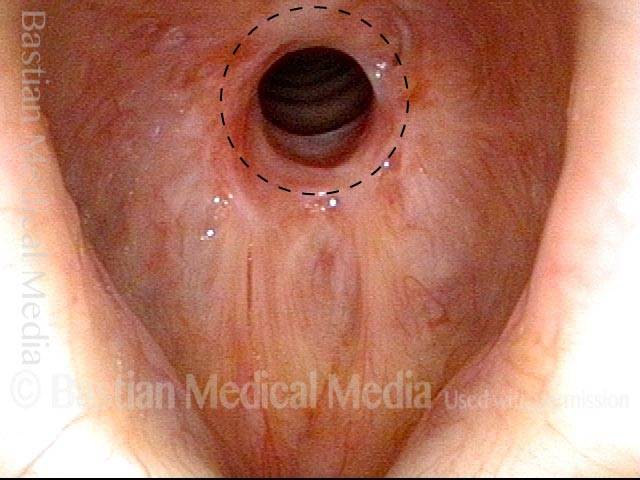
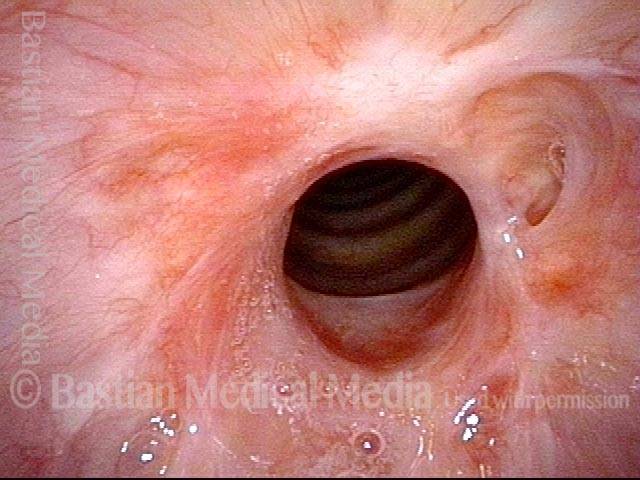
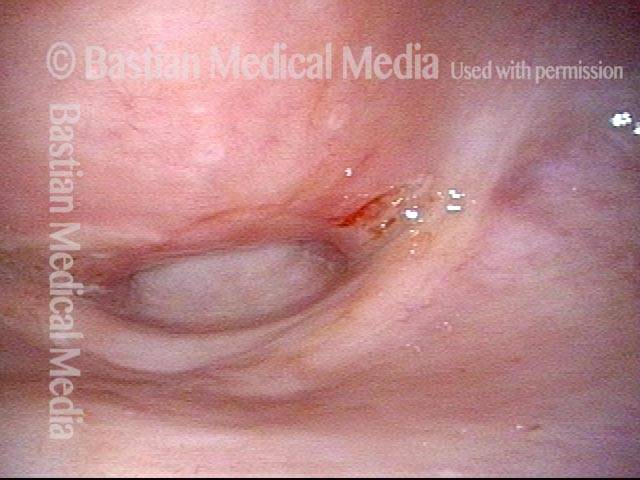
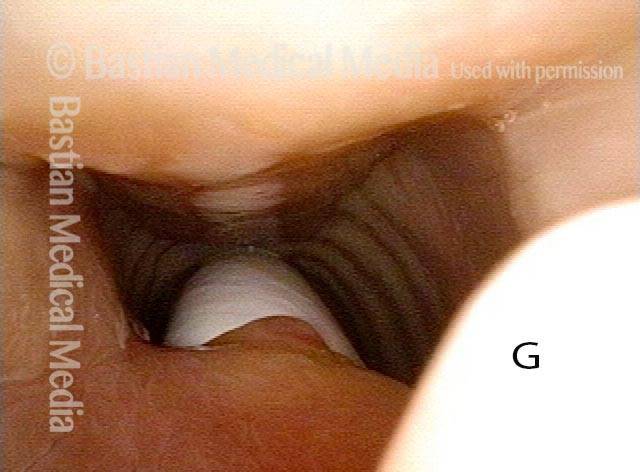
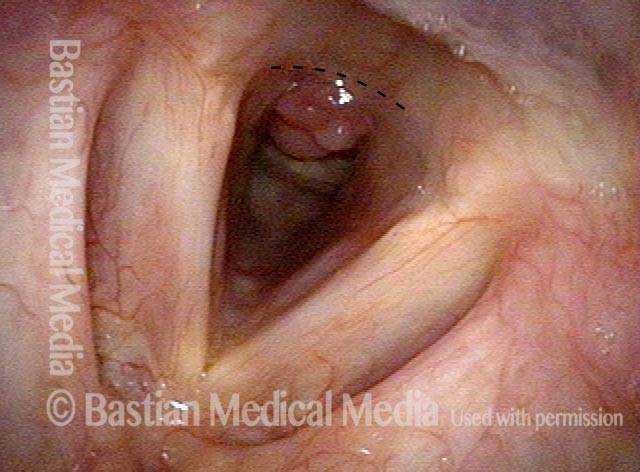
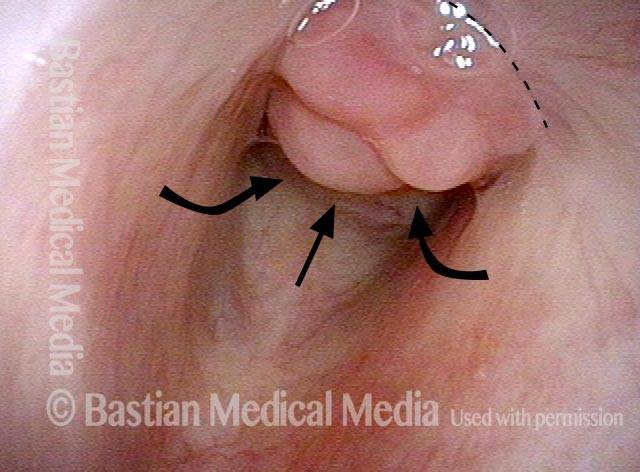
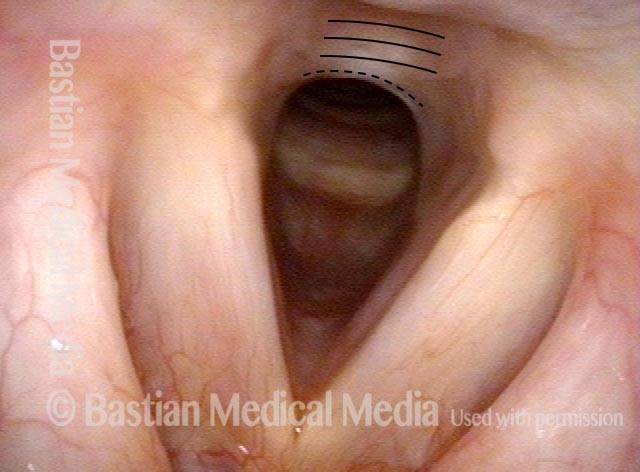
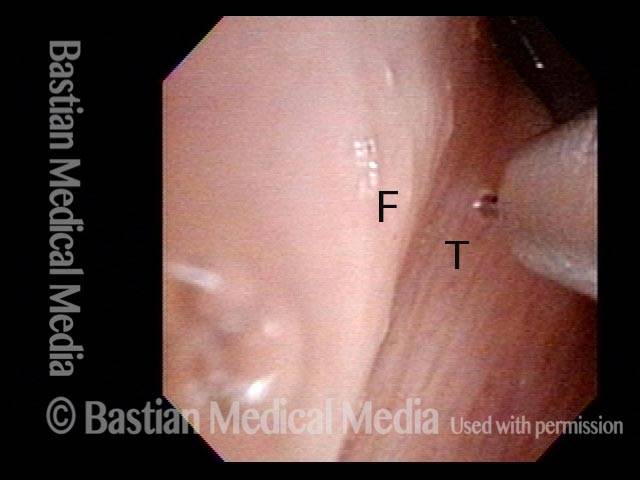
