Lifting the CPM for a R-CPD Injection
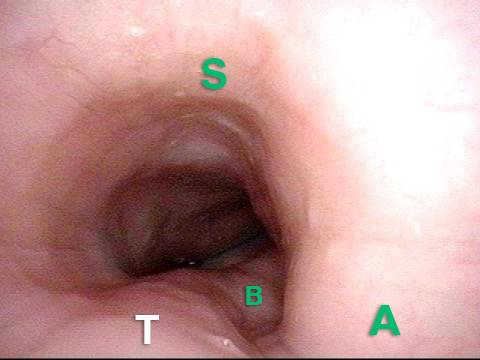
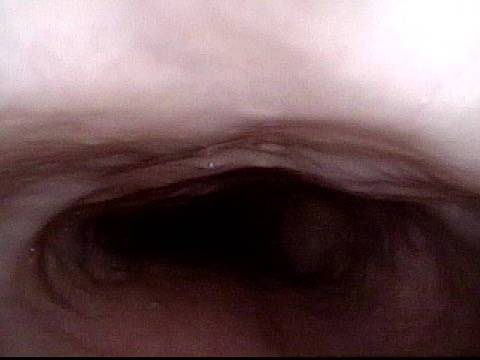
These are intra-operative photos of one of nearly 1500 persons treated for R-CPD as of September 2023. This sequence shows several things: The dilated, “always open” esophagus distal (below) the muscle; how to identify the cricopharyngeus muscle; and one way of injecting it.
Above the CPM (1 of 5)

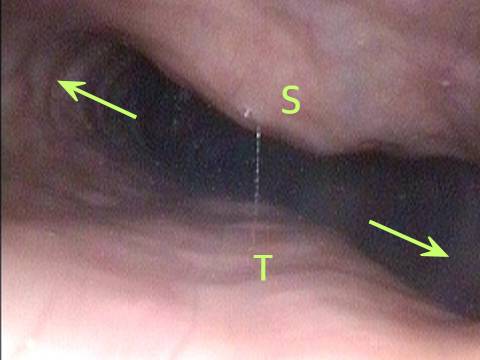
Ridge of the CPM (2 of 5)

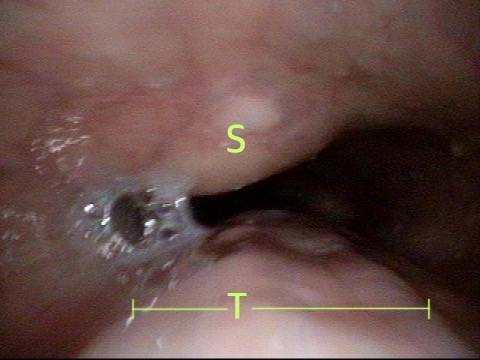
Exposed CPM ( 3 of 5)

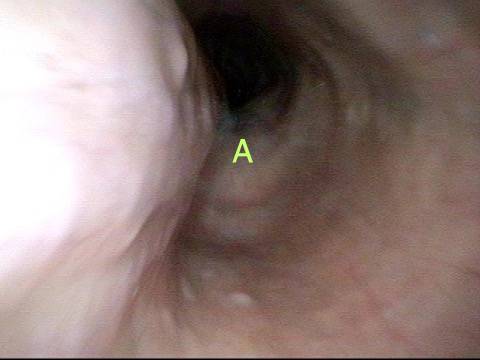
CPM Palpated ( 4 of 5)

Botox injection ( 5 of 5)