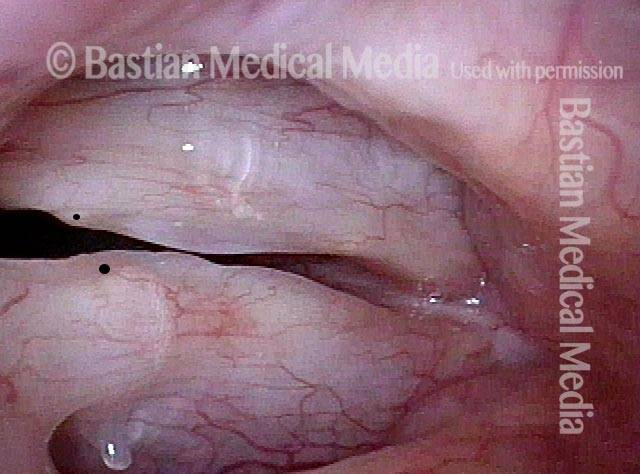
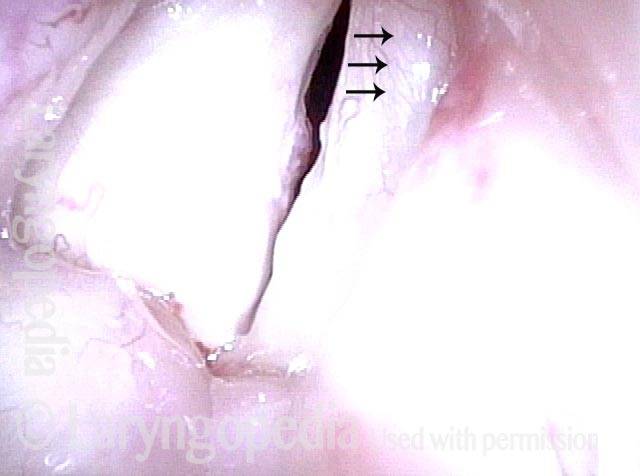
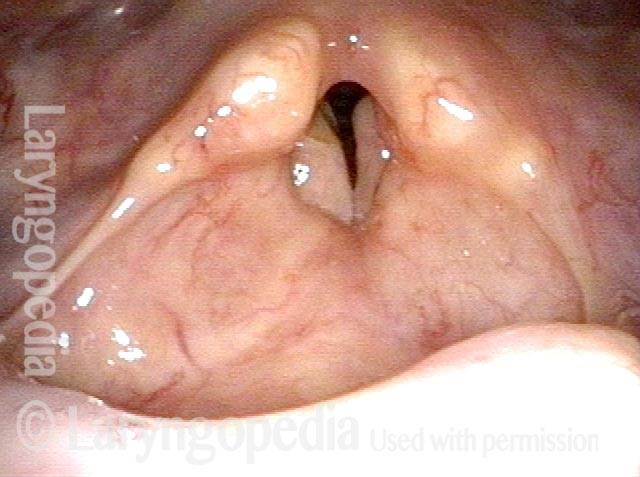
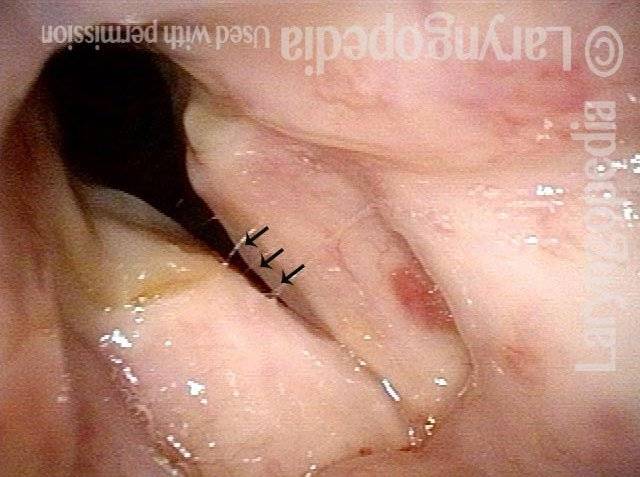
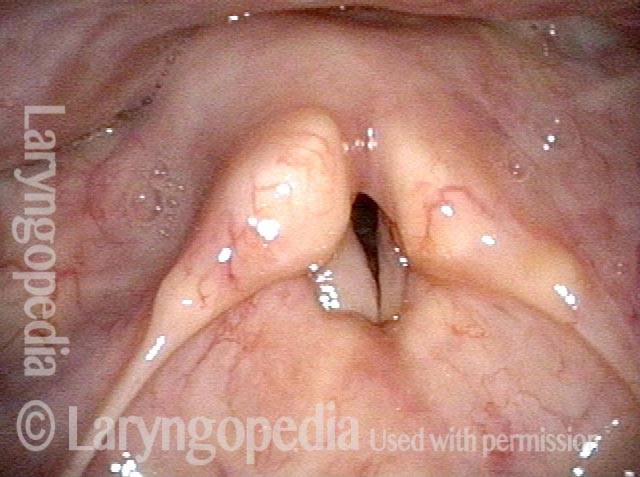
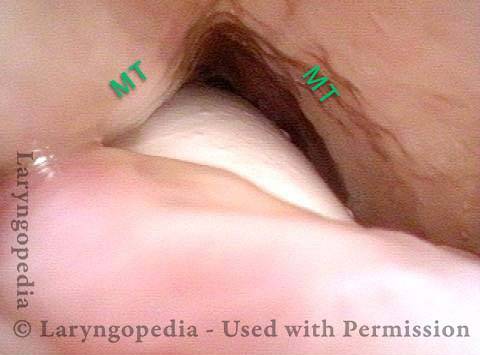
Post-Intubation Stenosis
Endotrachel tube injury (1 of 4)
Closer view, between the posterior vocal cords (2 of 4)