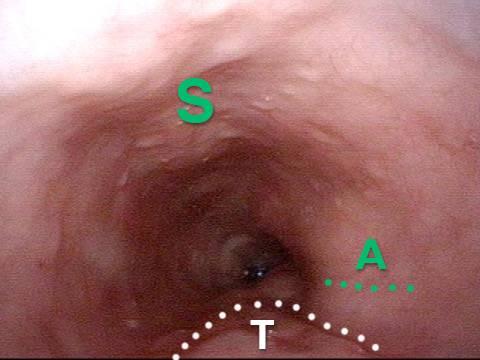
¿Dónde está el músculo cricofaríngeo?
Cricopharyngeus Muscle (1 of 3)
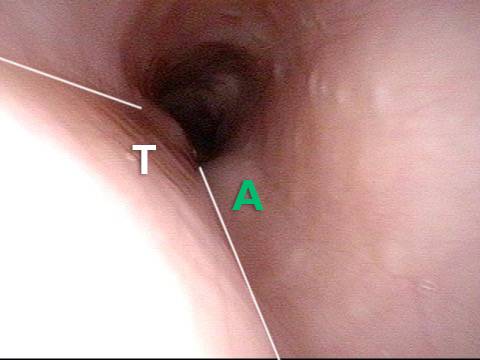
Open Cricopharyngeus Muscle (2 of 3)
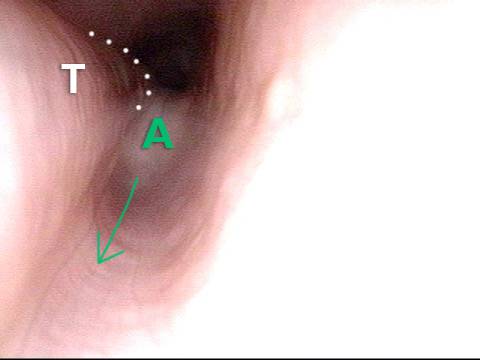
Closed (3 of 3)
Hallazgos Esofágicos
Aortic shelf (1 of 3)
Bony spur emerges due to stretched esophagus (2 of 3)

Stretched esophagus due to unburpable air (3 of 3)
Distensión Abdominal de R-CPD
Gastric Air Bubble (1 of 3)
Bloated Abdomen (2 of 3)

Non-bloated Abdomen (3 of 3)

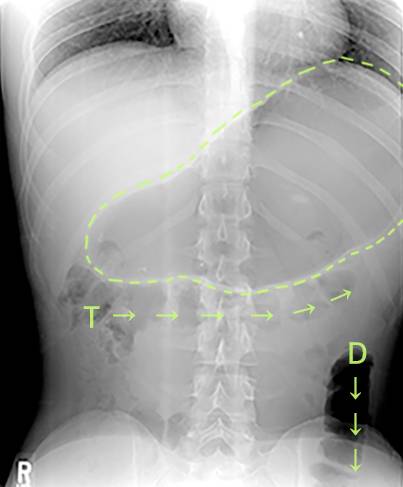
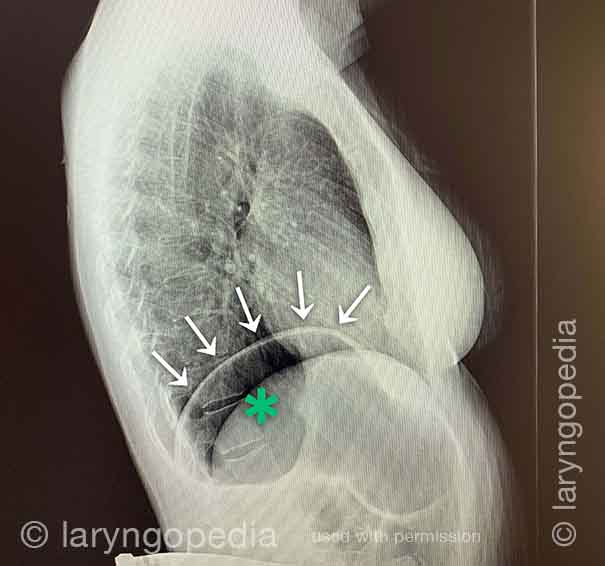
Una Rara «crisis abdominal» Debido a R-CPD (incapacidad para eructar)
X-Ray of Abdominal Bloating (1 of 2)
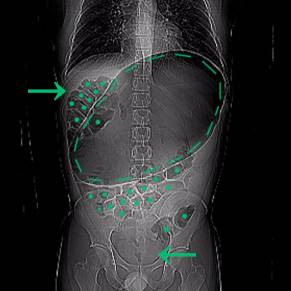
Original X-Ray (2 of 2)