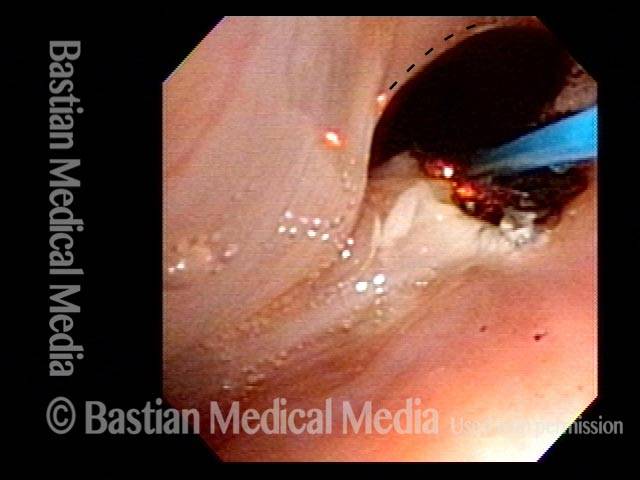
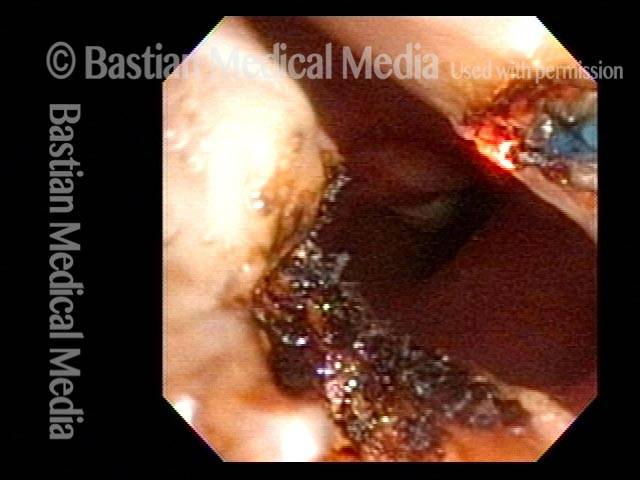
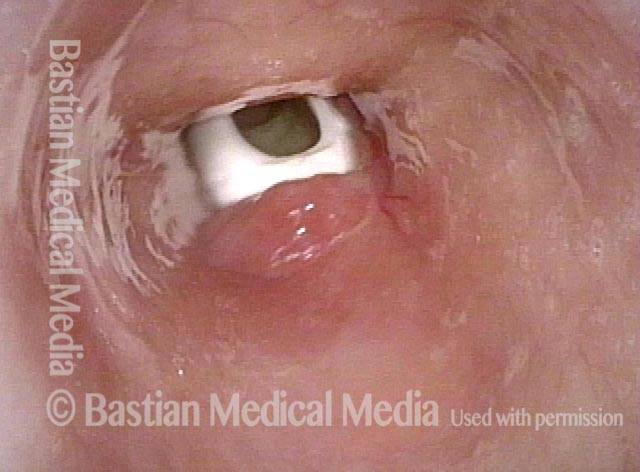
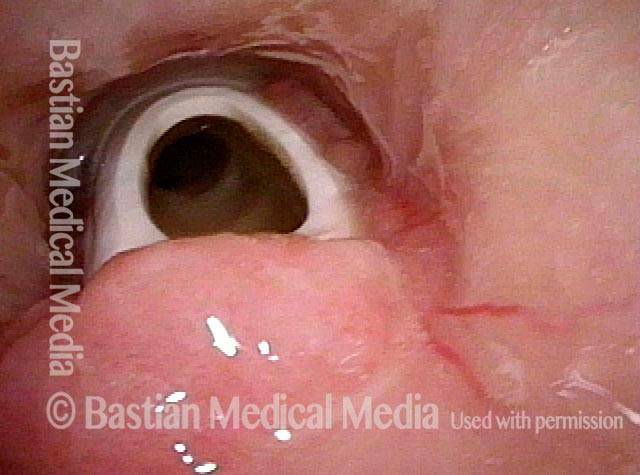
Even closer view, showing upper surface of the tube (3 of 4)
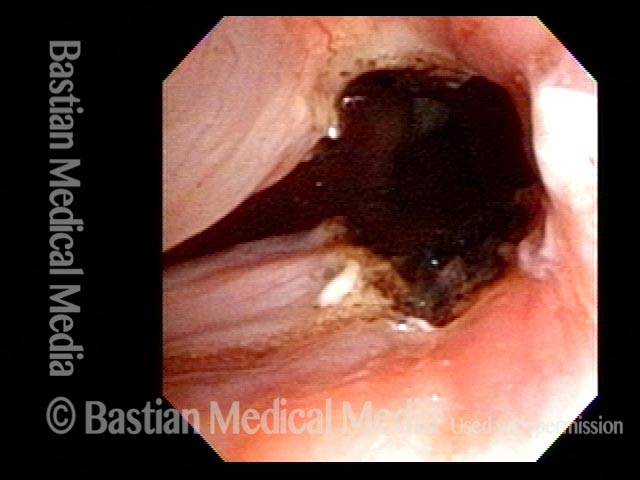
Non-inflammatory stenosis, caused purely by injury (4 of 4)
Sickle Cell Disease and Laryngeal Stenosis
Sickle cell disease and subglottic swelling (1 of 4)
At closer range (2 of 4)
Maturing granuloma (3 of 4)
High-grade stenosis ( 4 of 4)
Subglottic Granulation and Curving Airstream
Intubation injury (1 of 4)
Lobules (2 of 4)
2 months later (3 of 4)
Scar band (4 of 4)

Office-Based Surgery When General Anesthesia Is too Risky
Involuntary inspiratory voice (1 of 6)

Laser posterior commissuroplasty (2 of 6)
During the commissuroplasty (3 of 6)
Deepening divot (4 of 6)
Inspiratory indrawing decreased (5 of 6)
Phonation (6 of 6)
The Adult Result of Infant Cricoid Split
Cricoid split procedure (1 of 6)
Rotated view (2 of 6)

Open phase (3 of 6)
Cricoarytenoid joints (4 of 6)

Lateral excursion (5 of 6)
Closed phase (6 of 6)
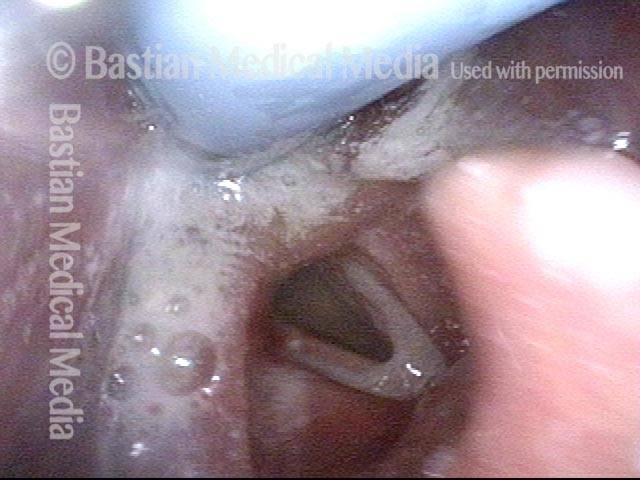
A Fenestrated Trach Tube Allows Voicing when there Is Stenosis
Tracheotomy (1 of 4)

View below vocal cords (2 of 4)
Fenestra (3 of 4)
Patient post-trach (4 of 4)
Stenosis of Larynx and Trachea before and after Cricotracheal Resection and Reanastomosis
Post intubation and tracheotomy (1 of 8)
Confirmed stenosis (2 of 8)

Tracheotomy tract (3 of 8)
Cricoid cartilage (4 of 8)
Resection needed (5 of 8)
Post surgery (6 of 8)

Trach removed (7 of 8)
Patient’s sentiment (8 of 8)

Stenosis Before and After Dilation for Forme Fruste Wegener’s
Subglottic stenosis (1 of 5)
Inflammation (2 of 5)

Flexible scope (3 of 5)

Post-dilation (4 of 5)
Post-operative bruising (5 of 5)
Sometimes “low-tech” Is Best for Stenosis
Esophageal bougie (1 of 4)
Swallowing crescent (2 of 4)
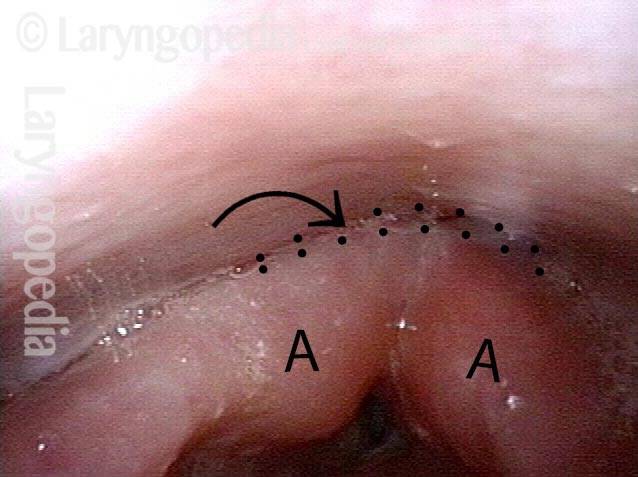
Post-arytenoid area (3 of 4)