No puedo eructar: Progresión de la hinchazón y la distensión abdominal; Un ciclo diario para muchos con R-CPD
Esta joven tiene los síntomas clásicos de R-CPD: el síndrome de no poder eructar. Temprano en el día, sus síntomas son mínimos y el abdomen está en la «línea de base» porque se ha «desinflado» a través de la flatulencia durante la noche. En esta serie se ve la diferencia en su distensión abdominal entre temprano y tarde en el día. Las imágenes de rayos X muestran la notable cantidad de aire retenido que explica su hinchazón y distensión. Su progresión es bastante típica; algunos con R-CPD se distienden incluso más de lo que se muestra aquí, especialmente después de comer una comida copiosa o consumir algo carbonatado.
Side view of a bloated abdomen (1 of 6)

Front view (2 of 6)

Greater Distention (3 of 6)

Front view of bloating stomach (4 of 6)

X-ray of trapped air (5 of 6)
Side view (6 of 6)
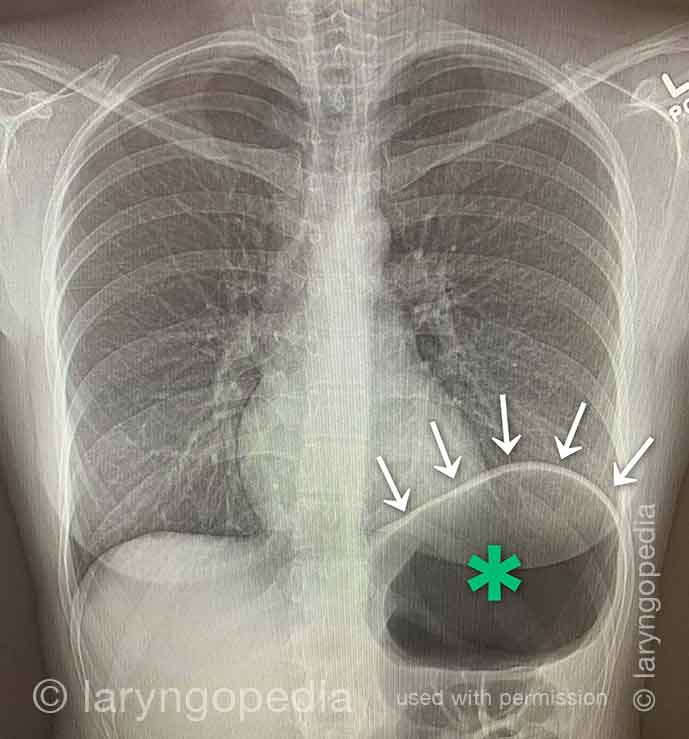
Dificultad para Respirar Causada por no Eructar (R-CPD)
Las personas que no pueden eructar y tienen el síndrome R-CPD completo a menudo dicen que cuando la hinchazón y la distensión son particularmente malas, y especialmente cuando tienen una sensación de presión en el pecho, también tienen una sensación de dificultad para respirar. Dirán, por ejemplo, “Soy un [cantante, o corredor, o ciclista o _____], pero mi habilidad está muy disminuida por R-CPD. Si estoy compitiendo o actuando, no puedo comer ni beber durante las 6 horas anteriores”. Algunos incluso dicen que no pueden completar un bostezo cuando