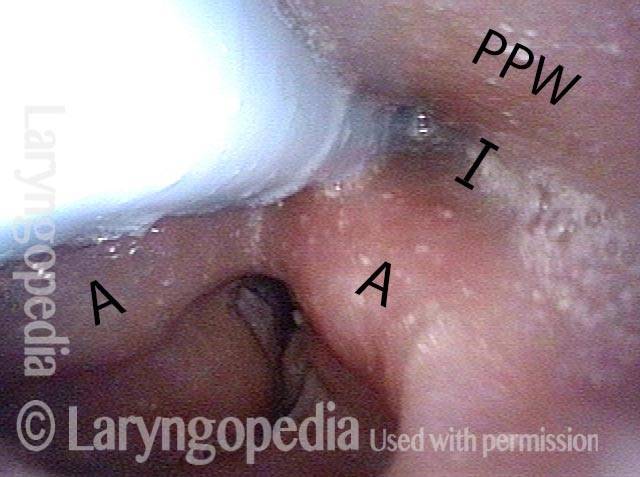
Maximum diameter (4 of 4)
Who knew…? Many Such Injuries Are Never Found
Coughing evaluation (1 of 6)
Intubation scars (2 of 6)

Stenosis (3 of 6)
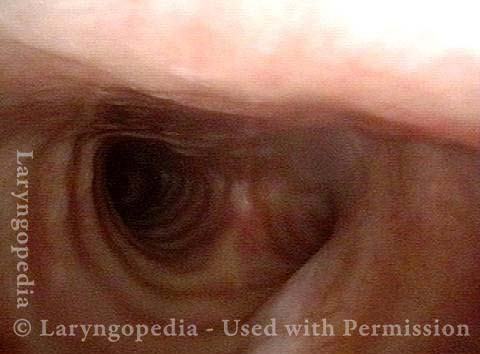
Further down trachea (4 of 6)
Below stenosis (5 of 6)
Carina (6 of 6)
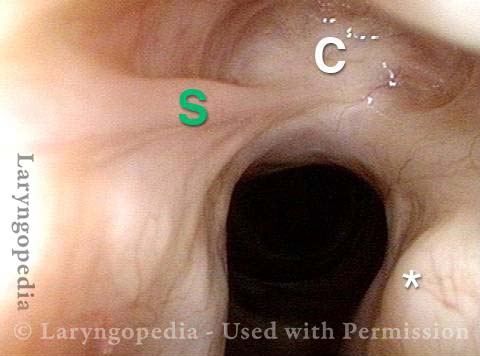
Stenosis at Two Levels: Supraglottic and Glottic
Laryngeal stenosis post intubation (1 of 7)
Closer range (2 of 7)
Posterior commissure (3 of 7)
View into trachea (4 of 7)

Post laser release (5 of 7)

Scarring (6 of 7)
Closer view (7 of 7)
Progressive Radiation Fibrosis Effects on the Larynx and a Solution to some of it
Forty years post-radiation (1 of 8)
Involuntary inspiratory voice (2 of 8)
Only capable of high pitch (3 of 8)
Open phase vibration (4 of 8)
One week post-commissuroplasty (5 of 8)
Rapid inhalation, closer view (6 of 8)
Three months post-surgery (7 of 8)
Closer view, post-surgery (8 of 8)

Tracheal Red Herring; the Real Culprit is Cricopharyngeus Spasm
Tracheal stenosis? (1 of 4)
Narrowing at trachea (2 of 4)

Closer view (3 of 4)

No significant change in breathing (4 of 4)

A Different Approach to Inflammatory Tracheal Stenosis
Planning on periodical injections (1 of 4)
Long-acting steroid (2 of 4)
Needle going into the posterior of stenosis (3 of 4)
Posterior tracheal wall (4 of 4)
Motivated Airway Examination Avoids Further Surgery
Marginal airway (1 of 4)

Airway at close range (2 of 4)

Forced inspiration (3 of 4)
Alternative to tracheotomy (4 of 4)

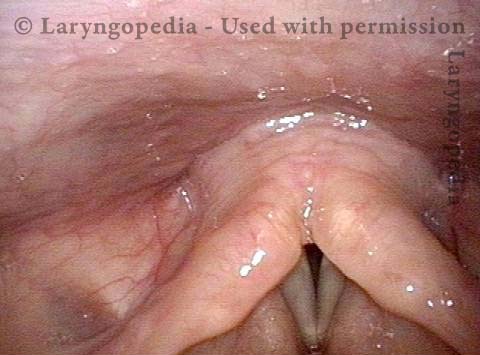
Supraglottic (above the vocal cord) scarring as a result of radiotherapy
Supraglottic Scarring (1 of 4)
Hoarseness caused by radiation effects (2 of 4)

Cords don’t close completely (3 of 4)
Normal caliber trachea (4 of 4)
Glottic Web Management Without A Keel
Glottic Web (1 of 7)
Glottic Web (2 of 7)
Glottic Web (3 of 7)
Glottic Web (4 of 7)

Re-grown mucosa (5 of 7)
Closed phase of vibration (6 of 7)
Restoration of oscillatory ability (7 of 7)

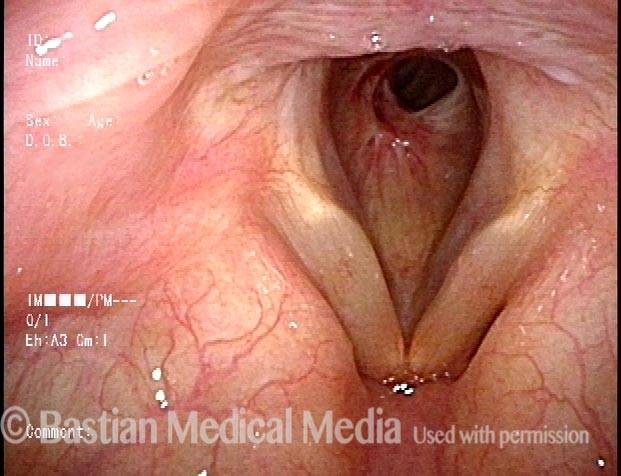
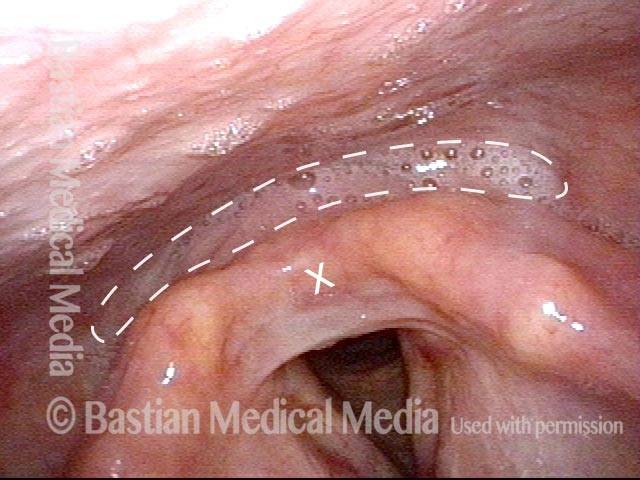
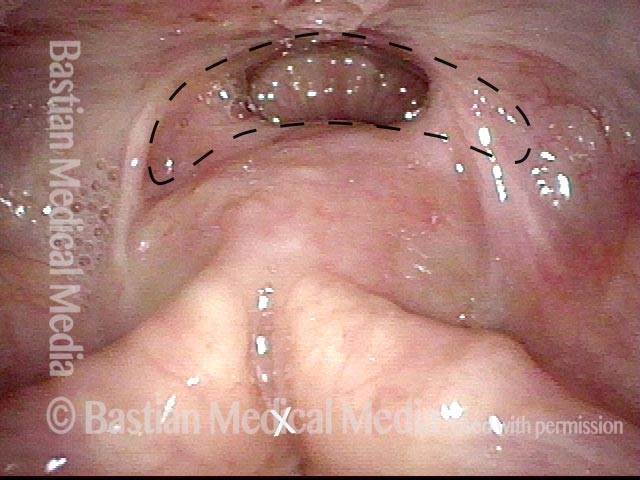
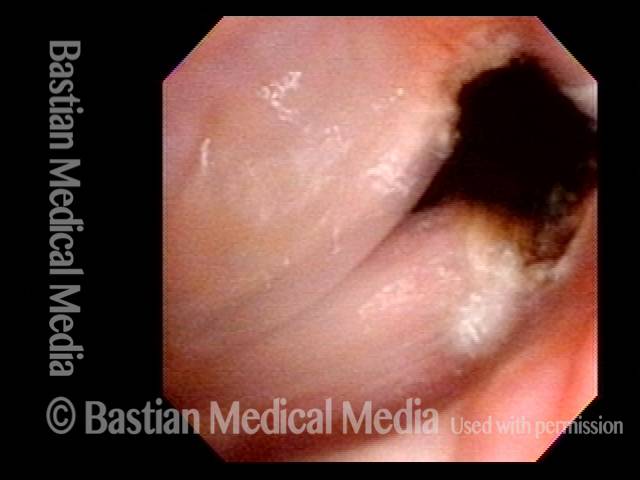
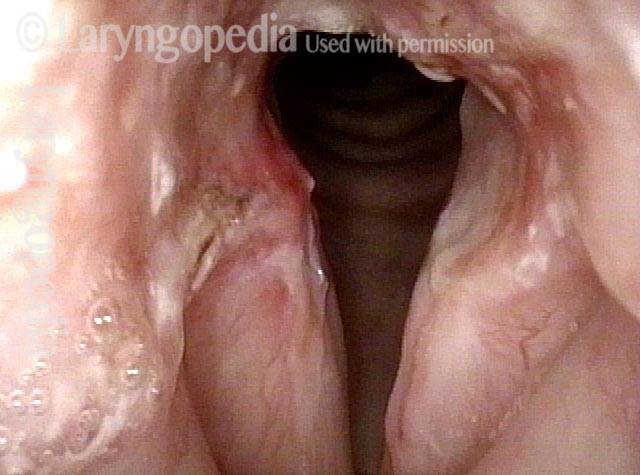
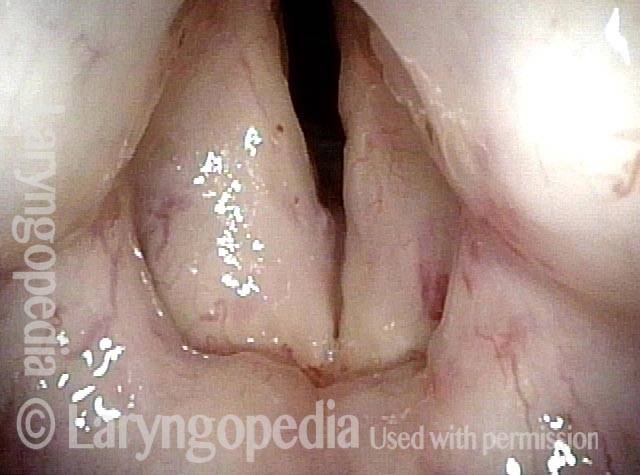
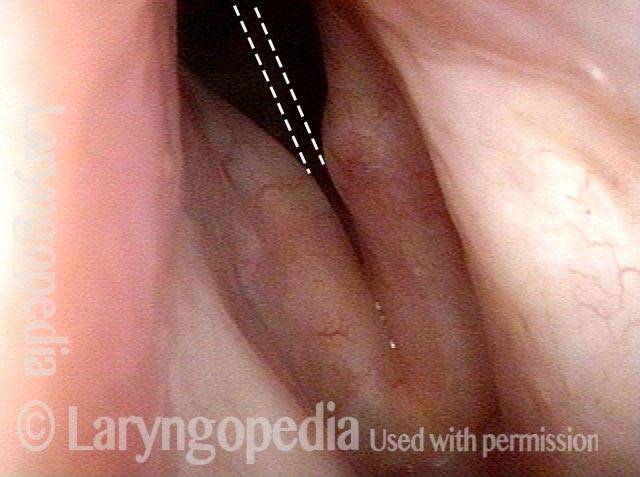
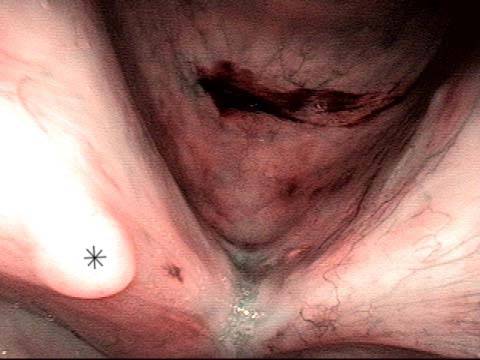
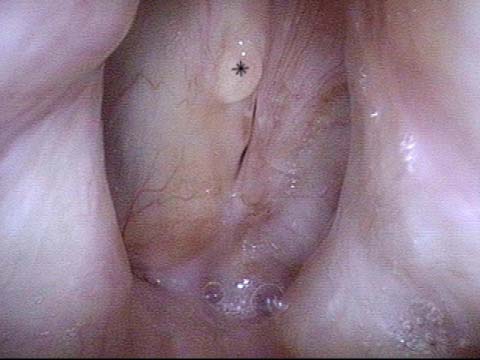
Nuances of Endotracheal Tube Injury
This woman with high-risk comorbidities of diabetes and obesity, was in ventilated in ICU more than a month for pulmonary complications of Covid-19 infection. She had an orotracheal tube in place for 3.5 weeks, and then a tracheotomy tube was placed. Now at her first visit a year later, she remains tracheotomy-dependent, and is told she has bilateral vocal cord paralysis (disproven in the following photo series).
Maximum glottic opening (1 of 8)