los síntomas son particularmente graves. Las radiografías a continuación explican cómo la incapacidad para eructar puede causar dificultad para respirar.
X-ray of trapped air (1 of 2)
Side view (2 of 2)
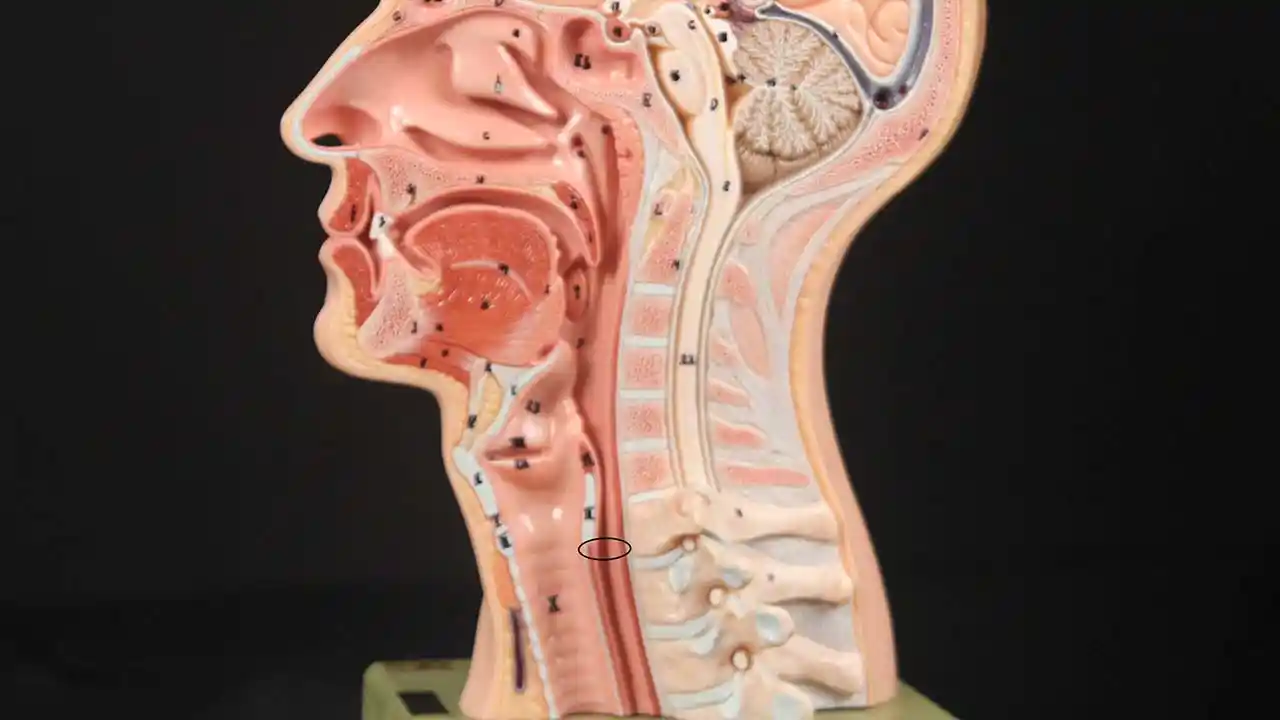
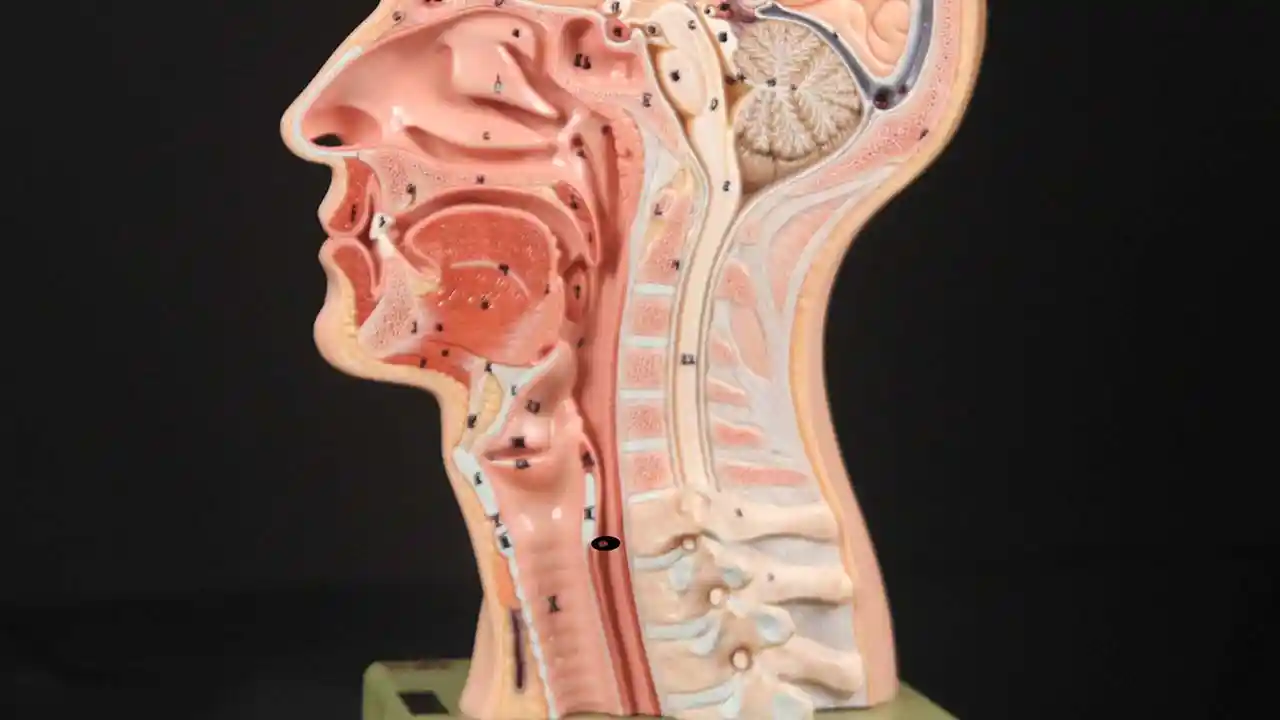
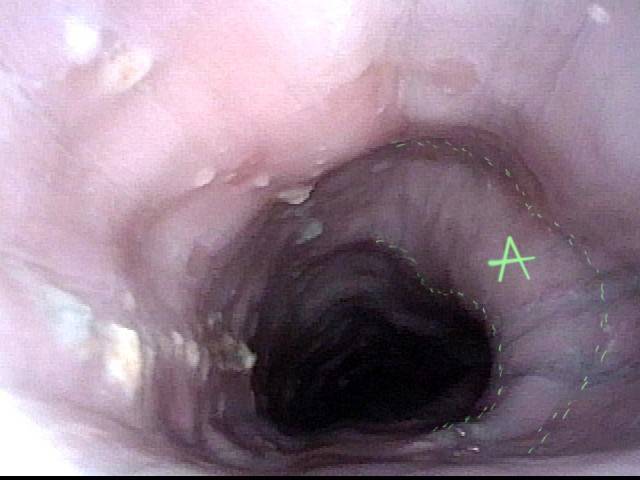
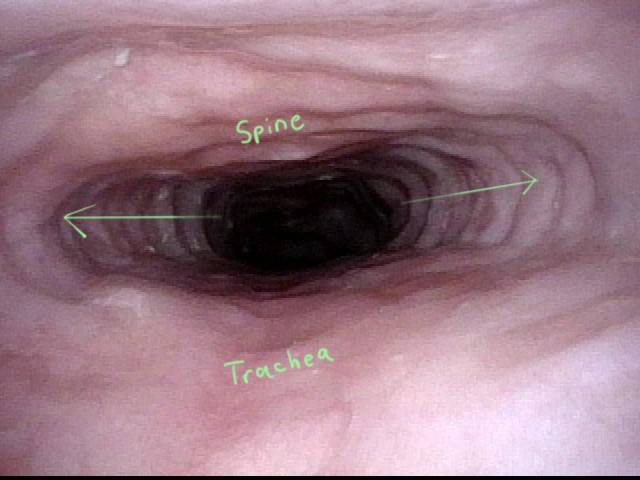
Hallazgos Esofágicos más Interesantes de R-CPD (incapacidad para eructar)
Stretched Esophagus (1 of 4)
Tracheal Wall (2 of 4)
Over-dilation (3 of 4)
Bronchus (4 of 4)
Dramática Dilatación Lateral del Esófago Superior
Remarkable lateral dilation (1 of 3)
Dilated upper esophagus (2 of 3)
Aortic shelf (3 of 3)
Cómo Puede Verse el Esófago «debajo de un eructo”
Baseline (1 of 3)

Pre-burp (2 of 3)
Post-burp (3 of 3)