Undersurface mucosa indraws (2 of 8)

Phonation (3 of 8)

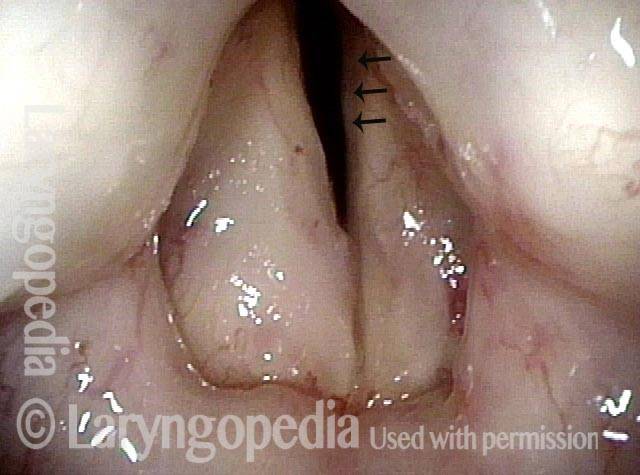
Posterior commissure divot (4 of 8)
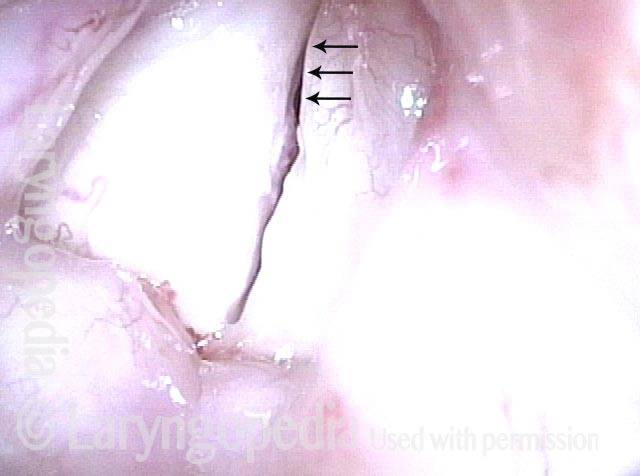
Further evidence of scarring (5 of 8)
View into trachea (6 of 8)
Vibration of trachea (7 of 8)

Open trachea beyond the tube (8 of 8)
The plan here is posterior commissuroplasty, followed by placement of a smaller trach tube and a trial of plugging. If plugging is tolerated during the day, she will need a sleep study with it plugged at night, given the tracheomalacia and her obesity.
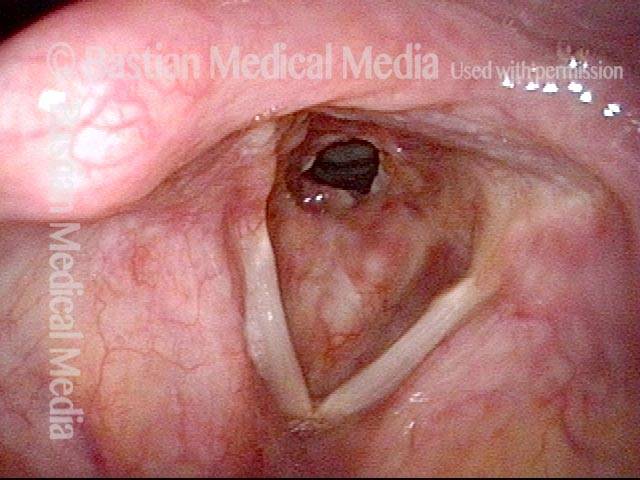
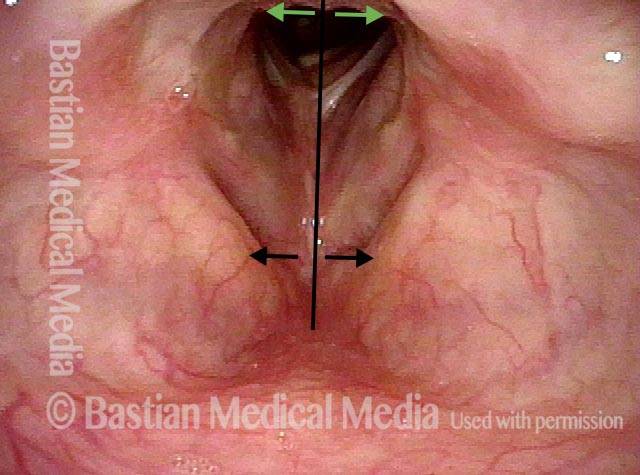
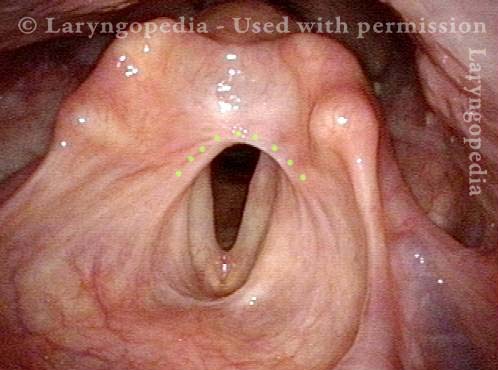
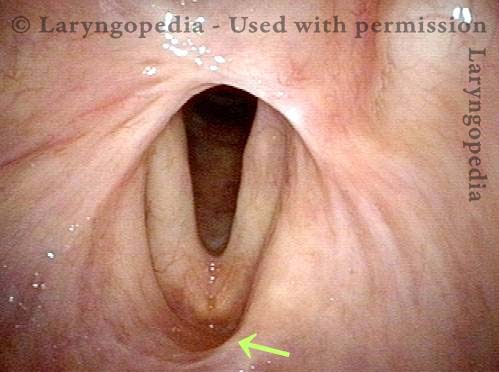
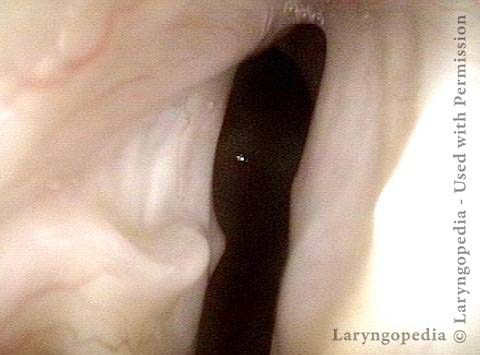
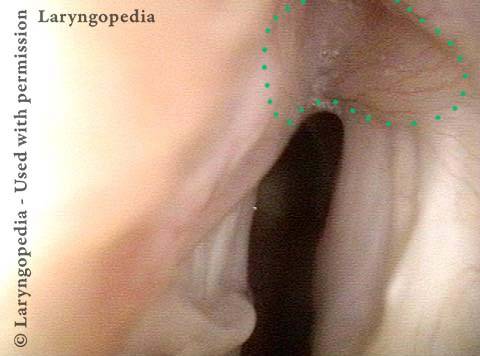
Breathing Tube Injury, not Vocal Cord Paralysis
This middle-aged woman was injured severely in an auto accident as a teenager. Recovery involved a long stay in ICU, and ventilation via a breathing (endotracheal) tube for a few weeks prior to tracheotomy.
Fifteen years earlier, a posterior commissuroplasty was done by me on the left side. Severely short of breath before that procedure, she said the improvement was such that she was able to do most activities of daily living remarkably well for many years.
While still much better than prior to the posterior commissuroplasty, she has felt a little more limited in the past few years and wants now another similar airway-widening procedure. Speaking voice can easily pass for normal, though she thinks it is occasionally a little rough.
Aperture is very narrow (1 of 6)

Involuntary inspiratory phonation (2 of 6)
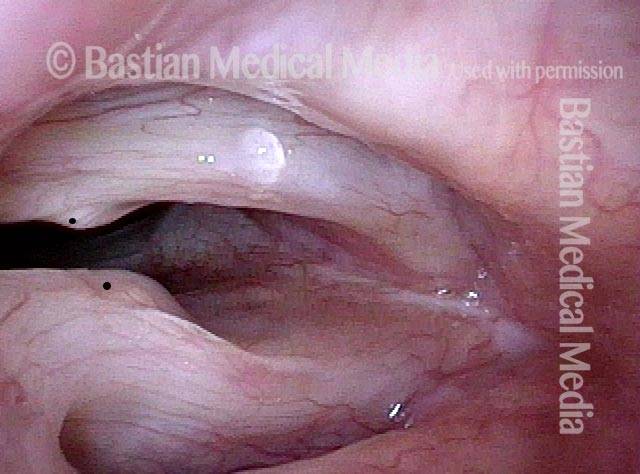
Divot on left vocal cord (3 of 6)

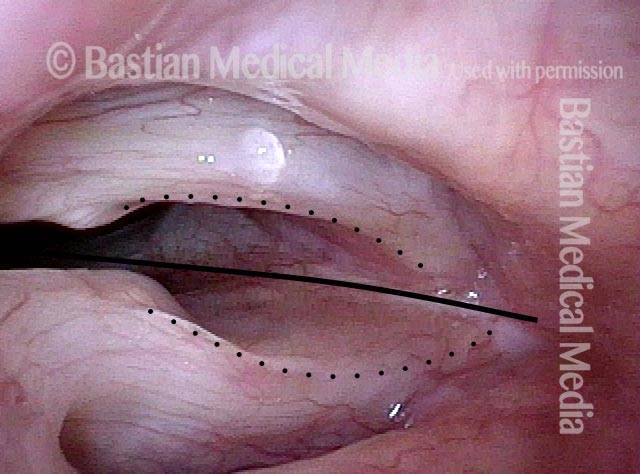
Endotracheal tube injury (4 of 6)
Laser cookie bite (5 of 6)
Surface scarring in the tracheotomy (6 of 6)